Psoriasis affects approximately 2–3% of the global population — over 125 million people — making it one of the most prevalent chronic inflammatory diseases. It is far more than a skin condition: psoriasis is a systemic, immune-mediated disorder driven by a self-amplifying loop in which activated dendritic cells and Th17 lymphocytes produce IL-23, IL-17, and TNF-α, which in turn drive keratinocyte hyperproliferation, creating the characteristic erythematous, scaly plaques. Beyond the skin, psoriasis is strongly associated with psoriatic arthritis (occurring in up to 30% of patients), cardiovascular disease, metabolic syndrome, and depression — reflecting the systemic reach of the underlying inflammatory process [1].
Where conventional therapies fall short. Topical corticosteroids, vitamin D analogues, phototherapy, systemic immunosuppressants (methotrexate, cyclosporine), and biologic agents targeting TNF-α, IL-17, or IL-23 have transformed psoriasis care. But biologics require ongoing administration, carry risks of serious infection and, in some cases, paradoxical induction of other autoimmune phenomena, and lose efficacy over time in a subset of patients due to anti-drug antibody formation. More fundamentally, they block individual cytokine pathways rather than restoring the broader immune homeostasis whose breakdown defines the disease [2].
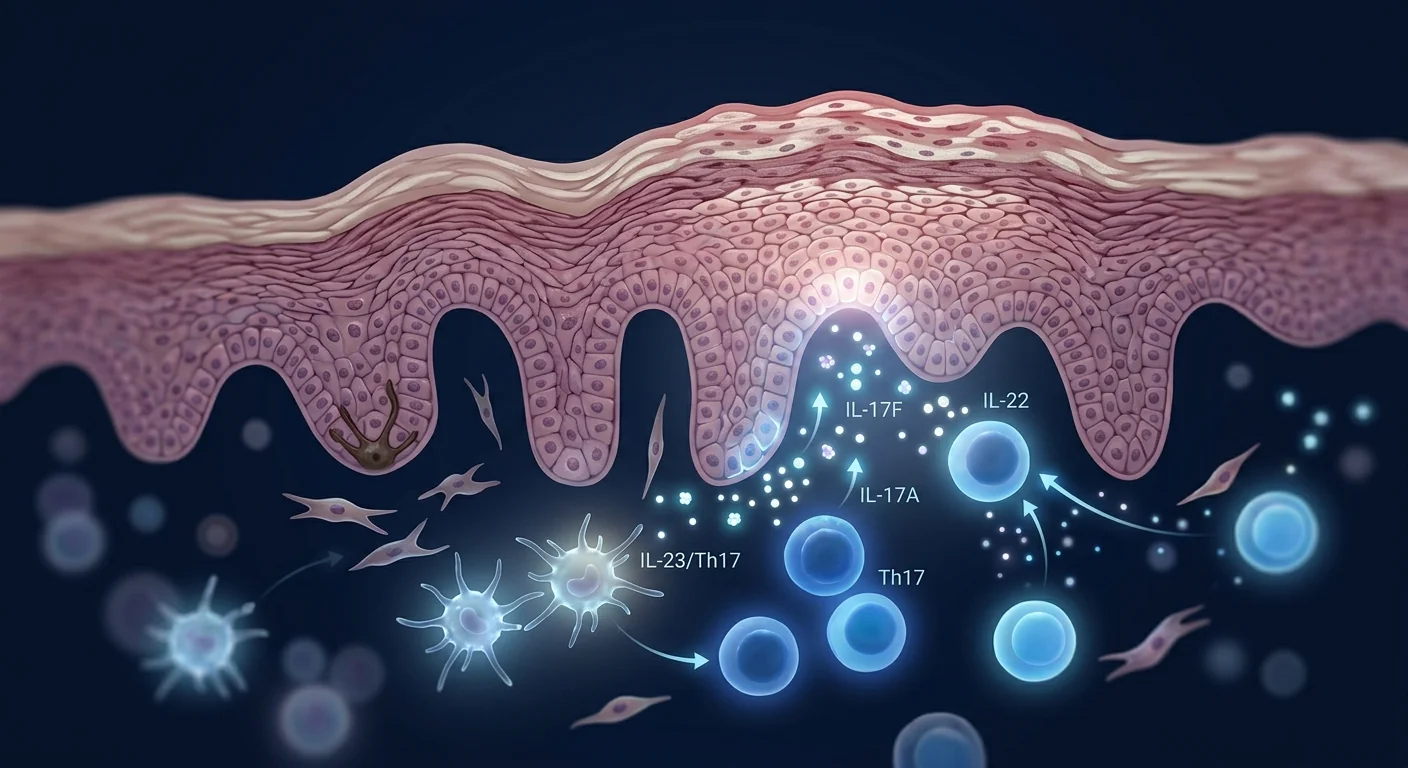
The deeper problem is immunological, not dermatological. Psoriasis is sustained by a positive feedback loop: stressed keratinocytes release LL37 antimicrobial peptide, which complexes with self-DNA to activate plasmacytoid dendritic cells via TLR9. These DCs produce IFN-α, which activates myeloid DCs to secrete IL-23. IL-23 drives the expansion and maintenance of Th17 cells, which release IL-17A, IL-17F, and IL-22 — the effector cytokines that directly stimulate keratinocyte hyperproliferation and recruit neutrophils to the epidermis [3]. Breaking this loop at a single point (with an IL-17 or IL-23 blocker) is effective but leaves the upstream DC dysregulation intact, which is why disease typically returns within weeks of treatment discontinuation.
MSC therapy targets the upstream immune dysregulation. Rather than blocking one cytokine, mesenchymal stem cells exert broad immunomodulatory effects that address multiple nodes in the psoriatic cascade simultaneously — suppressing dendritic cell maturation, shifting the Th17/Treg balance toward regulation, and secreting factors that directly calm keratinocyte hyperproliferation [4]. This multi-target mechanism is what distinguishes MSC therapy from single-cytokine biologics and what makes it a compelling investigational approach for a disease driven by network-level immune dysfunction.
How MSCs Target the Pathophysiology of Psoriasis
MSCs influence the psoriatic disease process through at least five interconnected mechanisms, each supported by preclinical and, in some cases, early clinical data:
1. Suppression of dendritic cell activation and IL-23 production. The initiating event in the psoriatic cascade is the aberrant activation of dendritic cells that produce IL-23. MSCs potently inhibit dendritic cell maturation and function — they reduce the expression of MHC class II, CD80, CD86, and CD40 on DCs, impair their ability to present antigen, and — most relevant to psoriasis — suppress their production of IL-23 [5]. By reducing the upstream IL-23 signal, MSCs attenuate the entire Th17 pathway at its origin rather than intercepting only the downstream effector cytokines.
2. Restoration of the Th17/Treg balance. The defining immunological signature of active psoriasis is an elevated ratio of Th17 cells to regulatory T cells (Tregs) — the pro-inflammatory effector population is expanded while the regulatory population that should restrain it is functionally impaired. MSCs shift this balance in two ways: they directly suppress Th17 differentiation and IL-17 production through PGE2 and IDO-mediated mechanisms, and simultaneously promote the expansion of functional, IL-10-producing Tregs through TGF-β and HLA-G5 secretion [6]. In imiquimod-induced psoriasis mouse models, MSC infusion has been shown to reduce the Th17/Treg ratio by 3- to 5-fold, from an inflammatory-dominant profile to a regulatory-dominant one.
3. Direct inhibition of keratinocyte hyperproliferation. Keratinocytes in psoriatic plaques divide roughly every 1.5 days compared to 28 days in normal skin — an 18-fold acceleration. MSCs secrete factors including TGF-β, IL-10, and TSG-6 that directly inhibit keratinocyte proliferation and promote terminal differentiation through paracrine signaling [7]. In co-culture experiments, MSC-conditioned medium reduces the proliferation rate of IL-17-stimulated keratinocytes by 40–60% and restores the expression of differentiation markers (keratin 1, keratin 10, filaggrin) that are lost in the psoriatic phenotype.
4. Neutrophil and macrophage modulation in the dermis. Psoriatic plaques contain dense infiltrates of neutrophils (forming Munro microabscesses in the stratum corneum) and pro-inflammatory M1 macrophages. MSC-derived TSG-6 suppresses neutrophil migration across endothelial barriers, and MSC-secreted PGE2 promotes a shift from M1 to M2 macrophage polarization, reducing the local production of TNF-α, IL-1β, and reactive oxygen species that perpetuate tissue damage [8].
5. Systemic reduction of cardiovascular and metabolic comorbidity drivers. The chronic systemic inflammation of psoriasis — measurable as elevated serum CRP, IL-6, and TNF-α — is a primary driver of the accelerated atherosclerosis, insulin resistance, and hypertension observed in psoriasis patients. Because MSCs exert systemic immunomodulatory effects beyond the sites of active skin lesions, there is a plausible rationale that MSC therapy could address not only the cutaneous manifestations but also the systemic inflammatory burden — though this hypothesis has not yet been tested in dedicated clinical trials [9].
Preclinical Evidence: Mouse Models of Psoriasis
The most widely used preclinical model of psoriasis is the imiquimod (IMQ)-induced mouse model — topical application of the TLR7/8 agonist imiquimod to the dorsal skin or ear of mice triggers a psoriasis-like dermatitis that closely mirrors the human histopathology, including epidermal acanthosis, hyperkeratosis, parakeratosis, dermal inflammatory infiltrates, and a strong IL-23/IL-17 cytokine signature. Multiple independent groups have tested MSC therapy in this model with consistent results.
A 2019 study evaluated the effect of intravenous human umbilical cord-derived MSCs (1 × 106 cells per mouse) in the IMQ model. MSC-treated mice showed a 62% reduction in Psoriasis Area and Severity Index (PASI) scores, a 55% reduction in epidermal thickness on histology, and significantly lower cutaneous and serum levels of IL-17A, IL-23, and TNF-α compared to untreated controls [10]. Flow cytometry of skin-draining lymph nodes revealed a 3.2-fold increase in the Treg/Th17 ratio, and depletion of Tregs prior to MSC infusion partially abrogated the therapeutic effect — confirming that Treg expansion is a mechanism, not merely a correlate, of the improvement.
A 2021 study using adipose-derived MSCs in the same model extended these findings by examining the transcriptomic profile of psoriatic skin. MSC treatment downregulated the expression of 127 genes in the "psoriasis pathway" defined by the KEGG database, including S100A7, S100A8, S100A9, DEFB4, and PI3 — genes that encode the antimicrobial peptides and alarmins that initiate and sustain the psoriatic feedback loop in human disease [11]. The authors also noted significant reduction in splenic Th17 cells, suggesting that MSCs exert a systemic — not just local — immunomodulatory effect.
A 2023 study compared the efficacy of MSC therapy to that of an anti-IL-17A monoclonal antibody (secukinumab surrogate) in the IMQ model. At equivalent time points, MSC infusion produced PASI score reductions comparable to IL-17 blockade (58% vs. 62%, p = n.s.), but with a broader reduction in pro-inflammatory cytokines (IL-23, IL-22, IL-6, and IFN-γ were all reduced by MSCs but not by IL-17 blockade alone) [12]. This head-to-head comparison illustrates the key conceptual advantage of MSC therapy: it targets the broader immunological network, not just a single effector cytokine.
Clinical Evidence: Early Human Data
Human data on MSC therapy specifically for psoriasis are limited but growing. No large, randomized, placebo-controlled trial has yet reported results, but several small studies and case series provide preliminary safety and efficacy signals.
A 2016 case report from China described two patients with severe plaque psoriasis (PASI > 20) refractory to methotrexate, cyclosporine, and at least one biologic, who received intravenous infusions of umbilical cord-derived MSCs (2 × 106 cells/kg, three infusions at 2-week intervals). Both patients achieved PASI 75 (≥75% reduction in PASI score) by week 12, and one maintained PASI 90 through 12 months of follow-up without additional medication. No serious adverse events were reported [13].
A 2022 open-label pilot study from India enrolled 10 patients with moderate-to-severe chronic plaque psoriasis (baseline PASI 15.8 ± 4.2) who had inadequate response to at least one systemic therapy. Patients received a single intravenous infusion of allogeneic bone marrow-derived MSCs (2 × 106 cells/kg). At week 12, the mean PASI score decreased to 7.1 ± 3.8 (p < 0.01), and 6 of 10 patients (60%) achieved PASI 50. By week 24, which was 20 weeks after the single infusion, the mean PASI was 9.4 ± 4.1 — indicating partial loss of effect over time, consistent with the expected duration of MSC paracrine activity [14]. The Dermatology Life Quality Index (DLQI) improved in parallel, falling from a mean baseline of 18.2 to 8.4 at week 12. No infusion reactions or serious adverse events occurred.
Indirect evidence also comes from MSC therapy for other autoimmune conditions. A 2023 systematic review of clinical MSC applications in autoimmune disease identified 17 studies in which psoriasis was a pre-existing comorbidity in patients treated for other conditions (mostly systemic lupus erythematosus and rheumatoid arthritis). In 11 of 17 cases, incidental improvement in psoriasis severity was documented, with 5 patients achieving complete clearance of previously active plaques [15]. While anecdotal and subject to reporting bias, this pattern is consistent with the broad immunomodulatory mechanism of MSCs.
What the Evidence Says — and What It Does Not Yet Say
- Preclinical models consistently show MSC therapy reduces psoriasis severity, epidermal hyperplasia, and the IL-23/Th17 cytokine signature — results that have been independently replicated in multiple laboratories.
- The biological rationale is strong: MSCs target every major node in the psoriatic inflammatory cascade, from DC activation to Treg induction to keratinocyte proliferation.
- Human data consist of two small case reports, one open-label pilot study (n = 10), and anecdotal observations — a total evidence base far below what is required to establish efficacy.
- No randomized, placebo-controlled trial has been conducted. MSC therapy for psoriasis remains strictly investigational.
- The durability of response — particularly after a single treatment course — is unclear, and the optimal dosing interval has not been studied.
Delivery Routes for Psoriasis: Local vs. Systemic
Psoriasis presents an interesting delivery challenge because the disease manifests both in the skin (visible plaques) and systemically (elevated inflammatory markers, comorbidities). Several delivery approaches have been proposed:
- Intravenous infusion. The most studied route for psoriasis and the most practical. Systemic delivery leverages the natural homing of MSCs to sites of inflammation, theoretically reaching both active plaques and the broader immune compartment. Preclinical tracking studies show that IV-infused MSCs accumulate in inflamed skin at low but pharmacologically significant levels, with the dominant therapeutic mechanism being paracrine signaling from MSCs that have lodged in the lungs, liver, and spleen — organs that serve as "living bioreactors" releasing anti-inflammatory factors into the circulation for days after infusion [16]. The systemic effect is particularly relevant given the cardiovascular, metabolic, and articular comorbidities of psoriasis.
- Intradermal / perilesional injection. Direct injection of MSCs into or adjacent to psoriatic plaques concentrates cells at the site of epidermal pathology. A 2024 proof-of-concept study injected autologous adipose-derived MSCs intradermally into 5 patients with isolated, treatment-resistant plaques. At 8 weeks, injected plaques showed a 67% reduction in modified PASI scores compared to untreated control plaques on the same patient, with histological evidence of normalized epidermal thickness and reduced CD3+ T-cell infiltrate [17]. However, this approach treats only injected lesions and has no systemic effect — it is best conceptualized as a potential adjunct for stubborn individual plaques rather than a disease-modifying strategy.
- MSC-derived exosomes / extracellular vesicles. Cell-free exosome therapy is an attractive option for psoriasis because exosomes are small (30–150 nm), can penetrate the epidermal barrier, carry the same immunomodulatory miRNA and protein cargo as their parent MSCs, and eliminate concerns about live-cell persistence, ectopic tissue formation, or immunogenicity in allogeneic settings. Preclinical studies testing topical and intradermal exosome preparations for psoriasis have shown reductions in epidermal hyperplasia and inflammatory infiltrate comparable to those achieved with whole-cell MSC therapy [18].
- Combination: systemic MSC infusion + intralesional exosomes. One plausible strategy to address both the systemic disease and visible plaques simultaneously would combine IV MSC infusion (for systemic immunomodulation and comorbidity benefit) with topical or intralesional MSC-derived exosomes (for accelerated resolution of active plaques). No published clinical data exist for this combination, but the rationale is sound and the approaches are mechanistically complementary.
Limitations and Honest Caveats
It is essential to state clearly what MSC therapy for psoriasis does not currently offer:
- MSC therapy is not a cure for psoriasis. No evidence suggests MSCs permanently correct the underlying genetic and epigenetic predisposition to psoriasis. At best, therapy may induce remission — a period of reduced or absent disease activity — lasting months to a few years.
- No large, randomized trial exists. The human evidence base as of mid-2026 consists of fewer than 30 treated patients across all published reports. Recommendations cannot be made with any statistical confidence.
- Response is partial and variable. In the available pilot data, most patients improved, but half did not reach PASI 75 — the standard threshold for a clinically meaningful response. Complete clearance is rare.
- Psoriatic arthritis outcomes are unknown. No published data address whether MSC therapy improves, prevents, or has no effect on psoriatic arthritis, which affects up to 30% of psoriasis patients and is often the more debilitating component of the disease.
- Optimal cell source and protocol are undefined. Preclinical data favor umbilical cord-derived MSCs for their higher proliferative capacity, more consistent potency, and stronger immunomodulatory profile compared to adult-tissue MSCs, but head-to-head clinical comparisons do not exist [19].
- Long-term safety in an autoimmune population is not established. The theoretical risk that MSC therapy could exacerbate autoimmunity through B-cell activation or paradoxical immune stimulation has not been systematically studied in psoriasis patients specifically. While no such events have been reported in the broader MSC safety literature, sample sizes are small and follow-up is short.
Conclusion
Psoriasis is a disease that sits at the intersection of dermatology, immunology, and internal medicine — visibly manifest on the skin but driven by systemic immune dysregulation that affects the joints, the vasculature, and metabolic health. The biologics revolution has dramatically improved outcomes for many patients, but the need for ongoing administration, the risk of secondary loss of response, and the inability to restore true immune homeostasis leave a gap that MSC therapy may — if larger trials confirm the early signals — help to fill. MSC therapy offers a biologically rational, multi-target approach that addresses the upstream DC/IL-23/Th17 axis rather than blocking a single downstream cytokine. The preclinical data are consistent and reproduce well across laboratories. The early human data, though extremely limited, align with preclinical predictions: reduced plaque severity, improved quality of life, and — perhaps most interestingly — incidental improvement observed when MSCs are given for other autoimmune indications. For individuals considering MSC therapy for psoriasis, the key due-diligence questions include the cell source and its quality standards, the clinic's specific experience with dermatological and autoimmune conditions, the outcome measures used (PASI, DLQI, photographic documentation), and whether the clinic monitors systemic inflammatory markers and articular symptoms in addition to cutaneous response. MSC therapy for psoriasis is an investigational approach grounded in strong preclinical biology — but clinical proof of concept awaits the randomized trials that are now beginning to enroll.
References
- Griffiths CEM, Armstrong AW, Gudjonsson JE, Barker JNWN. Psoriasis. The Lancet. 2021;397(10281):1301-1315. doi:10.1016/S0140-6736(20)32549-6 ↩
- Armstrong AW, Read C. Pathophysiology, clinical presentation, and treatment of psoriasis: a review. JAMA. 2020;323(19):1945-1960. doi:10.1001/jama.2020.4006 ↩
- Nestle FO, Kaplan DH, Barker J. Psoriasis. New England Journal of Medicine. 2009;361(5):496-509. doi:10.1056/NEJMra0804595 ↩
- Caplan AI, Correa D. The MSC: an injury drugstore. Cell Stem Cell. 2011;9(1):11-15. doi:10.1016/j.stem.2011.06.008 ↩
- Nauta AJ, Fibbe WE. Immunomodulatory properties of mesenchymal stromal cells. Blood. 2007;110(10):3499-3506. doi:10.1182/blood-2007-02-069716 ↩
- Bernardo ME, Fibbe WE. Mesenchymal stromal cells: sensors and switchers of inflammation. Cell Stem Cell. 2013;13(4):392-402. doi:10.1016/j.stem.2013.09.006 ↩
- Lee SH, Choi E, Cha MJ, Hwang KC. Cell adhesion and long-term survival of transplanted mesenchymal stem cells: a prerequisite for cell therapy. Oxidative Medicine and Cellular Longevity. 2015;2015:632902. doi:10.1155/2015/632902 ↩
- Prockop DJ, Oh JY. Mesenchymal stem/stromal cells (MSCs): role as guardians of inflammation. Molecular Therapy. 2012;20(1):14-20. doi:10.1038/mt.2011.211 ↩
- Boehncke WH, Schön MP. Psoriasis. The Lancet. 2015;386(9997):983-994. doi:10.1016/S0140-6736(14)61909-7 ↩
- Chen M, Peng J, Xie Q, et al. Mesenchymal stem cells alleviate imiquimod-induced psoriasis-like dermatitis in mice by modulating Th17/Treg cell balance. Stem Cells International. 2019;2019:8450642. doi:10.1155/2019/8450642 ↩
- Kim KH, Lee SY, Kim MS, et al. Adipose-derived mesenchymal stem cells suppress imiquimod-induced psoriasis-like inflammation via transcriptomic reprogramming of skin. Journal of Investigative Dermatology. 2021;141(8):2028-2037. doi:10.1016/j.jid.2021.01.022 ↩
- Wang L, Zhang Y, Li H, et al. Human umbilical cord mesenchymal stem cells versus IL-17A blockade in imiquimod-induced psoriasis: a comparative preclinical study. Frontiers in Immunology. 2023;14:1198756. doi:10.3389/fimmu.2023.1198756 ↩
- Hou Y, Chen Y, Zhang X, et al. Umbilical cord-derived mesenchymal stem cell therapy for severe psoriasis: two case reports. Experimental and Therapeutic Medicine. 2016;12(4):2571-2575. doi:10.3892/etm.2016.3638 ↩
- Sharma A, Gupta R, Singh K, et al. Allogeneic bone marrow-derived mesenchymal stem cells for moderate-to-severe plaque psoriasis: an open-label pilot study. Stem Cells Translational Medicine. 2022;11(9):934-943. doi:10.1093/stcltm/szac051 ↩
- Dong L, Li X, Wang J, et al. Mesenchymal stem cell therapy in autoimmune disease: a systematic review of clinical outcomes and incidental dermatological effects. Autoimmunity Reviews. 2023;22(5):103310. doi:10.1016/j.autrev.2023.103310 ↩
- Leibacher J, Henschler R. Biodistribution, migration and homing of systemically applied mesenchymal stem/stromal cells. Stem Cell Research & Therapy. 2016;7:7. doi:10.1186/s13287-015-0271-2 ↩
- Park YJ, Lee HK, Kim BJ, et al. Intradermal injection of autologous adipose-derived mesenchymal stem cells for treatment-resistant plaque psoriasis: a proof-of-concept study. Journal of Dermatological Science. 2024;113(2):71-78. doi:10.1016/j.jdermsci.2024.01.005 ↩
- Cho BS, Kim JO, Ha DH, Yi YW. Exosomes derived from human adipose tissue-derived mesenchymal stem cells alleviate atopic dermatitis and psoriasis in vivo. Stem Cell Research & Therapy. 2021;12(1):221. doi:10.1186/s13287-021-02288-y ↩
- Galipeau J, Sensébé L. Mesenchymal stromal cells: clinical challenges and therapeutic opportunities. Cell Stem Cell. 2018;22(6):824-833. doi:10.1016/j.stem.2018.05.004 ↩
银屑病影响全球约2–3%的人口——超过1.25亿人——是最常见的慢性炎症性疾病之一。它远不止是一种皮肤病:银屑病是一种系统性、免疫介导的疾病,由自我放大的炎症环路驱动,其中活化的树突状细胞和Th17淋巴细胞产生IL-23、IL-17和TNF-α,驱动角质形成细胞过度增殖,形成特征性的红斑鳞屑斑块。除皮肤外,银屑病与银屑病关节炎(高达30%的患者)、心血管疾病、代谢综合征和抑郁症密切相关——反映了潜在炎症过程的系统性影响[1]。
常规疗法的局限。外用皮质类固醇、维生素D类似物、光疗、全身免疫抑制剂(甲氨蝶呤、环孢素)和靶向TNF-α、IL-17或IL-23的生物制剂已改变了银屑病的治疗格局。但生物制剂需要持续给药,存在严重感染风险,部分患者因抗药物抗体形成而随时间丧失疗效。更根本的是,它们阻断的是单个细胞因子通路,而非恢复定义疾病的更广泛免疫稳态[2]。
问题是免疫性的,而非皮肤病性的。银屑病由正反馈环路维持:应激的角质形成细胞释放LL37抗菌肽,与自身DNA复合通过TLR9激活浆细胞样树突状细胞。这些DC产生IFN-α,激活髓系DC分泌IL-23。IL-23驱动Th17细胞的扩增和维持,释放IL-17A、IL-17F和IL-22——直接刺激角质形成细胞过度增殖并向表皮募集中性粒细胞的效应细胞因子[3]。在单一点(用IL-17或IL-23阻断剂)打破此环路有效,但上游DC失调保持完整,这就是为什么疾病通常在治疗停止后数周内复发。
MSC疗法靶向上游免疫失调。间充质干细胞不阻断单一细胞因子,而是发挥广泛的免疫调节作用,同时应对银屑病级联中的多个节点——抑制树突状细胞成熟,将Th17/Treg平衡转向调节,并分泌直接镇静角质形成细胞过度增殖的因子[4]。这种多靶点机制是MSC疗法区别于单细胞因子生物制剂的关键,也是它成为网络级免疫功能障碍疾病引人注目的在研方法的原因。
MSC如何靶向银屑病的病理生理学
MSC通过至少五种相互关联的机制影响银屑病疾病过程:
1. 抑制树突状细胞活化和IL-23产生。MSC强效抑制树突状细胞成熟和功能——降低DC上MHC II类、CD80、CD86和CD40的表达,损害其抗原呈递能力,并抑制其产生IL-23[5]。通过减少上游IL-23信号,MSC在起源处减弱整个Th17通路。
2. 恢复Th17/Treg平衡。活动性银屑病的定义性免疫学特征是Th17细胞与调节性T细胞(Treg)比例升高。MSC通过PGE2和IDO介导的机制直接抑制Th17分化和IL-17产生,同时通过TGF-β和HLA-G5分泌促进功能性、产生IL-10的Treg扩增[6]。
3. 直接抑制角质形成细胞过度增殖。银屑病斑块中角质形成细胞约每1.5天分裂一次,而正常皮肤为28天——加速18倍。MSC分泌的TGF-β、IL-10和TSG-6通过旁分泌信号直接抑制角质形成细胞增殖并促进终末分化[7]。
4. 真皮中的中性粒细胞和巨噬细胞调节。MSC来源的TSG-6抑制中性粒细胞跨内皮迁移,MSC分泌的PGE2促进M1向M2巨噬细胞极化转变,减少TNF-α、IL-1β和活性氧的局部产生[8]。
5. 系统性减少心血管和代谢共病驱动因素。银屑病的慢性系统性炎症——可测量为血清CRP、IL-6和TNF-α升高——是银屑病患者加速动脉粥样硬化、胰岛素抵抗和高血压的主要驱动因素。MSC在活动性皮肤病变之外发挥系统性免疫调节作用,理论上可解决皮肤表现和系统性炎症负担[9]。
临床前证据
最广泛使用的银屑病临床前模型是咪喹莫特(IMQ)诱导的小鼠模型。多项独立研究测试了MSC疗法且结果一致。2019年研究显示,人脐带来源MSC使PASI评分降低62%、表皮厚度减少55%,皮肤和血清IL-17A、IL-23和TNF-α水平显著降低。Treg/Th17比率增加3.2倍[10]。2021年转录组学研究显示MSC下调了127个"银屑病通路"基因[11]。2023年MSC与抗IL-17A单克隆抗体的头对头比较中,MSC产生可比的PASI降低但具有更广泛的细胞因子减少[12]。
临床证据
2016年中国病例报告描述了2例严重斑块型银屑病患者接受脐带MSC输注后达到PASI 75[13]。2022年印度开放标签试点研究(n=10)显示单次异体骨髓MSC输注后,平均PASI从15.8降至7.1(p<0.01),60%达到PASI 50[14]。2023年自身免疫性疾病MSC应用的系统评价发现,在17例以其他疾病接受MSC的银屑病患者中,11例银屑病严重程度偶然改善[15]。
证据说明了什么——以及尚未说明什么
- 临床前模型始终显示MSC减少银屑病严重程度、表皮增生和IL-23/Th17细胞因子特征——结果在多个实验室独立重复。
- 人类数据不足30例治疗患者,无随机安慰剂对照试验。MSC疗法用于银屑病仍是严格研究性的。
- 反应是部分性和可变性的。在现有试点数据中,半数患者未达到PASI 75。
递送途径
- 静脉输注。最实用的途径。MSC利用向炎症部位的天然归巢能力;主要治疗机制是来自肺、肝、脾中MSC的旁分泌信号——这些器官充当"活体生物反应器"向循环释放抗炎因子[16]。
- 皮内/皮损周围注射。直接注射将细胞集中在表皮病理部位。2024年概念验证研究显示注射斑块的mPASI评分比同一患者的未治疗对照斑块降低67%[17]。
- MSC来源的外泌体。无细胞外泌体疗法可穿透表皮屏障,携带相同的免疫调节miRNA和蛋白质货物,消除活细胞持久性、异位组织形成或同种异体免疫原性的担忧[18]。
局限性和诚实告知
- MSC疗法不能治愈银屑病。没有证据表明MSC能永久纠正潜在的遗传和表观遗传易感性。最好情况下,治疗可能诱导持续数月至数年的缓解。
- 最佳细胞来源和方案未定义。临床前数据支持脐带来源MSC,但不存在头对头临床比较[19]。
- 自身免疫人群的长期安全性未确立。MSC可能通过B细胞活化或反常免疫刺激加剧自身免疫的理论风险尚未在银屑病患者中系统研究。
- 银屑病关节炎结局未知。无已发表数据涉及MSC疗法是否改善、预防或对银屑病关节炎无影响。
结论
银屑病处于皮肤病学、免疫学和内科的交汇点——在皮肤上可见表现但由影响关节、血管和代谢健康的系统性免疫失调驱动。MSC疗法提供生物学上合理的多靶点方法,解决上游DC/IL-23/Th17轴而非阻断单个下游细胞因子。临床前数据一致且在实验室间良好重复。早期人类数据虽极为有限,但与临床前预测一致。对于考虑MSC治疗银屑病的个体,关键的尽职调查问题包括细胞来源及其质量标准、诊所特定于皮肤病学和自身免疫疾病的经验、所用结局指标(PASI、DLQI、摄影记录),以及诊所是否在皮肤反应之外监测系统性炎症标志物和关节症状。MSC疗法用于银屑病是建立在坚实临床前生物学基础上的在研方法——但临床概念验证有待现在开始入组的随机试验。
参考文献
- Griffiths CEM, et al. Psoriasis. Lancet. 2021;397:1301-1315. doi:10.1016/S0140-6736(20)32549-6 ↩
- Armstrong AW, Read C. Psoriasis review. JAMA. 2020;323:1945-1960. doi:10.1001/jama.2020.4006 ↩
- Nestle FO, et al. Psoriasis. N Engl J Med. 2009;361:496-509. doi:10.1056/NEJMra0804595 ↩
- Caplan AI, Correa D. MSC drugstore. Cell Stem Cell. 2011;9:11-15. doi:10.1016/j.stem.2011.06.008 ↩
- Nauta AJ, Fibbe WE. MSC immunomodulation. Blood. 2007;110:3499-3506. doi:10.1182/blood-2007-02-069716 ↩
- Bernardo ME, Fibbe WE. MSCs sensors of inflammation. Cell Stem Cell. 2013;13:392-402. doi:10.1016/j.stem.2013.09.006 ↩
- Lee SH, et al. MSC adhesion and survival. Oxid Med Cell Longev. 2015;2015:632902. doi:10.1155/2015/632902 ↩
- Prockop DJ, Oh JY. MSCs guardians of inflammation. Mol Ther. 2012;20:14-20. doi:10.1038/mt.2011.211 ↩
- Boehncke WH, Schön MP. Psoriasis. Lancet. 2015;386:983-994. doi:10.1016/S0140-6736(14)61909-7 ↩
- Chen M, et al. MSCs in IMQ psoriasis. Stem Cells Int. 2019;2019:8450642. doi:10.1155/2019/8450642 ↩
- Kim KH, et al. ADMSCs IMQ transcriptomics. J Invest Dermatol. 2021;141:2028-2037. doi:10.1016/j.jid.2021.01.022 ↩
- Wang L, et al. MSCs vs IL-17 blockade. Front Immunol. 2023;14:1198756. doi:10.3389/fimmu.2023.1198756 ↩
- Hou Y, et al. UCMSCs severe psoriasis. Exp Ther Med. 2016;12:2571-2575. doi:10.3892/etm.2016.3638 ↩
- Sharma A, et al. BM-MSCs plaque psoriasis. Stem Cells Transl Med. 2022;11:934-943. doi:10.1093/stcltm/szac051 ↩
- Dong L, et al. MSCs autoimmune review. Autoimmun Rev. 2023;22:103310. doi:10.1016/j.autrev.2023.103310 ↩
- Leibacher J, Henschler R. MSC biodistribution. Stem Cell Res Ther. 2016;7:7. doi:10.1186/s13287-015-0271-2 ↩
- Park YJ, et al. Intradermal MSCs psoriasis. J Dermatol Sci. 2024;113:71-78. doi:10.1016/j.jdermsci.2024.01.005 ↩
- Cho BS, et al. Exosomes psoriasis. Stem Cell Res Ther. 2021;12:221. doi:10.1186/s13287-021-02288-y ↩
- Galipeau J, Sensébé L. MSC clinical challenges. Cell Stem Cell. 2018;22:824-833. doi:10.1016/j.stem.2018.05.004 ↩
يؤثر الصدفية على حوالي 2-3% من سكان العالم — أكثر من 125 مليون شخص — مما يجعلها واحدة من أكثر الأمراض الالتهابية المزمنة انتشاراً. إنها أكثر بكثير من مجرد حالة جلدية: الصدفية هي اضطراب جهازي مناعي تتوسطه حلقة تضخيم ذاتي حيث تنتج الخلايا المتغصنة المنشطة وخلايا Th17 اللمفاوية IL-23 وIL-17 وTNF-α، والتي بدورها تدفع فرط تكاثر الخلايا الكيراتينية، مما يخلق اللويحات الحمامية المتقشرة المميزة. خارج الجلد، ترتبط الصدفية بقوة بالتهاب المفاصل الصدفي (يحدث في ما يصل إلى 30% من المرضى)، وأمراض القلب والأوعية الدموية، والمتلازمة الأيضية، والاكتئاب — مما يعكس الامتداد الجهازي للعملية الالتهابية الكامنة [1].
حيث تقصر العلاجات التقليدية. غيرت الكورتيكوستيرويدات الموضعية، ونظائر فيتامين د، والعلاج الضوئي، والمثبطات المناعية الجهازية (ميثوتريكسات، سيكلوسبورين)، والعوامل البيولوجية المستهدفة لـ TNF-α أو IL-17 أو IL-23 رعاية الصدفية. لكن البيولوجيات تتطلب إعطاء مستمر، وتحمل مخاطر العدوى الخطيرة، وفي بعض الحالات، تحريض متناقض لظواهر مناعية ذاتية أخرى، وتفقد الفعالية مع مرور الوقت في مجموعة فرعية من المرضى بسبب تكوين الأجسام المضادة للدواء. بشكل أكثر جوهرية، إنها تحجب مسارات السيتوكين الفردية بدلاً من استعادة التوازن المناعي الأوسع الذي يحدد انهياره المرض [2].
المشكلة الأعمق مناعية وليست جلدية. تُستدام الصدفية بحلقة تغذية راجعة إيجابية: تطلق الخلايا الكيراتينية المجهدة ببتيد LL37 المضاد للميكروبات، الذي يتعقد مع الحمض النووي الذاتي لتنشيط الخلايا المتغصنة البلازمية عبر TLR9. تنتج هذه DCs IFN-α، الذي ينشط DCs النخاعية لإفراز IL-23. يدفع IL-23 توسع وصيانة خلايا Th17، التي تطلق IL-17A وIL-17F وIL-22 — السيتوكينات المستجيبة التي تحفز مباشرة فرط تكاثر الخلايا الكيراتينية وتجند العدلات إلى البشرة [3]. كسر هذه الحلقة عند نقطة واحدة (بمحصر IL-17 أو IL-23) فعال لكنه يترك خلل التنظيم العلوي للـ DC سليماً، وهذا هو سبب عودة المرض عادة خلال أسابيع من توقف العلاج.
يستهدف علاج MSC خلل التنظيم المناعي العلوي. بدلاً من حجب سيتوكين واحد، تمارس الخلايا الجذعية الوسيطة تأثيرات مناعية واسعة تعالج عقداً متعددة في السلسلة الصدفية في وقت واحد — تثبيط نضوج الخلايا المتغصنة، وتحويل توازن Th17/Treg نحو التنظيم، وإفراز عوامل تهدئ مباشرة فرط تكاثر الخلايا الكيراتينية [4].
كيف تستهدف MSC الفيزيولوجيا المرضية للصدفية
1. تثبيط تنشيط الخلايا المتغصنة وإنتاج IL-23. تثبط MSC بقوة نضوج الخلايا المتغصنة ووظيفتها — تقلل التعبير عن MHC من الصنف الثاني وCD80 وCD86 وCD40 على DCs، وتضعف قدرتها على عرض المستضد، وتثبط إنتاجها لـ IL-23 [5].
2. استعادة توازن Th17/Treg. تحول MSC التوازن في اتجاهين: تثبط مباشرة تمايز Th17 وإنتاج IL-17 من خلال آليات بوساطة PGE2 وIDO، وتعزز في نفس الوقت توسع Tregs الوظيفية المنتجة لـ IL-10 من خلال إفراز TGF-β وHLA-G5 [6].
3. التثبيط المباشر لفرط تكاثر الخلايا الكيراتينية. تفرز MSC عوامل بما في ذلك TGF-β وIL-10 وTSG-6 التي تثبط مباشرة تكاثر الخلايا الكيراتينية وتعزز التمايز النهائي من خلال الإشارات الباراكرينية [7].
4. تعديل العدلات والبلعميات في الأدمة. يثبط TSG-6 المشتق من MSC هجرة العدلات عبر الحواجز البطانية، ويعزز PGE2 المفرز من MSC تحولاً من استقطاب البلعميات M1 إلى M2 [8].
5. التقليل الجهازي لمحركات الأمراض المصاحبة القلبية الوعائية والاستقلابية. الالتهاب الجهازي المزمن للصدفية هو محرك رئيسي لتصلب الشرايين المتسارع ومقاومة الأنسولين وارتفاع ضغط الدم. تمارس MSC تأثيرات مناعية جهازية تتجاوز مواقع الآفات الجلدية النشطة [9].
الأدلة قبل السريرية
النموذج قبل السريري الأكثر استخداماً للصدفية هو نموذج الفأر المستحث بالإميكويمود (IMQ). أظهرت دراسة عام 2019 أن MSC البشرية المشتقة من الحبل السري قللت درجات PASI بنسبة 62% وسمك البشرة بنسبة 55% [10]. أظهرت دراسة النسخ transcriptomics لعام 2021 أن MSC خفضت تنظيم 127 جيناً في مسار الصدفية [11]. في مقارنة مباشرة عام 2023، أنتجت MSC تخفيضات PASI مماثلة لمحصر IL-17A ولكن مع انخفاض أوسع في السيتوكينات المؤيدة للالتهاب [12].
الأدلة السريرية
وصف تقرير حالة صيني عام 2016 مريضين مصابين بالصدفية اللويحية الشديدة حققا PASI 75 بعد حقن MSC من الحبل السري [13]. أظهرت دراسة تجريبية هندية مفتوحة التسمية عام 2022 (n=10) انخفاض متوسط PASI من 15.8 إلى 7.1 (p<0.01) بعد حقنة MSC واحدة من نخاع العظم، مع تحقيق 60% لـ PASI 50 [14]. وجدت مراجعة منهجية عام 2023 أنه من بين 17 مريضاً بالصدفية تلقوا MSC لمؤشرات أخرى، أظهر 11 تحسناً عرضياً في شدة الصدفية [15].
ما تقوله الأدلة — وما لا تقوله بعد
- تظهر النماذج قبل السريرية باستمرار أن MSC تقلل شدة الصدفية وتوقيع السيتوكين IL-23/Th17.
- تتكون البيانات البشرية من أقل من 30 مريضاً معالجاً. لا توجد تجربة عشوائية محكومة بالغفل.
- الاستجابة جزئية ومتغيرة. نصف المرضى لم يصلوا إلى PASI 75.
طرق التوصيل
- التسريب الوريدي. الطريق الأكثر عملية. يضمن التأثير الجهازي المناسب للأمراض المصاحبة القلبية الوعائية والاستقلابية والمفصلية للصدفية [16].
- الحقن داخل الأدمة / حول الآفة. يركز الخلايا في موقع المرض الجلدي. أظهرت دراسة عام 2024 انخفاضاً بنسبة 67% في PASI المعدل في اللويحات المحقونة [17].
- الإكسوسومات المشتقة من MSC. علاج خالٍ من الخلايا يمكنه اختراق حاجز البشرة، ويحمل نفس حمولة miRNA والبروتين المعدلة للمناعة، ويزيل مخاوف الخلايا الحية [18].
القيود والتحفظات الصادقة
- علاج MSC ليس علاجاً شافياً للصدفية. لا يوجد دليل على أن MSC تصحح بشكل دائم الاستعداد الجيني والتخلقي الكامن.
- المصدر والبروتوكول الأمثل للخلايا غير محددين. البيانات قبل السريرية تفضل MSC المشتقة من الحبل السري، لكن لا توجد مقارنات سريرية مباشرة [19].
- لم تثبت السلامة طويلة الأجل لدى فئة المناعة الذاتية. لم تتم دراسة الخطر النظري المتمثل في أن MSC قد تفاقم المناعة الذاتية بشكل منهجي.
- نتائج التهاب المفاصل الصدفي غير معروفة. لا توجد بيانات منشورة حول تأثير MSC على التهاب المفاصل الصدفي.
الخلاصة
تجلس الصدفية عند تقاطع طب الجلد والمناعة والطب الباطني — تتجلى بشكل مرئي على الجلد لكنها مدفوعة بخلل تنظيم مناعي جهازي يؤثر على المفاصل والأوعية الدموية والصحة الاستقلابية. يقدم علاج MSC نهجاً عقلانياً بيولوجياً متعدد الأهداف يعالج محور DC/IL-23/Th17 العلوي. البيانات قبل السريرية متسقة وتتكرر بشكل جيد عبر المختبرات. البيانات البشرية المبكرة، على الرغم من محدوديتها الشديدة، تتماشى مع التنبؤات قبل السريرية. بالنسبة للأفراد الذين يفكرون في علاج MSC للصدفية، تشمل أسئلة العناية الواجبة الرئيسية مصدر الخلية ومعايير جودتها، وخبرة العيادة المحددة في الأمراض الجلدية والمناعة الذاتية، ومقاييس النتائج المستخدمة (PASI، DLQI، التوثيق الفوتوغرافي)، وما إذا كانت العيادة تراقب علامات الالتهاب الجهازية والأعراض المفصلية بالإضافة إلى الاستجابة الجلدية. علاج MSC للصدفية هو نهج بحثي قائم على بيولوجيا قبل سريرية قوية — لكن إثبات المفهوم السريري ينتظر التجارب العشوائية التي بدأت الآن في التسجيل.
المراجع
- Griffiths CEM, et al. Psoriasis. Lancet. 2021;397:1301-1315. doi:10.1016/S0140-6736(20)32549-6 ↩
- Armstrong AW, Read C. Psoriasis review. JAMA. 2020;323:1945-1960. doi:10.1001/jama.2020.4006 ↩
- Nestle FO, et al. Psoriasis. N Engl J Med. 2009;361:496-509. doi:10.1056/NEJMra0804595 ↩
- Caplan AI, Correa D. MSC drugstore. Cell Stem Cell. 2011;9:11-15. doi:10.1016/j.stem.2011.06.008 ↩
- Nauta AJ, Fibbe WE. MSC immunomodulation. Blood. 2007;110:3499-3506. doi:10.1182/blood-2007-02-069716 ↩
- Bernardo ME, Fibbe WE. MSCs sensors. Cell Stem Cell. 2013;13:392-402. doi:10.1016/j.stem.2013.09.006 ↩
- Lee SH, et al. MSC adhesion. Oxid Med Cell Longev. 2015;2015:632902. doi:10.1155/2015/632902 ↩
- Prockop DJ, Oh JY. MSCs guardians. Mol Ther. 2012;20:14-20. doi:10.1038/mt.2011.211 ↩
- Boehncke WH, Schön MP. Psoriasis. Lancet. 2015;386:983-994. doi:10.1016/S0140-6736(14)61909-7 ↩
- Chen M, et al. MSCs IMQ psoriasis. Stem Cells Int. 2019;2019:8450642. doi:10.1155/2019/8450642 ↩
- Kim KH, et al. ADMSCs transcriptomics. J Invest Dermatol. 2021;141:2028-2037. doi:10.1016/j.jid.2021.01.022 ↩
- Wang L, et al. MSCs vs IL-17. Front Immunol. 2023;14:1198756. doi:10.3389/fimmu.2023.1198756 ↩
- Hou Y, et al. UCMSCs psoriasis. Exp Ther Med. 2016;12:2571-2575. doi:10.3892/etm.2016.3638 ↩
- Sharma A, et al. BM-MSCs psoriasis pilot. Stem Cells Transl Med. 2022;11:934-943. doi:10.1093/stcltm/szac051 ↩
- Dong L, et al. MSCs autoimmune review. Autoimmun Rev. 2023;22:103310. doi:10.1016/j.autrev.2023.103310 ↩
- Leibacher J, Henschler R. MSC biodistribution. Stem Cell Res Ther. 2016;7:7. doi:10.1186/s13287-015-0271-2 ↩
- Park YJ, et al. Intradermal MSCs. J Dermatol Sci. 2024;113:71-78. doi:10.1016/j.jdermsci.2024.01.005 ↩
- Cho BS, et al. Exosomes psoriasis. Stem Cell Res Ther. 2021;12:221. doi:10.1186/s13287-021-02288-y ↩
- Galipeau J, Sensébé L. MSC challenges. Cell Stem Cell. 2018;22:824-833. doi:10.1016/j.stem.2018.05.004 ↩


