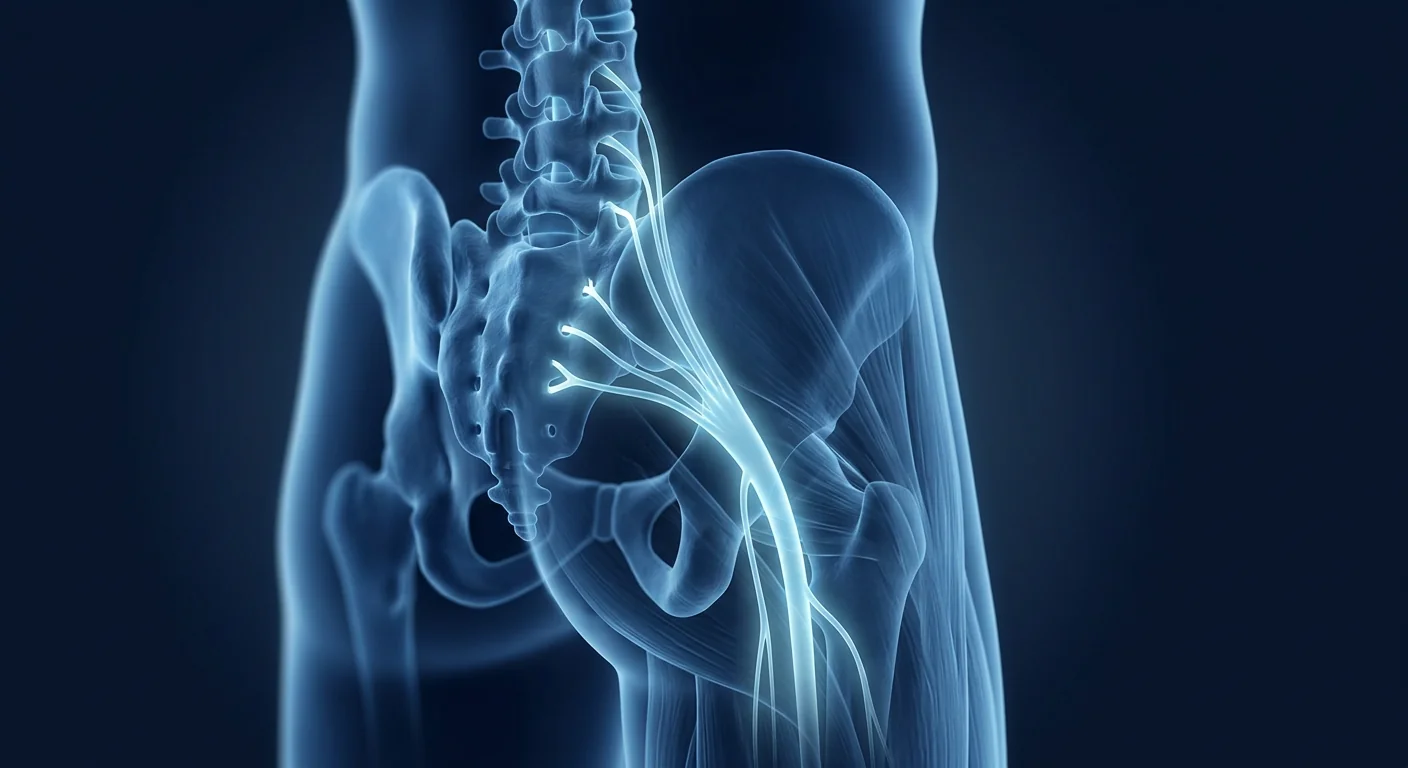
Sciatica is not a diagnosis — it is a symptom of a compressed or irritated nerve root in the lumbar spine. The hallmark is pain that travels from the lower back through the buttock and down the leg, following the path of the sciatic nerve — the longest and widest nerve in the human body, formed by nerve roots from L4 through S3. An estimated 10–40% of the population will experience at least one episode of sciatica in their lifetime, and a substantial proportion go on to develop chronic, disabling radicular pain that resists conventional treatment.[1]
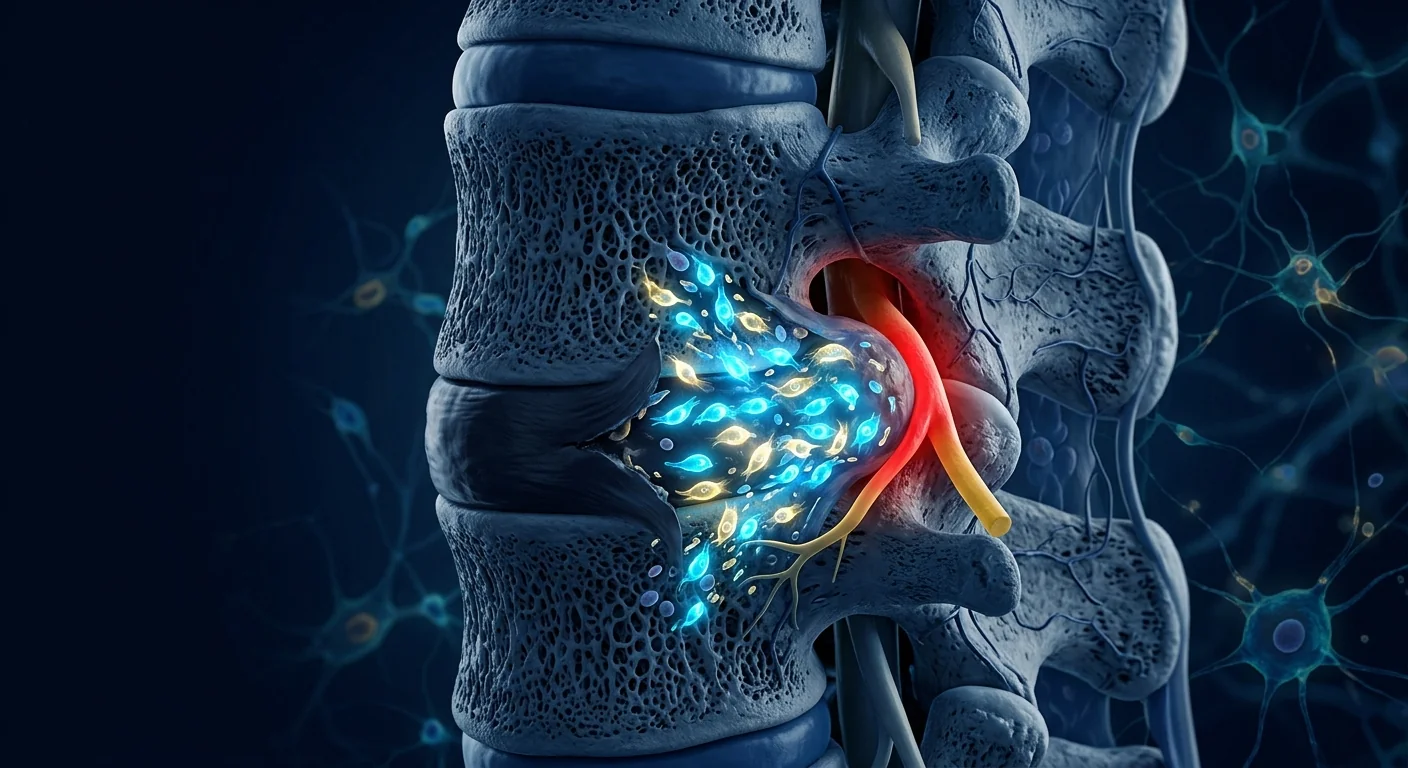
The most common cause is a herniated lumbar disc. When the soft nucleus pulposus breaches the fibrous annulus at L4–L5 or L5–S1, it can compress the adjacent nerve root — not just mechanically, but chemically. The extruded disc material triggers a potent inflammatory response, with elevated levels of TNF-α, IL-1β, IL-6, and prostaglandin E2 at the nerve root interface. This neuroinflammation — not mechanical compression alone — is what drives the characteristic burning, tingling, numbness, and weakness that define sciatica.
Conventional treatments bypass the biology. NSAIDs temporarily reduce prostaglandin synthesis but do not resolve the underlying cytokine cascade. Epidural steroid injections suppress inflammation locally but carry diminishing returns with repeated use and do not address disc integrity. For the roughly 10–20% of patients whose symptoms persist beyond 6–12 weeks, the pathway narrows to microdiscectomy — effective at removing the mechanical compression, but leaving the inflammatory milieu and disc degeneration unaddressed.
MSC therapy targets the nerve root environment directly. Mesenchymal stem cells do not simply mask pain — they engage the inflamed tissue and release a coordinated cocktail of anti-inflammatory mediators and neurotrophic factors. When delivered to the epidural space at the level of nerve root compression, MSCs can reduce local cytokine levels, support neural tissue integrity, and shift the local immune environment from degeneration toward regeneration.[2]
What Is Actually Happening at the Compressed Nerve Root
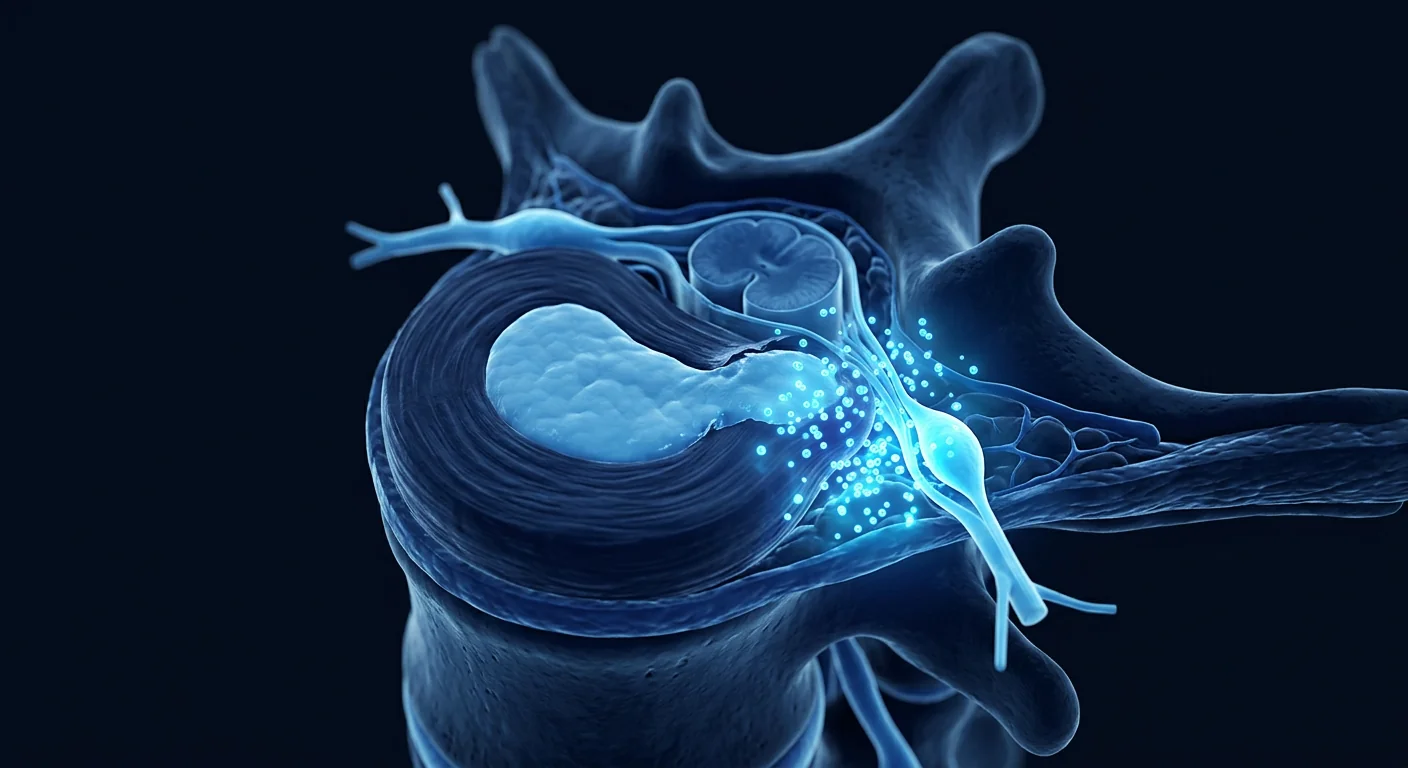
To understand why sciatica is so persistent, it helps to look at what happens at the nerve root interface. The dorsal root ganglion (DRG) — a cluster of sensory neuron cell bodies located just outside the spinal cord — is exquisitely sensitive to mechanical and chemical insult. When a herniated disc contacts the DRG or the nerve root, the extruded nucleus pulposus releases pro-inflammatory cytokines that sensitize nociceptors, lower the firing threshold of sensory neurons, and trigger ectopic discharges — signals sent to the brain even in the absence of a normal stimulus.[3]
This process has three overlapping components:
- Mechanical compression — the disc material physically deforms the nerve root, impairing axonal transport and microvascular blood flow.
- Chemical radiculitis — cytokines, chemokines, and matrix-degrading enzymes from the extruded nucleus pulposus directly inflame and irritate the nerve tissue.
- Immune activation — the nucleus pulposus is normally sequestered from the immune system; when exposed, it triggers an autoimmune-like inflammatory response that perpetuates the cycle.
This is why painkillers alone rarely provide lasting relief for chronic sciatica — they address only the descending pain signalling without touching the neuroinflammatory process that sustains it.
How MSC Therapy Works for Sciatica
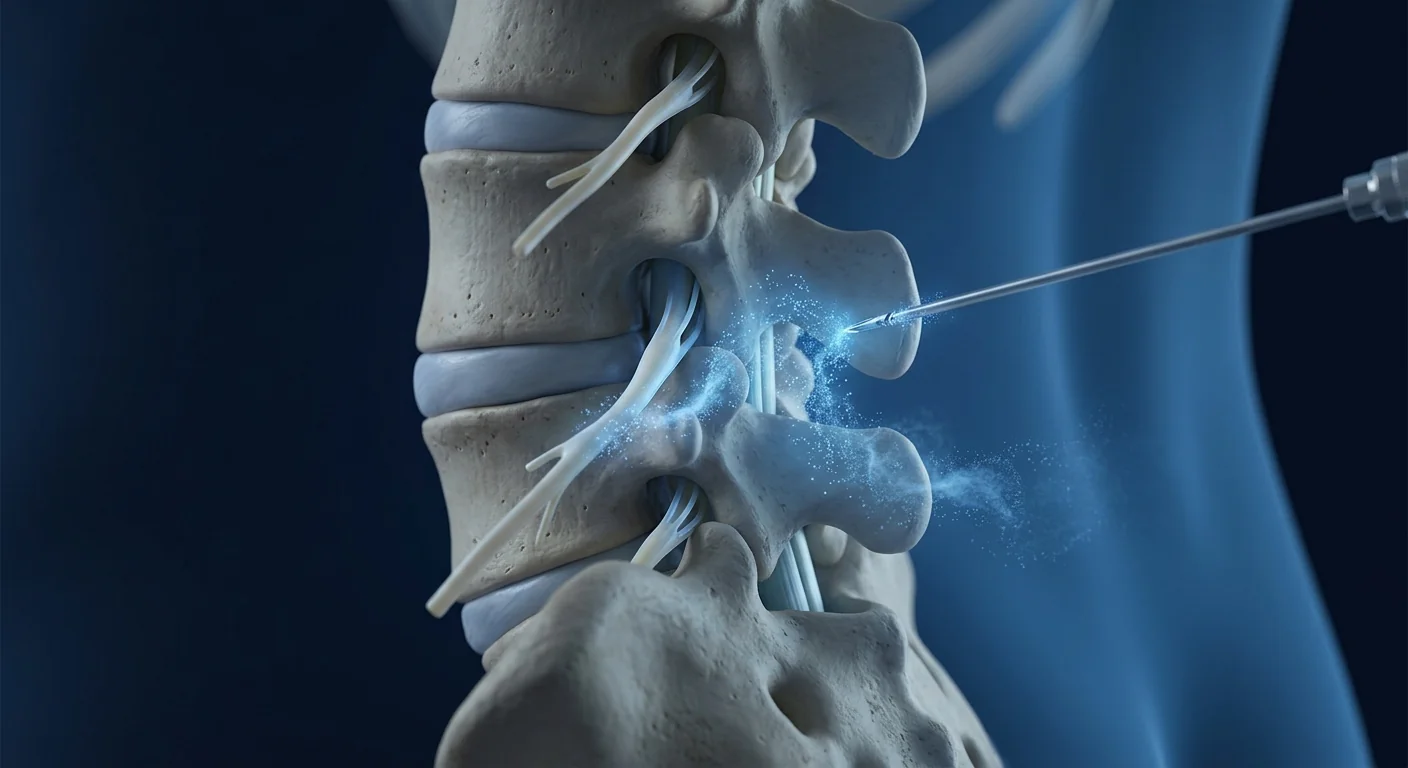
When clinical-grade MSCs are delivered to the epidural space near the compressed nerve root — typically via transforaminal epidural injection under fluoroscopic guidance — they engage the inflammatory environment through several coordinated mechanisms:[4]
1. They neutralize the cytokine storm at the nerve root
MSCs sense the high concentrations of TNF-α and IL-1β and respond by releasing powerful anti-inflammatory mediators — TSG-6, PGE2, IL-10, and IDO. TSG-6 in particular directly inhibits neutrophil migration, reduces macrophage activation, and dampens the cytokine cascade at its source. Within the epidural space, this can begin reducing radicular pain and sensory disturbances within the first few weeks after treatment.
2. They release neurotrophic and neuroprotective factors
MSCs secrete brain-derived neurotrophic factor (BDNF), nerve growth factor (NGF), glial cell line-derived neurotrophic factor (GDNF), and insulin-like growth factor-1 (IGF-1) — signalling molecules that support axonal integrity, promote Schwann cell activity, and protect neurons from apoptosis. At the compressed nerve root, this creates a biochemical environment that favours neural repair over ongoing degeneration.[5]
3. They modulate the local immune response
MSCs reprogram macrophages from a pro-inflammatory M1 phenotype to a regenerative M2 phenotype. In the context of disc herniation, this shift reduces the autoimmune-like response to exposed nucleus pulposus material, dampening the chronic inflammation that sustains radiculopathy long after the initial mechanical insult has resolved.[6]
4. They support disc matrix preservation
While the primary target in sciatica is the nerve root, MSCs also benefit the degenerating disc itself. Paracrine factors including TGF-β and BMP-7 signal resident disc cells to maintain proteoglycan and collagen synthesis, potentially slowing the progression of the disc degeneration that underlies recurrent herniation.[7]
What MSC Therapy Does NOT Do for Sciatica
Honest expectations matter. MSC therapy does not physically remove a herniated disc fragment. It does not reverse severe cauda equina syndrome, restore complete motor function in a long-standing foot drop, or correct advanced spinal stenosis. What it can do is reduce the neuroinflammation driving radicular pain, support nerve root healing, and potentially avoid or delay the need for surgical decompression in carefully selected patients with moderate herniation and persistent symptoms who have not progressed to severe neurological deficit.[8]
Who Is a Good Candidate for MSC Therapy in Sciatica?
The best outcomes are seen in patients whose sciatica is driven by neuroinflammation rather than purely mechanical compression. These are typically individuals who:[9]
- Have a contained or small-to-moderate herniated disc on MRI — not a large free fragment or complete extrusion with sequestration
- Experience radicular leg pain that is constant or near-constant, suggesting ongoing chemical radiculitis
- Have not responded adequately to conservative treatment — physical therapy, NSAIDs, and at least one epidural steroid injection
- Want to delay or avoid microdiscectomy surgery
- Do NOT have progressive motor weakness, cauda equina syndrome (bowel/bladder dysfunction, saddle anaesthesia), or severe spinal instability — these require urgent surgical evaluation
The role of the consultation — including a thorough MRI review, neurological examination, and functional assessment — is to distinguish inflammatory radiculopathy from surgical disc disease and determine whether regenerative therapy is appropriate for the individual patient.
What the Treatment Process Looks Like
At a clinical-grade centre, a typical sciatica-focused MSC protocol follows a structured pathway:
Step 1: Comprehensive Assessment
Lumbar MRI, neurological examination (sensory, motor, reflexes), pain mapping, and inflammatory biomarker evaluation. The goal is to identify the precise level of nerve root involvement — most commonly L4–L5 or L5–S1 — and confirm that neuroinflammation, not severe mechanical compression or instability, is the primary driver of symptoms.
Step 2: Protocol Design
The clinical team tailors the approach: transforaminal epidural injection under fluoroscopic guidance (the preferred route for sciatica, as it delivers MSCs directly to the affected nerve root), with or without supplementary IV infusion for systemic anti-inflammatory support. Dose, timing, and adjunctive physiotherapy are determined individually.
Step 3: Treatment Delivery
The transforaminal epidural injection is performed under real-time fluoroscopy or CT guidance, ensuring precise MSC placement at the nerve root–disc interface. The procedure is outpatient, takes 60–90 minutes including preparation, and patients walk out the same day with light activity restrictions.
Step 4: Recovery and Rehabilitation
A structured rehabilitation programme — including nerve gliding exercises, core stabilisation, postural retraining, and gradual return to activity — complements the cellular therapy. Most protocols recommend 48–72 hours of light activity followed by a graduated return to normal mobility over 2–4 weeks.
Step 5: Outcome Monitoring
Follow-up at 4, 12, and 24 weeks tracks pain using validated scales (Visual Analog Scale and Oswestry Disability Index), sensory and motor function, quality of life, and where clinically indicated, repeat MRI to assess disc and nerve root status.
Realistic Timelines: What to Expect and When
Cellular therapy follows a biological timeline, not a pharmacological one. Most patients experience response in three overlapping phases:[10]
Outcomes depend on disc herniation severity, duration of symptoms, nerve root involvement, MSC quality, dosing protocol, and the quality of the surrounding rehabilitation programme. A reputable clinic will be transparent about the proportion of patients experiencing strong, moderate, and limited benefit.
Safety and What Every Patient Should Know
When delivered with clinical-grade cells, image-guided technique, and appropriate clinical oversight, MSC therapy for sciatica has an excellent safety profile. The most common side effects are local: temporary post-injection soreness, mild stiffness, or a brief increase in radicular discomfort for 24–72 hours — likely reflecting the initial inflammatory response to the injection itself. Serious adverse events are rare in the published literature when GMP-grade cells and fluoroscopic guidance are used.[11]
The most significant preventable risk in this field is not the therapy itself — it is unregulated providers using non-clinical-grade cells with unverified sterility, identity, and potency. Patients should always confirm: MSC source and characterization (≥95% CD73/CD90/CD105 positive, ≤2% CD45/CD34/CD14 positive), laboratory certifications (ISO, GMP), and access to a Certificate of Analysis for the specific dose being administered.[12]
For the right patient — a contained disc herniation causing persistent radiculopathy with an inflammatory component — MSC therapy can offer meaningful relief without the recovery burden of surgery. The key is honest candidacy assessment before treatment begins.
— VELAR Clinical Team
The VELAR Approach to Sciatica
Sciatica protocols at VELAR Center begin with comprehensive MRI review, neurological examination, and biomarker assessment to map the precise nerve root involvement and confirm candidacy. Each protocol uses clinical-grade Wharton's jelly–derived MSCs (≥95% MSC marker expression, >90% post-thaw viability), delivered via transforaminal epidural injection under fluoroscopic guidance — with or without IV infusion depending on symptom severity and distribution. Every session is led by an experienced clinician, paired with structured neurorehabilitation, and monitored across the 1-, 3-, and 6-month milestones.[8]
If you are considering regenerative therapy for sciatica, the most important first step is an honest assessment of whether your specific disc pathology and symptom pattern are likely to respond — and a clear understanding of realistic outcomes for your stage of nerve root involvement.
Frequently Asked Questions
How much does stem cell therapy for sciatica cost in Thailand?
MSC therapy for sciatica in Thailand typically ranges from USD 6,000 to 12,000 depending on protocol complexity (single vs. combined delivery routes), cell dose, and whether adjunctive IV infusion is included. This is significantly lower than in the US or Europe, where comparable protocols often exceed USD 20,000.
Can MSC therapy replace surgery for a herniated disc?
MSC therapy may reduce or eliminate the need for microdiscectomy in carefully selected patients — those with contained disc herniations, inflammatory radiculopathy, and no progressive neurological deficits. It does not replace surgery for patients with large free fragments, cauda equina syndrome, or rapidly progressive motor weakness. An honest MRI-based assessment determines which path is appropriate.
How many MSC injections are needed for sciatica?
Most protocols involve a single transforaminal epidural injection session, sometimes combined with an IV infusion. Some patients with bilateral or multi-level involvement may benefit from a series of 2–3 sessions spaced 4–8 weeks apart. The exact protocol is determined after MRI review and neurological examination.
What is the success rate of stem cell therapy for sciatica?
Published studies on epidural MSC delivery for discogenic radiculopathy report that 60–75% of carefully selected patients experience clinically meaningful pain reduction (≥50% improvement on VAS) and functional gains at 6–12 months. Outcomes are strongest in patients with contained herniations, inflammatory-predominant symptoms, and symptoms present for less than 2 years.
Is MSC therapy for sciatica painful?
The transforaminal epidural injection itself involves brief local anaesthetic administration followed by the MSC injection under fluoroscopy — most patients describe it as pressure rather than pain. Post-procedure soreness at the injection site and a temporary increase in radicular discomfort lasting 24–72 hours is common and typically resolves with rest and ice.
How soon can I return to work after MSC therapy for sciatica?
Desk-based work can typically resume within 2–3 days. Physically demanding occupations may require 2–4 weeks of modified duties. The full biological response to MSC therapy develops over 2–3 months, so a gradual return to high-impact activities is recommended even if pain improves earlier.
References
- Stafford MA, Peng P, Hill DA. Sciatica: a review of history, epidemiology, pathogenesis, and the role of epidural steroid injection in management. British Journal of Anaesthesia. 2007;99(4):461-473. doi:10.1093/bja/aem238 ↩
- Urits I, Capuco A, Sharma M, et al. Stem cell therapies for treatment of discogenic low back pain: a comprehensive review. Current Pain and Headache Reports. 2019;23(9):65. doi:10.1007/s11916-019-0804-y ↩
- Valat JP, Genevay S, Marty M, Rozenberg S, Koes B. Sciatica. Best Practice & Research Clinical Rheumatology. 2010;24(2):241-252. doi:10.1016/j.berh.2009.11.005 ↩
- Centeno C, Markle J, Dodson E, et al. Treatment of lumbar degenerative disc disease-associated radicular pain with culture-expanded autologous mesenchymal stem cells: a pilot study on safety and efficacy. Journal of Translational Medicine. 2017;15(1):197. doi:10.1186/s12967-017-1300-y ↩
- Wilkins A, Kemp K, Ginty M, Hares K, Mallam E, Scolding N. Human bone marrow-derived mesenchymal stem cells secrete brain-derived neurotrophic factor which promotes neuronal survival in vitro. Stem Cell Research. 2009;3(1):63-70. doi:10.1016/j.scr.2009.02.006 ↩
- Caplan AI, Correa D. The MSC: an injury drugstore. Cell Stem Cell. 2011;9(1):11-15. doi:10.1016/j.stem.2011.06.008 ↩
- Sakai D, Schol J. Cell therapy for intervertebral disc repair: clinical perspective. Journal of Orthopaedic Translation. 2017;9:8-18. doi:10.1016/j.jot.2017.02.002 ↩
- Meisel HJ, Agarwal N, Hsieh PC, et al. Cell therapy for treatment of intervertebral disc degeneration: a systematic review. Global Spine Journal. 2019;9(1 Suppl):39S-52S. doi:10.1177/2192568219829024 ↩
- Pettine KA, Murphy MB, Suzuki RK, Sand TT. Percutaneous injection of autologous bone marrow concentrate cells significantly reduces lumbar discogenic pain through 12 months. Stem Cells. 2015;33(1):146-156. doi:10.1002/stem.1845 ↩
- Noriega DC, Ardura F, Hernández-Ramajo R, et al. Intervertebral disc repair by allogeneic mesenchymal bone marrow cells: a randomized controlled trial. Transplantation. 2017;101(8):1945-1951. doi:10.1097/TP.0000000000001484 ↩
- Dominici M, Le Blanc K, Mueller I, et al. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy. 2006;8(4):315-317. doi:10.1080/14653240600855905 ↩
- Orozco L, Soler R, Morera C, Alberca M, Sánchez A, García-Sancho J. Intervertebral disc repair by autologous mesenchymal bone marrow cells: a pilot study. Transplantation. 2011;92(7):822-828. doi:10.1097/TP.0b013e3182298a15 ↩
坐骨神经痛不是一个诊断——它是腰椎神经根受压或受刺激的症状。其标志性疼痛从下背部穿过臀部并向下延伸至腿部,沿着坐骨神经的路径——人体最长最宽的神经,由L4至S3的神经根组成。据估计,10–40%的人口在一生中至少会经历一次坐骨神经痛发作,其中相当大比例会发展为对常规治疗无效的慢性、致残性根性疼痛。[1]
最常见的原因是腰椎间盘突出。当柔软的髓核在L4–L5或L5–S1处突破纤维环时,它会压迫邻近的神经根——不仅是机械性的,也是化学性的。突出的椎间盘物质触发强烈的炎症反应,在神经根界面产生高浓度的TNF-α、IL-1β、IL-6和前列腺素E2。正是这种神经炎症——而非单纯的机械压迫——驱动了坐骨神经痛特征性的烧灼感、刺痛感、麻木感和无力感。
常规治疗绕开了生物学根源。非甾体抗炎药暂时减少前列腺素合成,但不能解决潜在的细胞因子级联反应。硬膜外类固醇注射局部抑制炎症,但重复使用的效果递减,且不解决椎间盘完整性问题。对于约10–20%的症状持续超过6–12周的患者,路径缩小到显微椎间盘切除术——有效去除机械压迫,但未解决炎症环境和椎间盘退行性问题。
MSC疗法直接针对神经根环境。间充质干细胞不仅掩盖疼痛——它们作用于发炎的组织并释放协调的抗炎介质和神经营养因子。当通过硬膜外腔递送到神经根受压水平时,MSC可以降低局部细胞因子水平,支持神经组织完整性,并将局部免疫环境从退化转向再生。[2]
受压神经根处究竟发生了什么
要理解坐骨神经痛为何如此顽固,有助于观察神经根界面发生了什么。背根神经节(DRG)——位于脊髓外侧的感觉神经元胞体簇——对机械性和化学性损伤极度敏感。当突出的椎间盘接触DRG或神经根时,挤出的髓核释放促炎细胞因子,敏化伤害感受器,降低感觉神经元放电阈值,并触发异位放电——即使没有正常刺激,信号也会传至大脑。[3]
这一过程包含三个重叠的成分:
- 机械压迫——椎间盘材料物理性地使神经根变形,损害轴突运输和微血管血流。
- 化学性神经根炎——来自挤出髓核的细胞因子、趋化因子和基质降解酶直接使神经组织发炎并受刺激。
- 免疫激活——髓核通常与免疫系统隔离;暴露时,它会触发类自身免疫的炎症反应,延续循环。
这就是为什么单独的止痛药很少能为慢性坐骨神经痛提供持久缓解——它们只针对下行疼痛信号,而不触及维持疼痛的神经炎症过程。
MSC疗法如何治疗坐骨神经痛
当临床级MSC被递送到受压神经根附近的硬膜外腔——通常通过荧光透视引导下的经椎间孔硬膜外注射——它们通过若干协调机制与炎症环境互动:[4]
1. 中和神经根处的细胞因子风暴
MSC感知高浓度的TNF-α和IL-1β,通过释放强大的抗炎介质——TSG-6、PGE2、IL-10和IDO来应对。TSG-6尤其直接抑制中性粒细胞迁移,减少巨噬细胞活化,并在源头减弱细胞因子级联反应。在硬膜外腔内,这可以在治疗后的最初几周内开始减少根性疼痛和感觉障碍。
2. 释放神经营养和神经保护因子
MSC分泌脑源性神经营养因子(BDNF)、神经生长因子(NGF)、胶质细胞源性神经营养因子(GDNF)和胰岛素样生长因子-1(IGF-1)——支持轴突完整性、促进施万细胞活性并保护神经元免于凋亡的信号分子。在受压神经根处,这创造了有利于神经修复而非持续退化的生化环境。[5]
3. 调节局部免疫反应
MSC将巨噬细胞从促炎性M1表型重新编程为再生性M2表型。在椎间盘突出的背景下,这种转变减少了对暴露的髓核材料的类自身免疫反应,抑制了在初始机械性损伤消退后长期维持根性病变的慢性炎症。[6]
4. 支持椎间盘基质保护
虽然坐骨神经痛的主要目标是神经根,但MSC也有益于正在退化的椎间盘本身。包括TGF-β和BMP-7在内的旁分泌因子向常驻椎间盘细胞发出信号以维持蛋白多糖和胶原合成,可能减缓导致复发性突出的椎间盘退行性进程。[7]
MSC疗法对坐骨神经痛所不能做的事
诚实的期望很重要。MSC疗法不会物理性地移除突出的椎间盘碎片。它不会逆转严重的马尾综合征,不会恢复长期足下垂的完全运动功能,也不会纠正晚期椎管狭窄。它能做的是减少驱动根性疼痛的神经炎症,支持神经根愈合,并可能在经过仔细筛选、具有中度突出和持续症状但尚未进展到严重神经功能缺损的患者中避免或延迟手术减压的需要。[8]
谁是MSC治疗坐骨神经痛的合适候选者?
最佳疗效见于坐骨神经痛主要由神经炎症而非单纯机械压迫驱动的患者。这些通常是个体:[9]
- MRI上显示包含性或小至中度椎间盘突出——而非大型游离碎片或完全挤出伴游离体
- 经历持续或近乎持续的根性腿痛,提示正在进行的化学性神经根炎
- 对保守治疗——物理治疗、非甾体抗炎药和至少一次硬膜外类固醇注射——反应不佳
- 希望延迟或避免显微椎间盘切除术
- 没有进行性运动无力、马尾综合征(肠/膀胱功能障碍、鞍区感觉缺失)或严重脊柱不稳——这些需要紧急手术评估
咨询的作用——包括详尽的MRI审阅、神经系统检查和功能评估——是区分炎症性根性病变和手术性椎间盘疾病,并确定再生疗法是否适合具体患者。
治疗过程是什么样子
在临床级中心,典型的以坐骨神经痛为重点的MSC方案遵循结构化路径:
第一步:综合评估
腰椎MRI、神经系统检查(感觉、运动、反射)、疼痛定位图和炎症生物标志物评估。目标是确定神经根受累的精确水平——最常见的是L4–L5或L5–S1——并确认神经炎症而非严重机械压迫或不稳是症状的主要驱动因素。
第二步:方案设计
临床团队定制方法:在荧光透视引导下经椎间孔硬膜外注射(坐骨神经痛的首选途径,因为它将MSC直接递送到受影响的神经根),有或没有辅助IV输注以提供全身抗炎支持。剂量、时间和辅助物理治疗均个体化确定。
第三步:治疗实施
经椎间孔硬膜外注射在实时荧光透视或CT引导下进行,确保MSC精确放置在神经根–椎间盘界面。该手术为门诊手术,包括准备在内需60–90分钟,患者当天即可行走离开,有轻度活动限制。
第四步:恢复和康复
结构化的康复计划——包括神经滑动练习、核心稳定、姿势再训练和逐渐恢复活动——与细胞治疗相辅相成。大多数方案建议48–72小时轻度活动,然后在2–4周内逐渐恢复正常活动能力。
第五步:疗效监测
在4、12和24周进行随访,使用经验证的量表(视觉模拟量表和Oswestry功能障碍指数)跟踪疼痛、感觉和运动功能、生活质量,并在临床需要时重复MRI以评估椎间盘和神经根状态。
实际时间表:何时期待什么
细胞疗法遵循生物学时间线而非药理学时间线。大多数患者在三个重叠阶段中体验反应:[10]
疗效取决于椎间盘突出严重程度、症状持续时间、神经根受累程度、MSC质量、剂量方案以及周围康复计划的质量。信誉良好的诊所将透明地说明经历强、中、有限受益的患者比例。
安全性与每位患者应知道的
当以临床级细胞、影像引导技术和适当的临床监督递送时,MSC治疗坐骨神经痛具有出色的安全性。最常见的副作用是局部的:注射后24–72小时的暂时酸痛、轻度僵硬或根性不适短暂增加——可能反映了注射本身的最初炎症反应。在使用GMP级细胞和荧光透视引导的已发表文献中,严重不良事件罕见。[11]
该领域最重要的可预防风险不是治疗本身——而是未经监管的提供者使用未经验证无菌性、身份和效力的非临床级细胞。患者应始终确认:MSC来源和特性(CD73/CD90/CD105阳性≥95%,CD45/CD34/CD14阳性≤2%)、实验室认证(ISO、GMP),以及获取所给予特定剂量的分析证书。[12]
对于合适的患者——包含性椎间盘突出引起持续性根性病变并伴有炎症成分——MSC疗法可以在没有手术恢复负担的情况下提供有意义的缓解。关键是在治疗开始前进行诚实的候选资格评估。
——VELAR 临床团队
VELAR的坐骨神经痛治疗方法
VELAR Center的坐骨神经痛方案从全面的MRI审阅、神经系统检查和生物标志物评估开始,以绘制精确的神经根受累情况并确认候选资格。每个方案使用临床级华通氏胶来源MSC(MSC标志物表达≥95%,解冻后活性>90%),通过荧光透视引导下的经椎间孔硬膜外注射递送——根据症状严重程度和分布情况有或没有IV输注。每次会话由经验丰富的临床医师主导,搭配结构化神经康复,并在1、3和6个月里程碑进行监测。[8]
如果您正在考虑坐骨神经痛的再生疗法,最重要的第一步是诚实评估您的具体椎间盘病理和症状模式是否可能响应——以及清晰理解您神经根受累阶段的实际疗效。
常见问题
泰国的干细胞治疗坐骨神经痛费用是多少?
泰国坐骨神经痛的MSC疗法通常费用在6,000至12,000美元之间,取决于方案复杂性(单一vs联合递送途径)、细胞剂量以及是否包含辅助IV输注。这显著低于美国或欧洲,那里同类方案通常超过20,000美元。
MSC疗法能否替代椎间盘突出手术?
在精心筛选的患者中——具有包含性椎间盘突出、炎症性根性病变且无进行性神经功能缺损者——MSC疗法可能减少或消除显微椎间盘切除术的需要。它不能替代需手术的大型游离碎片、马尾综合征或快速进行性运动无力患者。基于MRI的诚实评估决定哪条路径合适。
坐骨神经痛需要多少次MSC注射?
大多数方案涉及单次经椎间孔硬膜外注射会话,有时结合IV输注。一些双侧或多节段受累的患者可能受益于间隔4–8周的2–3次系列。确切方案在MRI审阅和神经系统检查后确定。
干细胞治疗坐骨神经痛的成功率是多少?
已发表的关于硬膜外MSC递送治疗椎间盘源性根性病变的研究报告称,60–75%的精心筛选患者在6–12个月时体验到临床上有意义的疼痛减轻(VAS改善≥50%)和功能获益。疗效在包含性突出、炎症为主症状且症状出现少于2年的患者中最强。
MSC治疗坐骨神经痛是否疼痛?
经椎间孔硬膜外注射本身涉及简短的局部麻醉给药,随后在荧光透视下进行MSC注射——大多数患者描述为压力而非疼痛。注射部位术后酸痛和24–72小时的根性不适暂时增加是常见的,通常通过休息和冰敷缓解。
MSC治疗坐骨神经痛后多久可以恢复工作?
案头工作通常可在2–3天内恢复。体力要求高的职业可能需要2–4周的调整工作。MSC疗法的完全生物学反应在2–3个月内发展,因此即使疼痛提前改善,也建议逐渐恢复高强度活动。
参考文献
- Stafford MA, Peng P, Hill DA. Sciatica: a review of history, epidemiology, pathogenesis, and the role of epidural steroid injection in management. British Journal of Anaesthesia. 2007;99(4):461-473. doi:10.1093/bja/aem238 ↩
- Urits I, Capuco A, Sharma M, et al. Stem cell therapies for treatment of discogenic low back pain: a comprehensive review. Current Pain and Headache Reports. 2019;23(9):65. doi:10.1007/s11916-019-0804-y ↩
- Valat JP, Genevay S, Marty M, Rozenberg S, Koes B. Sciatica. Best Practice & Research Clinical Rheumatology. 2010;24(2):241-252. doi:10.1016/j.berh.2009.11.005 ↩
- Centeno C, Markle J, Dodson E, et al. Treatment of lumbar degenerative disc disease-associated radicular pain with culture-expanded autologous mesenchymal stem cells: a pilot study on safety and efficacy. Journal of Translational Medicine. 2017;15(1):197. doi:10.1186/s12967-017-1300-y ↩
- Wilkins A, Kemp K, Ginty M, Hares K, Mallam E, Scolding N. Human bone marrow-derived mesenchymal stem cells secrete brain-derived neurotrophic factor which promotes neuronal survival in vitro. Stem Cell Research. 2009;3(1):63-70. doi:10.1016/j.scr.2009.02.006 ↩
- Caplan AI, Correa D. The MSC: an injury drugstore. Cell Stem Cell. 2011;9(1):11-15. doi:10.1016/j.stem.2011.06.008 ↩
- Sakai D, Schol J. Cell therapy for intervertebral disc repair: clinical perspective. Journal of Orthopaedic Translation. 2017;9:8-18. doi:10.1016/j.jot.2017.02.002 ↩
- Meisel HJ, Agarwal N, Hsieh PC, et al. Cell therapy for treatment of intervertebral disc degeneration: a systematic review. Global Spine Journal. 2019;9(1 Suppl):39S-52S. doi:10.1177/2192568219829024 ↩
- Pettine KA, Murphy MB, Suzuki RK, Sand TT. Percutaneous injection of autologous bone marrow concentrate cells significantly reduces lumbar discogenic pain through 12 months. Stem Cells. 2015;33(1):146-156. doi:10.1002/stem.1845 ↩
- Noriega DC, Ardura F, Hernández-Ramajo R, et al. Intervertebral disc repair by allogeneic mesenchymal bone marrow cells: a randomized controlled trial. Transplantation. 2017;101(8):1945-1951. doi:10.1097/TP.0000000000001484 ↩
- Dominici M, Le Blanc K, Mueller I, et al. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy. 2006;8(4):315-317. doi:10.1080/14653240600855905 ↩
- Orozco L, Soler R, Morera C, Alberca M, Sánchez A, García-Sancho J. Intervertebral disc repair by autologous mesenchymal bone marrow cells: a pilot study. Transplantation. 2011;92(7):822-828. doi:10.1097/TP.0b013e3182298a15 ↩
عرق النسا ليس تشخيصاً — إنه عرض لجذر عصبي مضغوط أو متهيج في العمود الفقري القطني. العلامة المميزة هي ألم يمتد من أسفل الظهر عبر الأرداف ونزولاً إلى الساق، متبعاً مسار العصب الوركي — أطول وأعرض عصب في جسم الإنسان، يتكون من جذور عصبية من L4 إلى S3. يُقدَّر أن 10–40% من السكان سيختبرون نوبة واحدة على الأقل من عرق النسا في حياتهم، وتتطور نسبة كبيرة إلى ألم جذري مزمن معيق يقاوم العلاج التقليدي.[1]
السبب الأكثر شيوعاً هو انفتاق قرص قطني. عندما تخترق النواة اللبية الرخوة الحلقة الليفية عند L4–L5 أو L5–S1، يمكنها ضغط جذر العصب المجاور — ليس فقط ميكانيكياً، بل كيميائياً أيضاً. تثير مادة القرص المنبثقة استجابة التهابية قوية، مع مستويات مرتفعة من TNF-α وIL-1β وIL-6 والبروستاغلاندين E2 عند واجهة جذر العصب. هذا الالتهاب العصبي — وليس الضغط الميكانيكي وحده — هو ما يدفع الحرقان والوخز والخدر والضعف المميزة لعرق النسا.
العلاجات التقليدية تتجاوز البيولوجيا. مضادات الالتهاب غير الستيرويدية تقلل مؤقتاً تصنيع البروستاغلاندين لكنها لا تحل سلسلة السيتوكينات الأساسية. حقن الستيرويد فوق الجافية تثبط الالتهاب موضعياً لكنها تحقق عوائد متناقصة مع الاستخدام المتكرر ولا تعالج سلامة القرص. بالنسبة لحوالي 10–20% من المرضى الذين تستمر أعراضهم لأكثر من 6–12 أسبوعاً، يضيق المسار إلى استئصال القرص المجهري — فعال في إزالة الضغط الميكانيكي، لكنه يترك البيئة الالتهابية وتنكس القرص دون معالجة.
علاج MSC يستهدف بيئة جذر العصب مباشرة. الخلايا الجذعية الوسيطة لا تخفي الألم ببساطة — إنها تتفاعل مع النسيج الملتهب وتطلق مزيجاً منسقاً من الوسائط المضادة للالتهاب والعوامل المغذية للأعصاب. عند التوصيل إلى الحيز فوق الجافية عند مستوى ضغط جذر العصب، يمكن لـ MSC تقليل مستويات السيتوكينات المحلية، دعم سلامة النسيج العصبي، وتحويل البيئة المناعية المحلية من التدهور نحو التجدد.[2]
ما يحدث فعلياً عند جذر العصب المضغوط
لفهم لماذا يكون عرق النسا مستمراً جداً، من المفيد النظر إلى ما يحدث عند واجهة جذر العصب. العقدة الجذرية الظهرية (DRG) — مجموعة من أجسام الخلايا العصبية الحسية تقع خارج الحبل الشوكي مباشرة — حساسة بشكل استثنائي للإصابة الميكانيكية والكيميائية. عندما يتصل القرص المنفتق بـ DRG أو جذر العصب، تطلق النواة اللبية المنبثقة سيتوكينات التهابية تُحسس مستقبلات الألم، تخفض عتبة إطلاق الخلايا العصبية الحسية، وتثير تفريغات شاذة — إشارات تُرسل إلى الدماغ حتى في غياب منبه طبيعي.[3]
لهذه العملية ثلاثة مكونات متداخلة:
- الضغط الميكانيكي — مادة القرص تشوه جذر العصب فيزيائياً، معيقةً النقل المحوري وتدفق الدم الشعري الدقيق.
- التهاب الجذر الكيميائي — السيتوكينات والكيموكينات والإنزيمات المحللة للمصفوفة من النواة اللبية المنبثقة تلتهب وتهيج النسيج العصبي مباشرة.
- التنشيط المناعي — النواة اللبية معزولة طبيعياً عن الجهاز المناعي؛ عند انكشافها، تثير استجابة التهابية شبه مناعية ذاتية تديم الدورة.
لهذا نادراً ما توفر مسكنات الألم وحدها راحة مستدامة لعرق النسا المزمن — إنها تعالج فقط إشارات الألم الهابطة دون لمس العملية الالتهابية العصبية التي تغذيه.
كيف يعمل علاج MSC لعرق النسا
عندما تُوصَّل MSC ذات الجودة السريرية إلى الحيز فوق الجافية بالقرب من جذر العصب المضغوط — عادةً عبر الحقن فوق الجافية عبر الثقبة بتوجيه التنظير الفلوري — تتفاعل مع البيئة الالتهابية من خلال عدة آليات منسقة:[4]
1. تحييد عاصفة السيتوكينات عند جذر العصب
تستشعر MSC التركيزات العالية من TNF-α وIL-1β وتستجيب بإطلاق وسائط قوية مضادة للالتهاب — TSG-6 وPGE2 وIL-10 وIDO. TSG-6 على وجه الخصوص يثبط مباشرة هجرة الخلايا المتعادلة، يقلل تنشيط البلاعم، ويُخمد سلسلة السيتوكينات في مصدرها. داخل الحيز فوق الجافية، يمكن أن يبدأ هذا في تقليل الألم الجذري والاضطرابات الحسية خلال الأسابيع الأولى بعد العلاج.
2. إطلاق عوامل مغذية للأعصاب وواقية للأعصاب
تفرز MSC عامل التغذية العصبية المشتق من الدماغ (BDNF)، عامل نمو العصب (NGF)، عامل التغذية العصبية المشتق من الخلايا الدبقية (GDNF)، وعامل النمو شبيه الأنسولين-1 (IGF-1) — جزيئات إشارة تدعم سلامة المحاور، تعزز نشاط خلايا شوان، وتحمي الخلايا العصبية من الاستماتة. عند جذر العصب المضغوط، يخلق هذا بيئة كيميائية حيوية تفضل الإصلاح العصبي على التدهور المستمر.[5]
3. تعديل الاستجابة المناعية المحلية
تعيد MSC برمجة البلاعم من النمط الظاهري الالتهابي M1 إلى النمط التجديدي M2. في سياق انفتاق القرص، يقلل هذا التحول من الاستجابة شبه المناعية الذاتية لمادة النواة اللبية المنكشفة، مخمداً الالتهاب المزمن الذي يديم الاعتلال الجذري لفترة طويلة بعد زوال الإصابة الميكانيكية الأولية.[6]
4. دعم الحفاظ على مصفوفة القرص
بينما الهدف الأساسي في عرق النسا هو جذر العصب، تفيد MSC أيضاً القرص المتدهور نفسه. العوامل شبه الإفرازية بما فيها TGF-β وBMP-7 تشير إلى خلايا القرص المقيمة للحفاظ على تصنيع البروتيوغليكان والكولاجين، مما قد يُبطئ تقدم تنكس القرص الكامن وراء الانفتاق المتكرر.[7]
ما لا يفعله علاج MSC لعرق النسا
التوقعات الصادقة مهمة. علاج MSC لا يزيل جسدياً قطعة قرص منفتق. لا يعكس متلازمة ذيل الفرس الشديدة، ولا يستعيد الوظيفة الحركية الكاملة في هبوط قدم طويل الأمد، ولا يصحح التضيق الشوكي المتقدم. ما يمكنه فعله هو تقليل الالتهاب العصبي المحرك للألم الجذري، دعم شفاء جذر العصب، وربما تجنب أو تأخير الحاجة إلى تخفيف الضغط الجراحي لدى مرضى مختارين بعناية مع انفتاق معتدل وأعراض مستمرة لم يتطوروا إلى عجز عصبي شديد.[8]
من هو المرشح الجيد لعلاج MSC في عرق النسا؟
أفضل النتائج تُرى لدى المرضى الذين يكون عرق النسا لديهم مدفوعاً بـالالتهاب العصبي بدلاً من الضغط الميكانيكي البحت. هؤلاء عادةً أفراد:[9]
- لديهم انفتاق قرص محتوى أو صغير إلى متوسط على MRI — وليس قطعة حرة كبيرة أو بثق كامل مع عزل
- يختبرون ألماً جذرياً في الساق مستمراً أو شبه مستمر، مما يشير إلى التهاب جذر كيميائي مستمر
- لم يستجيبوا بشكل كافٍ للعلاج المحافظ — العلاج الطبيعي، مضادات الالتهاب غير الستيرويدية، وحقنة ستيرويد فوق الجافية واحدة على الأقل
- يريدون تأخير أو تجنب جراحة استئصال القرص المجهري
- لا يعانون من ضعف حركي متقدم، متلازمة ذيل الفرس (خلل الأمعاء/المثانة، خدر السرج)، أو عدم استقرار فقري شديد — هذه تتطلب تقييماً جراحياً عاجلاً
دور الاستشارة — بما في ذلك مراجعة MRI شاملة وفحص عصبي وتقييم وظيفي — هو التمييز بين الاعتلال الجذري الالتهابي ومرض القرص الجراحي وتحديد ما إذا كان العلاج التجديدي مناسباً للمريض الفردي.
كيف تبدو عملية العلاج
في مركز ذي جودة سريرية، يتبع بروتوكول MSC النموذجي المرتكز على عرق النسا مساراً منظماً:
الخطوة 1: التقييم الشامل
MRI قطني، فحص عصبي (حسي، حركي، منعكسات)، تخطيط الألم، وتقييم المؤشرات الحيوية الالتهابية. الهدف هو تحديد المستوى الدقيق لإصابة جذر العصب — الأكثر شيوعاً L4–L5 أو L5–S1 — وتأكيد أن الالتهاب العصبي، وليس الضغط الميكانيكي الشديد أو عدم الاستقرار، هو المحرك الأساسي للأعراض.
الخطوة 2: تصميم البروتوكول
يصمم الفريق السريري النهج: حقن فوق الجافية عبر الثقبة بتوجيه التنظير الفلوري (الطريق المفضل لعرق النسا، لأنه يوصل MSC مباشرة إلى جذر العصب المصاب)، مع أو بدون تسريب وريدي تكميلي للدعم المضاد للالتهاب الجهازي. تُحدد الجرعة والتوقيت والعلاج الطبيعي المساعد بشكل فردي.
الخطوة 3: تسليم العلاج
يُجرى الحقن فوق الجافية عبر الثقبة تحت توجيه التنظير الفلوري أو CT في الوقت الحقيقي، ضامناً وضع MSC الدقيق عند واجهة جذر العصب–القرص. الإجراء خارجي، يستغرق 60–90 دقيقة بما في ذلك التحضير، ويغادر المرضى في نفس اليوم مع قيود نشاط خفيف.
الخطوة 4: التعافي وإعادة التأهيل
برنامج إعادة تأهيل منظم — بما في ذلك تمارين انزلاق العصب، تثبيت الجذع، إعادة تدريب الوضعية، والعودة التدريجية للنشاط — يكمل العلاج الخلوي. توصي معظم البروتوكولات بـ 48–72 ساعة من النشاط الخفيف متبوعة بعودة متدرجة إلى الحركة الطبيعية على مدى 2–4 أسابيع.
الخطوة 5: مراقبة النتائج
المتابعة في 4 و12 و24 أسبوعاً تتتبع الألم باستخدام مقاييس مُعتمَدة (مقياس التناظر البصري ومؤشر إعاقة Oswestry)، الوظيفة الحسية والحركية، جودة الحياة، وحيث يُشار سريرياً، إعادة MRI لتقييم حالة القرص وجذر العصب.
جداول زمنية واقعية: ماذا تتوقع ومتى
يتبع العلاج الخلوي جدولاً زمنياً بيولوجياً، لا دوائياً. يختبر معظم المرضى الاستجابة في ثلاث مراحل متداخلة:[10]
تعتمد النتائج على شدة انفتاق القرص، مدة الأعراض، إصابة جذر العصب، جودة MSC، بروتوكول الجرعات، وجودة برنامج إعادة التأهيل المحيط. ستكون العيادة ذات السمعة الجيدة شفافة بشأن نسبة المرضى الذين يختبرون فائدة قوية ومتوسطة ومحدودة.
السلامة وما يجب أن يعرفه كل مريض
عند التوصيل بخلايا ذات جودة سريرية، تقنية موجهة بالصورة، وإشراف سريري مناسب، يتمتع علاج MSC لعرق النسا بملف أمان ممتاز. الآثار الجانبية الأكثر شيوعاً هي موضعية: ألم مؤقت بعد الحقن، تيبس خفيف، أو زيادة وجيزة في عدم الراحة الجذرية لمدة 24–72 ساعة — مما يعكس على الأرجح الاستجابة الالتهابية الأولية للحقن نفسه. الأحداث السلبية الخطيرة نادرة في الأدبيات المنشورة عند استخدام خلايا بدرجة GMP وتوجيه التنظير الفلوري.[11]
أهم خطر يمكن منعه في هذا المجال ليس العلاج نفسه — بل المزودون غير المنظمين الذين يستخدمون خلايا غير سريرية الجودة بعقامة وهوية وفعالية غير متحقق منها. يجب على المرضى دائماً تأكيد: مصدر MSC وخصائصها (CD73/CD90/CD105 إيجابية ≥95%، CD45/CD34/CD14 إيجابية ≤2%)، اعتمادات المختبر (ISO، GMP)، والوصول إلى شهادة تحليل للجرعة المحددة المُعطاة.[12]
للمريض المناسب — انفتاق قرص محتوى يسبب اعتلالاً جذرياً مستمراً مع مكون التهابي — يمكن أن يقدم علاج MSC راحة ذات معنى دون عبء التعافي من الجراحة. المفتاح هو تقييم الأهلية الصادق قبل بدء العلاج.
— فريق VELAR السريري
منهج VELAR لعرق النسا
تبدأ بروتوكولات عرق النسا في VELAR Center بمراجعة MRI شاملة وفحص عصبي وتقييم المؤشرات الحيوية لرسم خريطة إصابة جذر العصب الدقيقة وتأكيد الأهلية. يستخدم كل بروتوكول MSC ذات جودة سريرية مشتقة من هلام وارتون (تعبير علامات MSC ≥95%، حيوية بعد الإذابة >90%)، تُوصَّل عبر الحقن فوق الجافية عبر الثقبة بتوجيه التنظير الفلوري — مع أو بدون تسريب وريدي حسب شدة الأعراض وتوزعها. تُقاد كل جلسة من قبل طبيب ذي خبرة، مقترنة بإعادة تأهيل عصبي منظم، ومُراقَبة عبر علامات 1 و3 و6 أشهر.[8]
إذا كنت تفكر في العلاج التجديدي لعرق النسا، فإن أهم خطوة أولى هي تقييم صادق لما إذا كان مرض قرصك المحدد ونمط أعراضك مرجحاً للاستجابة — وفهم واضح للنتائج الواقعية لمرحلة إصابة جذر العصب لديك.
الأسئلة الشائعة
كم تكلفة العلاج بالخلايا الجذعية لعرق النسا في تايلاند؟
يتراوح علاج MSC لعرق النسا في تايلاند عادةً من 6,000 إلى 12,000 دولار أمريكي حسب تعقيد البروتوكول (طرق توصيل مفردة مقابل مجتمعة)، جرعة الخلايا، وما إذا كان التسريب الوريدي المساعد مشمولاً. هذا أقل بكثير مما هو عليه في الولايات المتحدة أو أوروبا، حيث تتجاوز البروتوكولات المماثلة غالباً 20,000 دولار.
هل يمكن لعلاج MSC أن يحل محل جراحة الانفتاق القرصي؟
قد يقلل علاج MSC أو يلغي الحاجة إلى استئصال القرص المجهري لدى مرضى مختارين بعناية — أولئك الذين لديهم انفتاقات قرصية محتواة، اعتلال جذري التهابي، ولا عجز عصبي متقدم. لا يحل محل الجراحة للمرضى الذين لديهم قطع حرة كبيرة، متلازمة ذيل الفرس، أو ضعف حركي سريع التقدم. يحدد التقييم الصادق القائم على MRI أي مسار مناسب.
كم عدد حقن MSC المطلوبة لعرق النسا؟
تتضمن معظم البروتوكولات جلسة حقن واحدة عبر الثقبة فوق الجافية، أحياناً مع تسريب وريدي. قد يستفيد بعض المرضى ذوي الإصابة الثنائية أو متعددة المستويات من سلسلة من 2–3 جلسات بفاصل 4–8 أسابيع. يُحدد البروتوكول الدقيق بعد مراجعة MRI والفحص العصبي.
ما هو معدل نجاح العلاج بالخلايا الجذعية لعرق النسا؟
تفيد الدراسات المنشورة حول توصيل MSC فوق الجافية للاعتلال الجذري القرصي المنشأ بأن 60–75% من المرضى المختارين بعناية يختبرون تقليلاً ذا معنى سريري في الألم (تحسن ≥50% على VAS) ومكاسب وظيفية عند 6–12 شهراً. النتائج أقوى لدى المرضى ذوي الانفتاقات المحتواة، الأعراض ذات الغلبة الالتهابية، والأعراض الموجودة منذ أقل من سنتين.
هل علاج MSC لعرق النسا مؤلم؟
الحقن فوق الجافية عبر الثقبة نفسه يتضمن إعطاء مخدر موضعي وجيز متبوعاً بحقن MSC تحت التنظير الفلوري — يصفه معظم المرضى بأنه ضغط وليس ألماً. الألم بعد الإجراء في موقع الحقن وزيادة مؤقتة في عدم الراحة الجذرية لمدة 24–72 ساعة شائع ويختفي عادةً مع الراحة والثلج.
متى يمكنني العودة إلى العمل بعد علاج MSC لعرق النسا؟
يمكن عادةً استئناف العمل المكتبي خلال 2–3 أيام. قد تتطلب المهن ذات المتطلبات البدنية 2–4 أسابيع من المهام المعدلة. تتطور الاستجابة البيولوجية الكاملة لعلاج MSC على مدى 2–3 أشهر، لذا يُنصح بالعودة التدريجية للأنشطة عالية التأثير حتى لو تحسن الألم مبكراً.
المراجع
- Stafford MA, Peng P, Hill DA. Sciatica: a review of history, epidemiology, pathogenesis, and the role of epidural steroid injection in management. British Journal of Anaesthesia. 2007;99(4):461-473. doi:10.1093/bja/aem238 ↩
- Urits I, Capuco A, Sharma M, et al. Stem cell therapies for treatment of discogenic low back pain: a comprehensive review. Current Pain and Headache Reports. 2019;23(9):65. doi:10.1007/s11916-019-0804-y ↩
- Valat JP, Genevay S, Marty M, Rozenberg S, Koes B. Sciatica. Best Practice & Research Clinical Rheumatology. 2010;24(2):241-252. doi:10.1016/j.berh.2009.11.005 ↩
- Centeno C, Markle J, Dodson E, et al. Treatment of lumbar degenerative disc disease-associated radicular pain with culture-expanded autologous mesenchymal stem cells: a pilot study on safety and efficacy. Journal of Translational Medicine. 2017;15(1):197. doi:10.1186/s12967-017-1300-y ↩
- Wilkins A, Kemp K, Ginty M, Hares K, Mallam E, Scolding N. Human bone marrow-derived mesenchymal stem cells secrete brain-derived neurotrophic factor which promotes neuronal survival in vitro. Stem Cell Research. 2009;3(1):63-70. doi:10.1016/j.scr.2009.02.006 ↩
- Caplan AI, Correa D. The MSC: an injury drugstore. Cell Stem Cell. 2011;9(1):11-15. doi:10.1016/j.stem.2011.06.008 ↩
- Sakai D, Schol J. Cell therapy for intervertebral disc repair: clinical perspective. Journal of Orthopaedic Translation. 2017;9:8-18. doi:10.1016/j.jot.2017.02.002 ↩
- Meisel HJ, Agarwal N, Hsieh PC, et al. Cell therapy for treatment of intervertebral disc degeneration: a systematic review. Global Spine Journal. 2019;9(1 Suppl):39S-52S. doi:10.1177/2192568219829024 ↩
- Pettine KA, Murphy MB, Suzuki RK, Sand TT. Percutaneous injection of autologous bone marrow concentrate cells significantly reduces lumbar discogenic pain through 12 months. Stem Cells. 2015;33(1):146-156. doi:10.1002/stem.1845 ↩
- Noriega DC, Ardura F, Hernández-Ramajo R, et al. Intervertebral disc repair by allogeneic mesenchymal bone marrow cells: a randomized controlled trial. Transplantation. 2017;101(8):1945-1951. doi:10.1097/TP.0000000000001484 ↩
- Dominici M, Le Blanc K, Mueller I, et al. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy. 2006;8(4):315-317. doi:10.1080/14653240600855905 ↩
- Orozco L, Soler R, Morera C, Alberca M, Sánchez A, García-Sancho J. Intervertebral disc repair by autologous mesenchymal bone marrow cells: a pilot study. Transplantation. 2011;92(7):822-828. doi:10.1097/TP.0b013e3182298a15 ↩