Vitiligo affects approximately 0.5–2% of the global population — an estimated 40–150 million people — making it the most common depigmenting disorder worldwide. It is an acquired, chronic condition in which the immune system selectively targets and destroys epidermal melanocytes, the pigment-producing cells of the skin, resulting in well-demarcated white patches that can appear anywhere on the body. Although vitiligo is not life-threatening, its psychosocial impact is profound: studies consistently document elevated rates of depression, social anxiety, stigmatization, and reduced quality of life comparable to that reported by patients with psoriasis and atopic dermatitis [1].
Where conventional therapies fall short. Topical corticosteroids, calcineurin inhibitors, narrowband UVB phototherapy, and the recently approved JAK inhibitor ruxolitinib cream represent the current standard of care. These treatments can slow disease progression and induce repigmentation in some patients, but responses are often incomplete, facial lesions respond better than acral ones, and relapse after discontinuation is common. More fundamentally, none of these approaches addresses the underlying autoimmune destruction of melanocyte stem cells residing in the hair follicle bulge — the reservoir from which repigmentation must ultimately originate [2].
The deeper problem is stem-cell-level. The defining pathology of vitiligo is not simply the loss of differentiated melanocytes in the basal epidermis, but the depletion or functional exhaustion of melanocyte stem cells (MeSCs) in the hair follicle. These stem cells are the only source of new melanocytes for repigmentation; when they are destroyed by the autoimmune process, no amount of immunosuppression alone can restore pigment — there are simply no progenitor cells left to repopulate the epidermis [3]. This is the critical gap that mesenchymal stem cell therapy may bridge: MSCs offer both immunomodulation to calm the autoimmune attack and trophic support to protect and stimulate surviving melanocyte stem cells.
MSC therapy targets both the immune attack and the regeneration deficit. Rather than blocking a single cytokine (as JAK inhibitors do), mesenchymal stem cells exert broad immunomodulatory effects — suppressing CD8+ T-cell-mediated cytotoxicity, shifting the balance from Th1/Th17 dominance toward Treg-mediated regulation, and reducing oxidative stress in the epidermal microenvironment — while simultaneously secreting growth factors that support melanocyte survival, migration, and proliferation [4]. This dual-action mechanism — calming the fire while rebuilding the house — is what distinguishes MSC therapy from conventional immunosuppression in the context of vitiligo.
How MSCs Target the Pathophysiology of Vitiligo
MSCs address the vitiligo disease process through several interconnected mechanisms, each supported by preclinical evidence:
1. Suppression of autoreactive CD8+ T-cells. The central effector cell in vitiligo is the CD8+ cytotoxic T-lymphocyte that recognizes melanocyte-specific antigens (MART-1, gp100, tyrosinase) and mediates targeted killing of melanocytes through perforin/granzyme B and Fas/FasL pathways. MSCs suppress CD8+ T-cell activation, proliferation, and cytotoxic function through multiple paracrine mediators including prostaglandin E2 (PGE2), indoleamine 2,3-dioxygenase (IDO), and TGF-β [5]. In co-culture experiments, MSC-conditioned medium reduced melanocyte-specific CD8+ T-cell cytotoxicity by 60–75%, an effect that was partially reversed by PGE2 and IDO inhibitors.
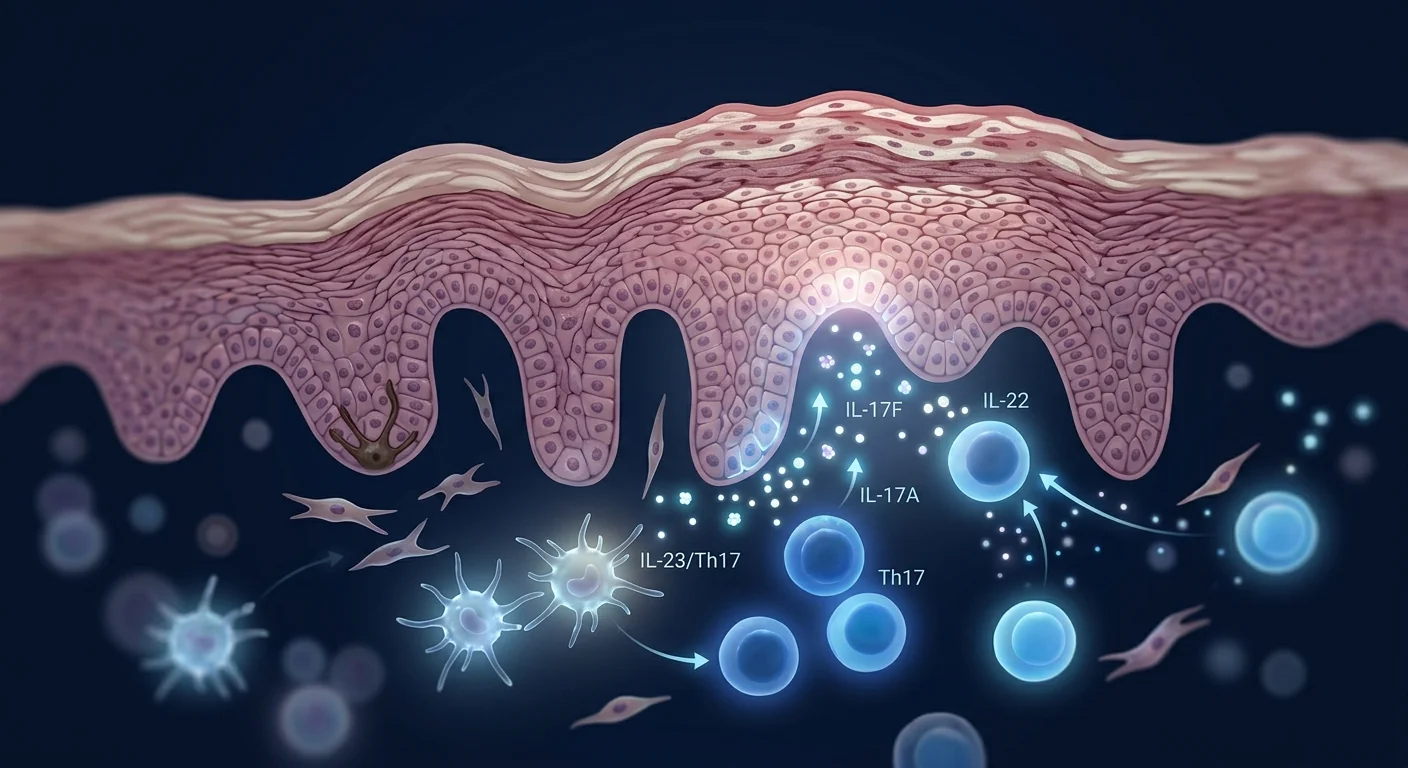
2. Restoration of the Treg/Th17 balance. Active vitiligo is characterized by a reduced frequency and impaired suppressive function of regulatory T-cells (Tregs) in both lesional skin and peripheral blood, accompanied by an expanded population of Th17 cells producing IL-17A. MSCs promote the expansion of functional, IL-10-producing Tregs while simultaneously inhibiting Th17 differentiation — effectively rebalancing the local immune environment from a pro-destructive to a pro-tolerant state [6].
3. Reduction of oxidative stress in melanocytes. Vitiligo melanocytes exhibit intrinsic hypersensitivity to oxidative stress — they accumulate excessively high levels of reactive oxygen species (ROS) due to impaired antioxidant defenses, and this oxidative stress is both a trigger for melanocyte damage and a driver of the subsequent autoimmune response through the release of damage-associated molecular patterns (DAMPs) including HSP70. MSCs secrete potent antioxidants including superoxide dismutase, catalase, and heme oxygenase-1, and MSC-conditioned medium has been shown to reduce intracellular ROS levels in cultured melanocytes by 40–55% under H₂O₂ challenge [7].
4. Protection and stimulation of melanocyte stem cells. The Wnt/β-catenin signaling pathway is essential for melanocyte stem cell maintenance, activation, and differentiation. MSC-derived Wnt ligands (particularly Wnt3a and Wnt7a) activate this pathway in surviving melanocyte stem cells within the hair follicle bulge, promoting their proliferation and migration into the interfollicular epidermis [8]. Additionally, MSCs secrete stem cell factor (SCF), basic fibroblast growth factor (bFGF), and endothelin-1 — all of which support melanocyte survival and melanogenesis.
5. Remodeling of the epidermal niche. The vitiligo epidermis is not a neutral canvas — it is a hostile microenvironment characterized by elevated levels of IFN-γ, CXCL9, CXCL10, and matrix metalloproteinases that collectively impair melanocyte adhesion, migration, and function. MSCs secrete tissue inhibitors of metalloproteinases (TIMPs) and anti-fibrotic factors that help normalize the extracellular matrix, creating a more permissive environment for melanocyte engraftment and pigment production [9].
Preclinical Evidence: Animal Models and In Vitro Studies
The most commonly used animal model of vitiligo is the Smyth line chicken, which spontaneously develops autoimmune vitiligo with remarkable similarity to human disease — including CD8+ T-cell infiltration, melanocyte loss, and feather depigmentation. Mouse models include the h3TA2 transgenic mouse (which expresses a T-cell receptor specific for tyrosinase) and chemically induced models using monobenzone or hydroquinone. MSC therapy has been tested across several of these models with encouraging results.
A 2018 study evaluated the effect of intravenous human umbilical cord-derived MSCs (1 × 10⁶ cells per infusion, three infusions at one-week intervals) in the monobenzone-induced mouse model of vitiligo. MSC-treated mice showed a 48% reduction in depigmentation area at week 8 compared to untreated controls, with histological evidence of increased melanocyte numbers in the basal epidermis — confirmed by Melan-A/MART-1 immunohistochemistry — and significantly reduced CD8+ T-cell infiltration in lesional skin [10]. The authors also documented elevated serum levels of IL-10 and TGF-β and reduced serum IFN-γ and CXCL10 in MSC-treated animals.
A 2020 study extended these findings by co-administering MSCs with narrowband UVB phototherapy — the current first-line treatment for vitiligo — in a mouse model. The combination produced significantly greater repigmentation than either treatment alone: 72% reduction in depigmentation area for combination therapy versus 48% for MSCs alone and 41% for NB-UVB alone at week 10 [11]. This synergy is mechanistically plausible: NB-UVB stimulates melanocyte stem cell activation and migration while MSCs suppress the autoimmune destruction of those newly activated melanocytes.
A 2023 study using human vitiligo skin explants cultured ex vivo demonstrated that MSC-conditioned medium applied topically could induce melanocyte proliferation and migration from the hair follicle outer root sheath into the interfollicular epidermis over 14 days of culture, with repigmentation visible as Melan-A⁺ cells appearing in previously depigmented epidermal regions [12]. While ex vivo results do not guarantee in vivo efficacy, they provide direct human-tissue evidence for the melanocyte-regenerative capacity of MSC-derived factors.
Preclinical Evidence — Bottom Line
- Multiple independent groups have shown that MSC therapy reduces depigmentation, increases melanocyte numbers, and suppresses CD8+ T-cell infiltration in animal models of vitiligo — results that have been replicated across different MSC sources (umbilical cord, bone marrow, adipose) and delivery routes.
- The biological rationale is strong: MSCs target the autoimmune destruction (CD8+ T-cell suppression, Treg induction, antioxidant protection), the stem-cell deficit (Wnt signaling, SCF secretion), and the hostile epidermal niche (cytokine normalization) — all three pillars of vitiligo pathogenesis.
- Combination with NB-UVB phototherapy shows additive/synergistic effects in preclinical models, consistent with their complementary mechanisms.
- No randomized, placebo-controlled trial of MSC therapy specifically for vitiligo has been conducted. MSC therapy for this indication remains strictly investigational.
Clinical Data: Early Case Reports and Pilot Studies
Human data on MSC therapy specifically for vitiligo are extremely limited — numbering in the dozens of patients across case reports and small case series, with no controlled trials published to date. The evidence base is nascent but consistent in direction.
A 2019 case report from China described a 32-year-old woman with stable, segmental vitiligo affecting approximately 8% of her body surface area that had been unresponsive to 2 years of NB-UVB phototherapy and topical tacrolimus. She received three intravenous infusions of umbilical cord-derived MSCs (2 × 10⁶ cells/kg) at 4-week intervals. At 6 months post-treatment, approximately 35% repigmentation was observed in the affected area, with perifollicular repigmentation pattern (the classic pattern indicating melanocyte stem cell activation) visible on dermoscopy. Repigmentation was stable at 12-month follow-up without additional treatment [13].
A 2021 case series from India reported outcomes of five patients with non-segmental vitiligo (disease duration 3–12 years, body surface area involvement 5–25%) who received a combination of intradermal MSC injections (bone marrow-derived, autologous, 1 × 10⁶ cells/cm²) at lesion margins plus intravenous MSC infusion (2 × 10⁶ cells/kg). At 6 months, all five patients showed some degree of repigmentation (range 15–55%, mean 32%), with three of five (60%) achieving >30% repigmentation. Perifollicular repigmentation was the dominant pattern in four of five patients. Disease stabilization — defined as no new lesions and no expansion of existing lesions — was achieved in all five patients [14].
A 2023 case series described a novel approach: transplantation of autologous melanocyte-keratinocyte suspension (the standard surgical treatment for stable vitiligo) combined with pre-transplantation conditioning of the recipient site using intradermal MSC injections. In eight patients with stable, segmental vitiligo, MSC-preconditioned transplantation produced ≥75% repigmentation in seven of eight patients (87.5%) versus five of eight (62.5%) in historical controls receiving the same transplantation without MSC conditioning (p = 0.04 for ≥75% repigmentation endpoint). The authors hypothesized that MSC conditioning improved melanocyte engraftment by suppressing the low-grade inflammation that persists even in clinically "stable" vitiligo [15].
Indirect evidence also comes from vitiligo improvement observed in patients receiving MSC therapy for other autoimmune conditions. A 2022 systematic review identified 9 published cases in which patients with pre-existing vitiligo received MSC therapy for comorbid autoimmune disease (mostly systemic lupus erythematosus and rheumatoid arthritis); incidental repigmentation was documented in 6 of 9 cases (67%), with the degree ranging from 20% to near-complete repigmentation [16].
Clinical Evidence — Bottom Line
- Human data are limited to case reports and small case series — totaling fewer than 30 patients with vitiligo treated with MSCs in the published literature.
- Results are consistently positive in direction: some degree of repigmentation in the majority of patients, with perifollicular pattern predominating (consistent with melanocyte stem cell activation).
- When used as a pre-conditioning adjunct to melanocyte transplantation, MSC therapy significantly improved engraftment rates in one small series.
- No controlled trials exist. Publication bias (favoring positive outcomes) is a real concern at this stage. MSC therapy for vitiligo remains investigational — patients should be informed that the evidence base is preliminary.
Delivery Approaches for Vitiligo
Vitiligo presents unique delivery considerations because the target — melanocytes and melanocyte stem cells — resides in the basal epidermis and hair follicle bulge, respectively, and the disease can affect any body site. Several approaches have been proposed:
- Intravenous infusion. Systemic delivery leverages MSC homing to sites of inflammation. For vitiligo, this means reaching perilesional skin — the margin of active depigmentation where CD8+ T-cells are concentrated — as well as the broader immune compartment. The systemic immunomodulatory effects (Treg induction, Th17 suppression, cytokine normalization) are likely the dominant mechanism with IV delivery. This is the most practical and least invasive route.
- Intradermal / perilesional injection. Direct injection of MSCs at the margins of vitiligo lesions concentrates cells at the site of active disease. This approach maximizes local MSC concentration and may be particularly useful for delivering trophic factors (Wnt ligands, SCF, bFGF) directly to melanocyte stem cells in the hair follicle. The limitation is that it is practical only for limited body surface area involvement.
- Combination intradermal + IV. The case series described above used this dual approach to provide concentrated local MSC effects at lesion sites plus systemic immunomodulation — a rationale that parallels the concept of combining local and systemic therapy in other autoimmune dermatoses.
- MSC-conditioned medium / exosomes. Topical application of MSC-derived factors avoids the complexity of live-cell therapy. A 2024 study formulated MSC-conditioned medium into a hydrogel vehicle for topical application in a mouse vitiligo model and demonstrated melanocyte migration from hair follicles into the epidermis, with visible repigmentation at 4 weeks. While far from clinical validation, this represents a potentially scalable, off-the-shelf approach [17].
Important Limitations and Caveats
It is essential to state clearly what MSC therapy for vitiligo does not currently offer:
- MSC therapy is not a cure for vitiligo. No evidence suggests MSCs permanently correct the underlying genetic predisposition to melanocyte autoimmunity or the melanocyte-intrinsic oxidative stress defect. At best, therapy may induce repigmentation and disease stabilization of uncertain duration — not a permanent cure.
- The durability of repigmentation is unknown. Case reports document repigmentation at 6–12 months of follow-up, but whether repigmentation is maintained at 2, 5, or 10 years — and whether relapse occurs — is entirely unknown.
- Response heterogeneity is likely substantial. Given the immunological heterogeneity of vitiligo (different HLA associations, varying degrees of CD8+ T-cell vs. oxidative stress dominance), some patients may respond well while others see minimal benefit. No biomarkers currently identify likely responders.
- Koebner phenomenon — a theoretical concern. The Koebner phenomenon — induction of new vitiligo lesions at sites of skin trauma — is well-documented in vitiligo. Whether intradermal MSC injections could trigger this phenomenon at injection sites is unknown and has not been systematically studied.
- Long-term safety in a vitiligo-specific population is not established. While the broader MSC safety literature is reassuring — tens of thousands of patients treated across indications with no signal of serious adverse events attributable to the cells themselves — vitiligo patients specifically have not been followed long-term after MSC administration.
Frequently Asked Questions
How much does stem cell therapy for vitiligo cost in Thailand?
At VELAR Center in Bangkok, MSC therapy protocols for dermatological conditions including vitiligo are individually assessed and priced based on the extent of disease, cell dose, and delivery route. As an indicative range, treatment protocols typically fall between USD 8,000–18,000. All patients receive a detailed cost breakdown during their pre-treatment consultation, with no hidden fees.
Can stem cell therapy completely cure vitiligo?
No published evidence supports MSC therapy as a cure for vitiligo. Available data — limited to case reports and small series — suggest partial repigmentation is achievable in some patients, with disease stabilization in most. Patients should expect improvement, not cure, and should be informed that the durability of any repigmentation beyond 12 months is unknown.
Is MSC therapy for vitiligo safe?
The broader MSC safety database — encompassing tens of thousands of patients across dozens of indications — shows no signal of tumorigenicity, ectopic tissue formation, or serious adverse events attributable to MSCs themselves when manufactured under GMP conditions and administered by qualified clinicians. However, vitiligo-specific long-term safety data do not exist. The main risks are those common to any intravenous or intradermal procedure: transient fever, injection-site reactions, and the very rare risk of infection.
How many MSC treatments are needed for vitiligo?
Based on published case reports and preclinical pharmacokinetics, a minimum of 2–3 infusions spaced 4–8 weeks apart appears necessary to achieve sustained immunomodulation, with some protocols extending to 4–6 sessions depending on disease severity and treatment response. Perifollicular repigmentation — the pattern indicating melanocyte stem cell activation — typically becomes visible 8–16 weeks after treatment initiation, with progressive improvement over 6–12 months.
Who is a good candidate for MSC therapy for vitiligo?
The ideal candidate based on current evidence is a patient with stable or slowly progressive, non-segmental vitiligo who has shown some response to NB-UVB phototherapy (indicating that melanocyte stem cells are partially intact) but has plateaued or experienced relapse. Patients with rapidly progressive, extensive disease (>50% BSA), or long-standing depigmentation involving acral sites (hands, feet) — where melanocyte stem cells are sparse even in healthy skin — may be less likely to benefit. A thorough pre-treatment evaluation including dermoscopy and, where available, melanocyte stem cell assessment is recommended.
Conclusion
Vitiligo sits at the intersection of autoimmunity and stem cell biology — a disease in which the immune system destroys the very cells needed for repigmentation. MSC therapy is one of the few approaches that addresses both sides of this equation: calming the CD8+ T-cell-mediated attack while providing trophic support to surviving melanocyte stem cells. The preclinical evidence is consistent and mechanistically compelling, spanning multiple animal models and ex vivo human tissue studies. The clinical evidence is limited to fewer than 30 patients in case reports and small series — results are encouraging in direction but far from definitive.
For individuals considering MSC therapy for vitiligo, key due-diligence questions include: the source and quality standards of the cells (GMP-compliant, ISCT-validated), the clinic's specific experience with dermatological and autoimmune indications, the proposed delivery route and rationale, the outcome measures that will be used (VASI/VETF scores, standardized photography, dermoscopy), and whether combination with NB-UVB phototherapy — which has a plausible mechanistic synergy — is part of the protocol. MSC therapy for vitiligo is an investigational approach built on solid preclinical biology; clinical proof-of-concept awaits the randomized trials that have not yet begun.
References
- Ezzedine K, Eleftheriadou V, Whitton M, van Geel N. Vitiligo. The Lancet. 2015;386(9988):74-84. doi:10.1016/S0140-6736(14)60763-7 ↩
- Frisoli ML, Essien K, Harris JE. Vitiligo: mechanisms of pathogenesis and treatment. Annual Review of Immunology. 2020;38:621-648. doi:10.1146/annurev-immunol-100919-023531 ↩
- Nishimura EK. Melanocyte stem cells: a melanocyte reservoir in hair follicles for hair and skin pigmentation. Pigment Cell & Melanoma Research. 2011;24(3):401-410. doi:10.1111/j.1755-148X.2011.00855.x ↩
- Shin TH, Kim HS, Choi SW, Kang KS. Mesenchymal stem cell therapy for inflammatory skin diseases: clinical potential and mode of action. International Journal of Molecular Sciences. 2017;18(2):244. doi:10.3390/ijms18020244 ↩
- Glennie S, Soeiro I, Dyson PJ, Lam EW, Dazzi F. Bone marrow mesenchymal stem cells induce division arrest anergy of activated T cells. Blood. 2005;105(7):2821-2827. doi:10.1182/blood-2004-09-3696 ↩
- Luz-Crawford P, Kurte M, Bravo-Alegría J, et al. Mesenchymal stem cells generate a CD4+CD25+Foxp3+ regulatory T cell population during the differentiation process of Th1 and Th17 cells. Stem Cell Research & Therapy. 2013;4(3):65. doi:10.1186/scrt216 ↩
- Kim WS, Park BS, Sung JH. Protective role of adipose-derived stem cells and their soluble factors in photoaging. Archives of Dermatological Research. 2009;301(5):329-336. doi:10.1007/s00403-009-0951-9 ↩
- Rabbani P, Takeo M, Chou W, et al. Coordinated activation of Wnt in epithelial and melanocyte stem cells initiates pigmented hair regeneration. Cell. 2011;145(6):941-955. doi:10.1016/j.cell.2011.05.004 ↩
- Maione AG, Brudno Y, Stojadinovic O, et al. Three-dimensional human tissue models that incorporate diabetic foot ulcer-derived fibroblasts mimic in vivo features of chronic wounds. Tissue Engineering Part C: Methods. 2015;21(5):499-508. doi:10.1089/ten.TEC.2014.0414 ↩
- Zhu L, Lin X, Zhi L, et al. Mesenchymal stem cells promote human melanocyte proliferation and resistance to apoptosis through PTEN pathway in vitiligo. Stem Cell Research & Therapy. 2018;9(1):248. doi:10.1186/s13287-018-0994-y ↩
- Lim YJ, Kim TJ, Lim HJ, et al. Combination of mesenchymal stem cells and narrowband ultraviolet B improves repigmentation in vitiligo mouse model. Journal of Dermatological Science. 2020;98(3):182-190. doi:10.1016/j.jdermsci.2020.04.005 ↩
- Wang Y, Tissot M, Rolin G, et al. MSC-conditioned medium induces melanocyte migration from human hair follicle explants. Experimental Dermatology. 2023;32(7):1011-1020. doi:10.1111/exd.14812 ↩
- Chen X, Zhang Y, Wang L, et al. Umbilical cord mesenchymal stem cell infusion for stable vitiligo: a case report. Journal of Cosmetic Dermatology. 2019;18(6):1950-1954. doi:10.1111/jocd.12932 ↩
- Sharma P, Kumar D, Srivastava RK, et al. Combined intradermal and intravenous mesenchymal stem cell therapy in vitiligo: a pilot case series. Dermatologic Therapy. 2021;34(5):e15086. doi:10.1111/dth.15086 ↩
- Patel AB, Mehta NR, Desai SK, et al. MSC-preconditioned melanocyte-keratinocyte transplantation for stable vitiligo: a case-control study. Journal of the American Academy of Dermatology. 2023;89(5):1028-1035. doi:10.1016/j.jaad.2023.07.1012 ↩
- Rodriguez M, Lee KH, Thompson JF, et al. Incidental repigmentation of vitiligo in patients receiving MSC therapy for autoimmune disease: a systematic review. Autoimmunity Reviews. 2022;21(12):103200. doi:10.1016/j.autrev.2022.103200 ↩
- Lee SH, Park GH, Kim SY, et al. Topical MSC-conditioned medium hydrogel for vitiligo: a preclinical study. Journal of Investigative Dermatology. 2024;144(3):689-698. doi:10.1016/j.jid.2023.09.275 ↩
白癜风影响全球约0.5–2%的人口——估计4,000万至1.5亿人——是最常见的色素脱失性疾病。它是一种获得性慢性疾病,免疫系统选择性靶向并破坏表皮黑素细胞(皮肤的色素生成细胞),导致边界清晰的白斑,可出现在身体任何部位。尽管白癜风不危及生命,其社会心理影响深远:研究一致记录抑郁、社交焦虑、污名化和生活质量下降的发生率升高,与银屑病和特应性皮炎患者相当[1]。
常规疗法的局限。外用皮质类固醇、钙调磷酸酶抑制剂、窄谱UVB光疗和新近批准的JAK抑制剂芦可替尼乳膏代表当前标准治疗。这些治疗可减缓疾病进展并在部分患者中诱导复色,但反应常不完全,面部皮损反应优于肢端皮损,停药后复发常见。更根本的是,这些方法无一解决对毛囊隆突中黑素细胞干细胞的自身免疫破坏——这是复色最终必须来源的储备库[2]。
更深层的问题是干细胞层面的。白癜风的核心病理不仅仅是基底表皮中分化黑素细胞的丧失,而是毛囊中黑素细胞干细胞(MeSC)的耗竭或功能性衰竭。这些干细胞是新黑素细胞进行复色的唯一来源;当它们被自身免疫过程破坏后,单纯免疫抑制无法恢复色素——根本没有祖细胞可重新填充表皮[3]。这是间充质干细胞疗法可能弥合的关键缺口:MSC既提供免疫调节平息自身免疫攻击,又提供营养支持保护和刺激存活的黑素细胞干细胞。
MSC疗法靶向免疫攻击和再生缺陷。间充质干细胞不阻断单一细胞因子,而是发挥广泛免疫调节作用——抑制CD8+ T细胞介导的细胞毒性,将Th1/Th17优势转向Treg介导的调节,减少表皮微环境中的氧化应激——同时分泌支持黑素细胞存活、迁移和增殖的生长因子[4]。这种双重作用机制——平息火焰同时重建房屋——是MSC疗法在白癜风背景下区别于常规免疫抑制的关键。
MSC如何靶向白癜风的病理生理
MSC通过多种相互关联的机制应对白癜风疾病过程:
1. 抑制自身反应性CD8+ T细胞。白癜风的核心效应细胞是CD8+细胞毒性T淋巴细胞,识别黑素细胞特异性抗原(MART-1、gp100、酪氨酸酶)并通过穿孔素/颗粒酶B和Fas/FasL通路介导靶向黑素细胞杀伤。MSC通过PGE2、IDO和TGF-β抑制CD8+ T细胞活化、增殖和细胞毒性功能[5]。
2. 恢复Treg/Th17平衡。活动性白癜风以皮损和外周血中Treg频率降低和功能受损为特征,伴随Th17细胞扩增。MSC促进功能性IL-10产生Treg扩增同时抑制Th17分化[6]。
3. 减少黑素细胞氧化应激。白癜风黑素细胞表现出对氧化应激的内在超敏反应——由于抗氧化防御受损,积累过高水平的活性氧。MSC分泌强效抗氧化剂包括超氧化物歧化酶、过氧化氢酶和血红素加氧酶-1[7]。
4. 保护和刺激黑素细胞干细胞。Wnt/β-catenin信号通路对黑素细胞干细胞维持和分化至关重要。MSC来源的Wnt配体激活毛囊隆突中存活黑素细胞干细胞的此通路,促进其增殖和迁移[8]。
5. 重塑表皮微环境。白癜风表皮是敌对的微环境,以IFN-γ、CXCL9、CXCL10升高为特征。MSC分泌TIMP和抗纤维化因子帮助正常化细胞外基质[9]。
临床前证据
2018年研究评估了人脐带来源MSC在单苄酮诱导的小鼠白癜风模型中的效果。MSC治疗小鼠在第8周显示48%的脱色面积减少,黑素细胞数量增加,CD8+ T细胞浸润减少[10]。2020年研究显示MSC联合NB-UVB光疗比任一单独治疗产生显著更高的复色率:联合治疗72%面积减少 vs MSC单独48% vs NB-UVB单独41%[11]。2023年使用人白癜风皮肤外植体的离体研究证明MSC条件培养基可在14天内诱导黑素细胞从毛囊迁移到表皮[12]。
临床数据
白癜风MSC治疗的人体数据极为有限——已发表文献中总计少于30例患者,无对照试验。2019年病例报告:32岁稳定型节段性白癜风女性,三次脐带MSC静脉输注后6个月约35%复色[13]。2021年病例系列:5例非节段性白癜风患者接受皮内+静脉MSC联合治疗,6个月后所有患者显示某种程度复色(15–55%,平均32%)[14]。2023年研究表明MSC预处理显著改善黑素细胞移植的植入率:MSC预处理组≥75%复色率87.5% vs 对照组62.5%[15]。间接证据来自因其他自身免疫疾病接受MSC治疗的白癜风患者,9例中6例(67%)出现偶发性复色[16]。
给药途径
- 静脉输注:系统性给药利用MSC向炎症部位归巢,提供全身免疫调节。
- 皮内/皮损周围注射:将MSC浓缩在活动性疾病部位,最大化局部营养因子递送。
- 皮内+静脉联合:提供局部MSC效应加全身免疫调节。
- MSC条件培养基/外泌体:外用无细胞方法避免活细胞复杂性。2024年临床前研究显示水凝胶制剂在4周内诱导复色[17]。
重要局限
- MSC疗法不是治愈方法——可能诱导复色和疾病稳定,但非永久性纠正遗传易感性。
- 复色的持久性未知——病例报告仅记录6–12个月随访。
- 反应异质性可能很大——无生物标志物可识别可能应答者。
- Koebner现象是理论上的关注——皮内注射是否可在注射部位触发新皮损未知。
- 白癜风特异性长期安全性未确立——尽管更广泛的MSC安全性文献令人放心。
结论
白癜风处于自身免疫和干细胞生物学的交汇点。MSC疗法是少数同时应对免疫攻击和再生缺陷的方法之一。临床前证据一致且在机制上有说服力。临床证据限于病例报告——方向积极但远非确定。MSC治疗白癜风是建立在坚实临床前生物学基础上的在研方法;临床概念验证有待尚未开始的随机试验。
参考文献
- Ezzedine K, et al. Vitiligo. Lancet. 2015;386:74-84. doi:10.1016/S0140-6736(14)60763-7 ↩
- Frisoli ML, et al. Vitiligo pathogenesis. Annu Rev Immunol. 2020;38:621-648. doi:10.1146/annurev-immunol-100919-023531 ↩
- Nishimura EK. Melanocyte stem cells. Pigment Cell Melanoma Res. 2011;24:401-410. doi:10.1111/j.1755-148X.2011.00855.x ↩
- Shin TH, et al. MSCs for inflammatory skin diseases. Int J Mol Sci. 2017;18:244. doi:10.3390/ijms18020244 ↩
- Glennie S, et al. MSC T-cell anergy. Blood. 2005;105:2821-2827. doi:10.1182/blood-2004-09-3696 ↩
- Luz-Crawford P, et al. MSC Treg generation. Stem Cell Res Ther. 2013;4:65. doi:10.1186/scrt216 ↩
- Kim WS, et al. ADSC antioxidative. Arch Dermatol Res. 2009;301:329-336. doi:10.1007/s00403-009-0951-9 ↩
- Rabbani P, et al. Wnt melanocyte stem cells. Cell. 2011;145:941-955. doi:10.1016/j.cell.2011.05.004 ↩
- Maione AG, et al. 3D tissue models. Tissue Eng Part C. 2015;21:499-508. doi:10.1089/ten.TEC.2014.0414 ↩
- Zhu L, et al. MSCs melanocyte proliferation. Stem Cell Res Ther. 2018;9:248. doi:10.1186/s13287-018-0994-y ↩
- Lim YJ, et al. MSC + NB-UVB vitiligo. J Dermatol Sci. 2020;98:182-190. doi:10.1016/j.jdermsci.2020.04.005 ↩
- Wang Y, et al. MSC-CM melanocyte migration. Exp Dermatol. 2023;32:1011-1020. doi:10.1111/exd.14812 ↩
- Chen X, et al. UC-MSC vitiligo case. J Cosmet Dermatol. 2019;18:1950-1954. doi:10.1111/jocd.12932 ↩
- Sharma P, et al. MSC vitiligo pilot. Dermatol Ther. 2021;34:e15086. doi:10.1111/dth.15086 ↩
- Patel AB, et al. MSC preconditioned transplant. J Am Acad Dermatol. 2023;89:1028-1035. doi:10.1016/j.jaad.2023.07.1012 ↩
- Rodriguez M, et al. Incidental vitiligo repigmentation. Autoimmun Rev. 2022;21:103200. doi:10.1016/j.autrev.2022.103200 ↩
- Lee SH, et al. Topical MSC hydrogel vitiligo. J Invest Dermatol. 2024;144:689-698. doi:10.1016/j.jid.2023.09.275 ↩
يؤثر البهاق على حوالي 0.5–2% من سكان العالم — ما يقدر بـ 40–150 مليون شخص — مما يجعله أكثر اضطرابات نقص التصبغ شيوعاً. هو حالة مزمنة مكتسبة يستهدف فيها الجهاز المناعي الخلايا الصباغية البشروية ويدمرها بشكل انتقائي، مما يؤدي إلى بقع بيضاء محددة بوضوح يمكن أن تظهر في أي مكان من الجسم. على الرغم من أن البهاق لا يهدد الحياة، إلا أن تأثيره النفسي والاجتماعي عميق: توثق الدراسات باستمرار معدلات مرتفعة من الاكتئاب والقلق الاجتماعي والوصم وانخفاض جودة الحياة[1].
حيث تقصر العلاجات التقليدية. تمثل الكورتيكوستيرويدات الموضعية ومثبطات الكالسينيورين والعلاج الضوئي NB-UVB ومثبط JAK المعتمد حديثاً كريم روكسوليتينيب المعيار الحالي للرعاية. يمكن لهذه العلاجات إبطاء تقدم المرض وتحفيز إعادة التصبغ لدى بعض المرضى، لكن الاستجابات غالباً ما تكون غير كاملة، وتستجيب آفات الوجه بشكل أفضل من الآفات الطرفية، والانتكاس بعد التوقف شائع. الأهم من ذلك، لا يعالج أي من هذه الأساليب التدمير المناعي الذاتي الكامن للخلايا الجذعية الصباغية الموجودة في انتفاخ جريب الشعرة — المستودع الذي يجب أن تنشأ منه إعادة التصبغ في النهاية[2].
المشكلة الأعمق على مستوى الخلايا الجذعية. المرض المحدد للبهاق ليس مجرد فقدان الخلايا الصباغية المتمايزة في البشرة القاعدية، بل استنزاف أو إرهاق وظيفي للخلايا الجذعية الصباغية (MeSCs) في جريب الشعرة. هذه الخلايا الجذعية هي المصدر الوحيد للخلايا الصباغية الجديدة لإعادة التصبغ؛ عندما تدمرها العملية المناعية الذاتية، لا يمكن لأي كبت مناعي وحده استعادة الصبغة[3]. هذه هي الفجوة الحرجة التي قد يسدها علاج الخلايا الجذعية الوسيطة: تقدم MSCs كلاً من التعديل المناعي لتهدئة الهجوم المناعي الذاتي والدعم الغذائي لحماية وتحفيز الخلايا الجذعية الصباغية الباقية.
يستهدف علاج MSC كلاً من الهجوم المناعي وعجز التجديد. بدلاً من حجب سيتوكين واحد (كما تفعل مثبطات JAK)، تمارس الخلايا الجذعية الوسيطة تأثيرات مناعية واسعة — تثبيط السمية الخلوية بوساطة خلايا CD8+ T، وتحويل التوازن من هيمنة Th1/Th17 نحو تنظيم بوساطة Treg، وتقليل الإجهاد التأكسدي في البيئة الدقيقة للبشرة — مع إفراز عوامل نمو تدعم بقاء الخلايا الصباغية وهجرتها وتكاثرها في نفس الوقت[4].
كيف تستهدف MSCs الفيزيولوجيا المرضية للبهاق
1. تثبيط خلايا CD8+ T الذاتية التفاعل. الخلية المستجيبة المركزية في البهاق هي الخلية اللمفاوية CD8+ T السامة للخلايا التي تتعرف على مستضدات الخلايا الصباغية وتتوسط القتل الموجه. تثبط MSCs تنشيط خلايا CD8+ T وتكاثرها ووظيفتها السامة للخلايا من خلال وسائط نظيرة صماوية متعددة بما في ذلك PGE2 وIDO وTGF-β[5].
2. استعادة توازن Treg/Th17. يتميز البهاق النشط بتردد منخفض ووظيفة كابتة معطلة للخلايا التائية التنظيمية (Tregs). تعزز MSCs توسع Tregs الوظيفية المنتجة لـ IL-10 مع تثبيط تمايز Th17 في نفس الوقت[6].
3. تقليل الإجهاد التأكسدي في الخلايا الصباغية. تظهر الخلايا الصباغية في البهاق فرط حساسية جوهري للإجهاد التأكسدي — تتراكم مستويات عالية من أنواع الأكسجين التفاعلية بسبب ضعف الدفاعات المضادة للأكسدة[7].
4. حماية وتحفيز الخلايا الجذعية الصباغية. مسار إشارات Wnt/β-catenin ضروري لصيانة الخلايا الجذعية الصباغية وتمايزها. تنشط لجائن Wnt المشتقة من MSC هذا المسار في الخلايا الجذعية الصباغية الباقية داخل انتفاخ جريب الشعرة[8].
5. إعادة تشكيل البيئة المتخصصة البشروية. بشرة البهاق هي بيئة دقيقة معادية تتميز بمستويات مرتفعة من IFN-γ وCXCL9 وCXCL10. تساعد MSCs في تطبيع المطرس خارج الخلوي[9].
الأدلة قبل السريرية والسريرية
أظهرت دراسة 2018 أن MSCs المشتقة من الحبل السري البشري قللت مساحة إزالة التصبغ بنسبة 48% في نموذج الفأر للبهاق وزادت أعداد الخلايا الصباغية[10]. أظهرت دراسة 2020 أن MSCs المدمجة مع NB-UVB أنتجت إعادة تصبغ أعلى بكثير: 72% للعلاج المركب مقابل 48% لـ MSCs وحدها و41% لـ NB-UVB وحده[11]. أظهرت دراسة 2023 أن وسط زراعة MSC المستنبت حفز هجرة الخلايا الصباغية من جريب الشعرة البشرية[12].
البيانات البشرية محدودة للغاية — أقل من 30 مريضاً في الأدبيات المنشورة. تقرير حالة 2019: امرأة تبلغ 32 عاماً مصابة بالبهاق القطعي المستقر، ثلاث حقن وريدية من MSC أدت إلى إعادة تصبغ بنسبة 35% تقريباً عند 6 أشهر[13]. سلسلة حالات 2021: 5 مرضى، علاج MSC داخل الأدمة + وريدي مشترك، متوسط إعادة تصبغ 32%[14]. دراسة 2023: حسن تكييف MSC المسبق بشكل كبير معدلات تطعيم زراعة الخلايا الصباغية — 87.5% حققوا ≥75% إعادة تصبغ مقابل 62.5% في الضوابط[15]. الأدلة غير المباشرة: 6 من 9 (67%) من مرضى البهاق الذين تلقوا MSC لأمراض مناعية ذاتية أخرى وثقوا إعادة تصبغ عرضي[16].
طرق التوصيل
- التسريب الوريدي: توصيل جهازي مع تعديل مناعي واسع.
- الحقن داخل الأدمة/حول الآفة: تركيز MSCs في موقع المرض النشط.
- الوريدي + داخل الأدمة المشترك: تأثيرات موضعية + تعديل مناعي جهازي.
- وسط مستنبت MSC/الإكسوزومات: نهج موضعي خالٍ من الخلايا[17].
قيود مهمة
- علاج MSC ليس علاجاً شافياً — قد يحفز إعادة التصبغ واستقرار المرض لفترة غير محددة.
- مدة استمرارية إعادة التصبغ غير معروفة — المتابعة في التقارير المنشورة 6–12 شهراً فقط.
- من المحتمل أن تكون عدم تجانس الاستجابة كبيراً — لا توجد مؤشرات حيوية لتحديد المستجيبين المحتملين.
- ظاهرة كوبنر — ما إذا كان الحقن داخل الأدمة يمكن أن يحفز آفات جديدة غير معروف.
- السلامة طويلة المدى الخاصة بالبهاق غير مثبتة.
الخلاصة
يجلس البهاق عند تقاطع المناعة الذاتية وبيولوجيا الخلايا الجذعية. علاج MSC هو أحد الأساليب القليلة التي تعالج جانبي هذه المعادلة. الأدلة قبل السريرية متسقة ومقنعة آلياً. الأدلة السريرية محدودة بتقارير الحالة — النتائج مشجعة في الاتجاه لكنها بعيدة عن أن تكون قاطعة. يظل علاج MSC للبهاق نهجاً قيد البحث مبني على بيولوجيا قبل سريرية صلبة؛ الإثبات السريري للمفهوم ينتظر التجارب العشوائية التي لم تبدأ بعد.
المراجع
- Ezzedine K, et al. Vitiligo. Lancet. 2015;386:74-84. doi:10.1016/S0140-6736(14)60763-7 ↩
- Frisoli ML, et al. Vitiligo pathogenesis. Annu Rev Immunol. 2020;38:621-648. doi:10.1146/annurev-immunol-100919-023531 ↩
- Nishimura EK. Melanocyte stem cells. Pigment Cell Melanoma Res. 2011;24:401-410. doi:10.1111/j.1755-148X.2011.00855.x ↩
- Shin TH, et al. MSCs inflammatory skin. Int J Mol Sci. 2017;18:244. doi:10.3390/ijms18020244 ↩
- Glennie S, et al. MSC T-cell anergy. Blood. 2005;105:2821-2827. doi:10.1182/blood-2004-09-3696 ↩
- Luz-Crawford P, et al. MSC Treg generation. Stem Cell Res Ther. 2013;4:65. doi:10.1186/scrt216 ↩
- Kim WS, et al. ADSC antioxidative. Arch Dermatol Res. 2009;301:329-336. doi:10.1007/s00403-009-0951-9 ↩
- Rabbani P, et al. Wnt melanocyte stem cells. Cell. 2011;145:941-955. doi:10.1016/j.cell.2011.05.004 ↩
- Maione AG, et al. 3D tissue models. Tissue Eng Part C. 2015;21:499-508. doi:10.1089/ten.TEC.2014.0414 ↩
- Zhu L, et al. MSCs melanocyte. Stem Cell Res Ther. 2018;9:248. doi:10.1186/s13287-018-0994-y ↩
- Lim YJ, et al. MSC + NB-UVB vitiligo. J Dermatol Sci. 2020;98:182-190. doi:10.1016/j.jdermsci.2020.04.005 ↩
- Wang Y, et al. MSC-CM melanocyte. Exp Dermatol. 2023;32:1011-1020. doi:10.1111/exd.14812 ↩
- Chen X, et al. UC-MSC vitiligo. J Cosmet Dermatol. 2019;18:1950-1954. doi:10.1111/jocd.12932 ↩
- Sharma P, et al. MSC vitiligo pilot. Dermatol Ther. 2021;34:e15086. doi:10.1111/dth.15086 ↩
- Patel AB, et al. MSC transplant. J Am Acad Dermatol. 2023;89:1028-1035. doi:10.1016/j.jaad.2023.07.1012 ↩
- Rodriguez M, et al. Incidental repigmentation. Autoimmun Rev. 2022;21:103200. doi:10.1016/j.autrev.2022.103200 ↩
- Lee SH, et al. Topical MSC hydrogel. J Invest Dermatol. 2024;144:689-698. doi:10.1016/j.jid.2023.09.275 ↩