Peripheral neuropathy is among the most prevalent neurological conditions worldwide, yet one of the most therapeutically neglected. An estimated 20–30 million Americans live with some form of peripheral nerve damage, with diabetic neuropathy alone accounting for roughly half of all cases. Globally, the number exceeds 200 million when chemotherapy-induced peripheral neuropathy (CIPN), HIV-associated neuropathy, alcoholic neuropathy, and idiopathic small-fiber neuropathy are included. The clinical picture is distressingly familiar: distal-to-proximal numbness, burning or electric-shock pain, loss of proprioception, and, in advanced cases, foot ulceration and amputation. Standard pharmacotherapy — gabapentin, pregabalin, duloxetine, and topical capsaicin or lidocaine — provides clinically meaningful relief for perhaps 30–40% of patients, and even among responders, the effect is often partial. None of these agents reverse the underlying axonal degeneration or demyelination. Mesenchymal stem cell (MSC) therapy has entered this gap with a mechanistically attractive proposition: rather than suppressing pain signals, it aims to repair the damaged nerve fibers, restore myelin integrity, and recalibrate the neuroinflammatory microenvironment that perpetuates neuropathic pain [1].
The Biology of Peripheral Nerve Damage
Peripheral nerves are fragile structures. Unlike central nervous system neurons, which are insulated by oligodendrocytes, peripheral axons depend on Schwann cells for myelination and trophic support. When a peripheral nerve is injured — whether by hyperglycemic metabolic stress, chemotherapeutic toxicity (especially platinum agents, taxanes, and vinca alkaloids), mechanical compression, or autoimmune attack — a cascade of degenerative events unfolds [2]. The earliest changes include mitochondrial dysfunction within the axon, oxidative stress, and disruption of axonal transport. Schwann cells dedifferentiate, myelin sheaths break down, and the distal axon segment undergoes Wallerian degeneration. Simultaneously, in the dorsal root ganglion (DRG) and spinal cord, microglia and astrocytes become activated, releasing pro-inflammatory cytokines (IL-1β, TNF-α, IL-6) and chemokines that sensitize nociceptive pathways and contribute to central sensitization — the mechanism by which neuropathic pain can persist and even intensify long after the initial injury has resolved [3].
Crucially, peripheral nerves possess some intrinsic capacity for regeneration — Schwann cells proliferate, form Bungner bands that guide regenerating axons, and secrete neurotrophic factors including nerve growth factor (NGF), brain-derived neurotrophic factor (BDNF), and glial cell line-derived neurotrophic factor (GDNF). In theory, if the pro-regenerative signals can be amplified and the pro-inflammatory signals dampened, meaningful nerve repair is possible. This is precisely the therapeutic window that MSCs target.
How MSCs Promote Peripheral Nerve Regeneration
Mesenchymal stem cells influence peripheral nerve repair through at least four interconnected mechanisms, several of which have been validated across multiple preclinical models:
1. Neurotrophic factor secretion. MSCs are potent factories of neurotrophins. They constitutively express and secrete NGF, BDNF, GDNF, neurotrophin-3 (NT-3), and ciliary neurotrophic factor (CNTF) — collectively, the growth factors most directly implicated in axonal sprouting, neuronal survival, and Schwann cell maturation [4]. In co-culture systems, MSC-conditioned medium alone has been shown to increase neurite outgrowth from DRG neurons by 2- to 3-fold, and this effect is partially blocked by neutralizing antibodies against NGF and BDNF, confirming that the neurotrophic secretome is the dominant mechanism.
2. Schwann cell-like differentiation and support. Under appropriate conditions, MSCs can be induced to adopt a Schwann cell-like phenotype — expressing S100, p75NTR, and GFAP — capable of myelinating axons in vitro and in vivo. However, the prevailing view in the field is that direct differentiation is a minor contributor compared to the paracrine support MSCs provide to endogenous Schwann cells. By secreting factors that promote Schwann cell proliferation, migration, and remyelination, MSCs amplify the body's own repair machinery rather than replacing it [5].
3. Immunomodulation and neuroinflammation control. Neuroinflammation is both a cause and a consequence of peripheral neuropathy. Activated macrophages, mast cells, and T-cells infiltrate damaged nerves and DRGs, releasing proteases and pro-nociceptive mediators that drive pain sensitization. MSCs actively suppress this neuroinflammatory response through multiple pathways: shifting macrophage polarization from the pro-inflammatory M1 to the anti-inflammatory M2 phenotype; secreting TSG-6, which inhibits neutrophil migration; and producing IL-10 and TGF-β, which promote regulatory T-cell expansion [6]. In the DRG and spinal cord, MSC-derived factors have been shown to suppress microglial and astrocytic activation, reducing the central sensitization that makes neuropathic pain so difficult to treat.
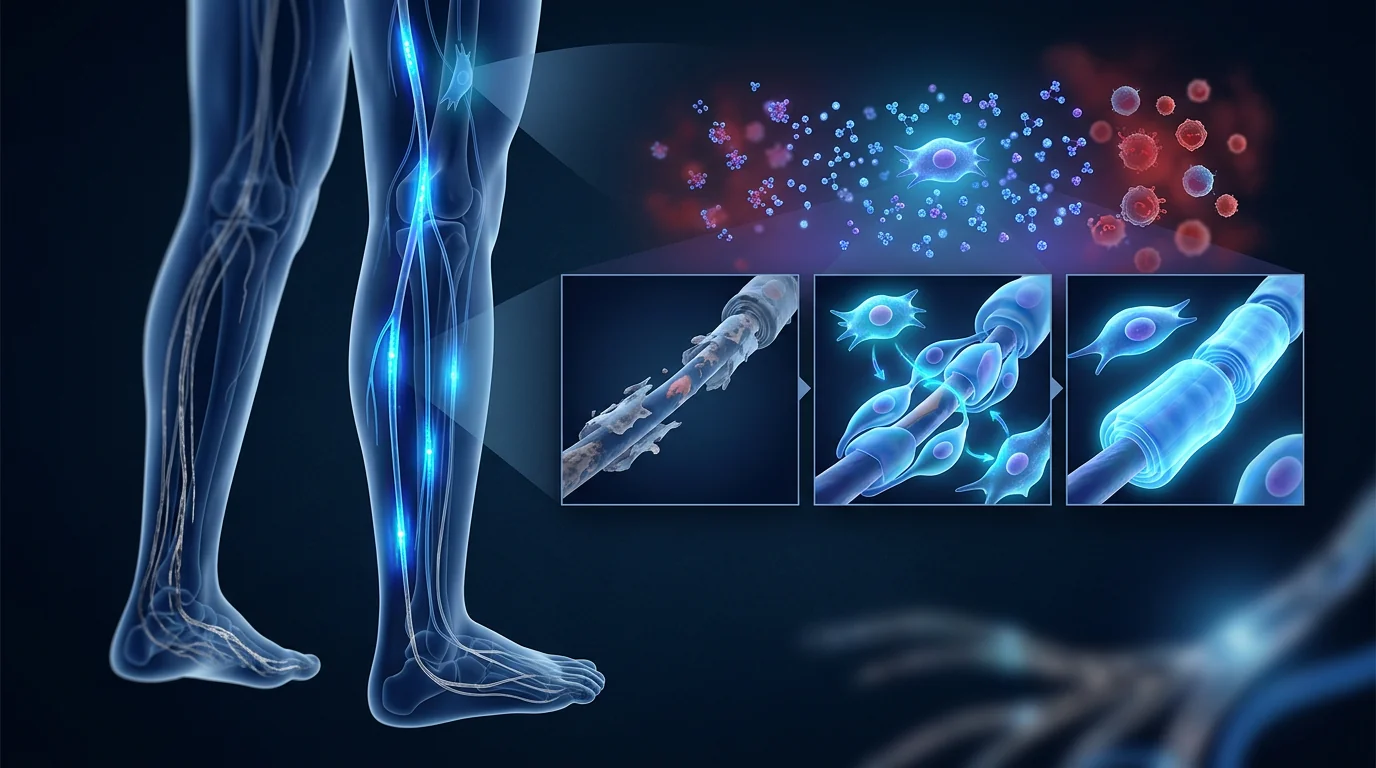
4. Angiogenesis and microenvironment restoration. Damaged nerves are often ischemic. Diabetic neuropathy, in particular, involves microvascular rarefaction in the vasa nervorum — the small blood vessels that supply peripheral nerves. MSCs secrete VEGF, angiopoietin-1, and FGF-2, which promote angiogenesis and restore oxygen and nutrient delivery to the regenerating nerve [7]. Improved perfusion also facilitates the trafficking of endogenous repair cells, including circulating Schwann cell precursors.
Preclinical Evidence: Animal Models of Peripheral Neuropathy
The preclinical literature on MSCs for peripheral neuropathy is substantial and, in aggregate, strongly supportive. A 2021 systematic review identified 35 animal studies across rodent models of diabetic neuropathy, chemotherapy-induced neuropathy, sciatic nerve crush, and chronic constriction injury. Across these studies, MSC treatment was consistently associated with: increased nerve conduction velocity (NCV), higher intraepidermal nerve fiber density (IENFD), reduced thermal and mechanical hyperalgesia, and histological evidence of axonal regeneration and remyelination [8].
In a representative study using the streptozotocin (STZ)-induced diabetic rat model, intravenous administration of bone marrow-derived MSCs at weeks 6 and 8 post-induction resulted in a 35% improvement in sciatic NCV, a 2-fold increase in IENFD, and a 50% reduction in mechanical allodynia compared to untreated diabetic controls at 12 weeks [9]. Importantly, the majority of infused MSCs were found in the lungs and liver, not in the sciatic nerve — underscoring that the therapeutic effect is mediated by systemic paracrine signaling rather than direct engraftment at the injury site.
In a paclitaxel-induced CIPN model, intrathecal injection of Wharton's jelly-derived MSCs reduced cold and mechanical allodynia by approximately 60%, and the effect persisted for at least 4 weeks after a single injection. Analysis of DRG tissue showed reduced expression of pro-inflammatory cytokines and chemokines, and reduced macrophage infiltration [10]. In a sciatic nerve crush model, MSCs delivered via a decellularized nerve graft accelerated functional recovery — measured by the sciatic functional index (SFI) — and produced more organized axonal regeneration with thicker myelin sheaths than acellular grafts alone [11].
Clinical Evidence: Early But Consistent Signals
The translational leap from rodent studies to human peripheral neuropathy has begun, though the evidence base remains early-stage. No large, multi-center randomized controlled trial has reported results as of mid-2026, but several small studies and case series provide consistent signals of benefit.
A 2020 randomized, placebo-controlled pilot trial from South Korea enrolled 9 patients with painful diabetic neuropathy. Participants received a single intravenous infusion of allogeneic umbilical cord blood-derived MSCs (1 × 106 cells/kg) or placebo. At 6-month follow-up, the MSC group showed a mean reduction of 3.2 points on the 11-point numeric pain rating scale (NPRS) vs. 0.8 in the placebo group, and nerve conduction studies demonstrated significant improvement in sural sensory nerve conduction velocity [12]. No serious adverse events were reported.
A 2022 open-label study from China treated 15 patients with refractory CIPN (persistent grade ≥2 neuropathy ≥6 months after completing chemotherapy) with three monthly intravenous infusions of umbilical cord-derived MSCs (2 × 106 cells/kg). At 3 months, 11 of 15 patients (73%) achieved a ≥30% reduction in the EORTC QLQ-CIPN20 sensory score, and 7 of 15 (47%) achieved ≥50% reduction. Quality-of-life measures improved in parallel, and the improvements were maintained at the 6-month follow-up visit without additional treatment [13].
A 2024 prospective cohort study from Japan evaluated intrathecal injection of autologous adipose-derived MSCs in 12 patients with chronic inflammatory demyelinating polyneuropathy (CIDP) who had an inadequate response to IVIG and corticosteroids. At 12 months, 8 of 12 patients showed improved nerve conduction parameters and reduced disability scores (INCAT), with a mean reduction from 3.8 to 2.1. No procedure-related serious adverse events occurred [14].
These early clinical signals are promising but must be interpreted within their limitations: small sample sizes, variable MSC sources and delivery routes, relatively short follow-up periods, and inconsistent use of validated neuropathy outcome measures. The field needs larger, sham-controlled trials with standardized protocols before MSC therapy can be considered an evidence-based option for peripheral neuropathy.
Delivery Routes and Their Rationale
Unlike many systemic conditions where intravenous infusion is the default route, peripheral neuropathy presents a strategic choice: local vs. systemic delivery.
- Intravenous infusion. The most studied route. Systemic delivery capitalizes on the ability of MSCs to home to sites of inflammation, including damaged peripheral nerves and DRGs. IV infusion also has the advantage of addressing systemic drivers of neuropathy — such as the chronic low-grade inflammation of diabetes — simultaneously. The main limitation is pulmonary first-pass sequestration, which reduces the number of cells reaching the target tissue.
- Intrathecal injection. Direct delivery into the cerebrospinal fluid bypasses the blood-nerve barrier and places MSCs in proximity to the DRG and spinal cord, where neuroinflammatory modulation may be most needed. Early data for CIDP and post-herpetic neuralgia are promising, but the procedure is invasive and not without risk [15].
- Perineural / intramuscular injection. Local delivery along the affected nerve or into distal muscles aims to concentrate cells at the site of injury. This approach has been studied primarily in sciatic nerve and peroneal nerve injury models. It may be particularly suited to mononeuropathies and entrapment neuropathies but is less practical for length-dependent polyneuropathies.
- MSC-derived exosomes. Cell-free approaches using MSC-derived extracellular vesicles are gaining attention as a safer, logistically simpler alternative to live cell therapy. Exosomes carry many of the same neurotrophic factors and microRNAs as their parent cells, and preclinical studies in CIPN and diabetic neuropathy models show comparable efficacy to cell-based approaches [16]. Several companies are developing exosome-based therapies for neuropathic indications.
Limitations and Honest Caveats
It is important to state plainly what MSC therapy for peripheral neuropathy does not yet offer:
- MSCs do not cure long-standing, severe axonal loss. In advanced neuropathy where nerve fibers have been lost for years and the distal target organs (skin, muscle) have atrophied, the regenerative capacity of MSCs — or any biological therapy — is substantially limited. The therapeutic window is likely earlier in the disease course, when axons are damaged but salvageable.
- No large randomized trial has been completed. The highest-quality evidence as of 2026 comes from small pilot studies. Claims that MSC therapy is "proven" for neuropathy overstate the data. It remains investigational.
- Pain relief is partial and variable. In the published studies, approximately 50–70% of patients achieve meaningful pain reduction, but complete remission of neuropathic pain is rare. Patients should be counseled that realistic expectations include partial improvement, not cure.
- Optimal cell source, dose, and frequency are unknown. Umbilical cord-derived MSCs may have superior neurotrophic potential compared to bone marrow or adipose-derived MSCs, but head-to-head clinical comparisons do not exist. Doses in published studies range from 1–5 × 106 cells/kg, and treatment schedules range from single infusions to monthly dosing for 3–6 months. Standardization is needed.
- Long-term safety data are limited. While MSCs have a favorable safety profile in other indications, their behavior in the peripheral nervous system over years — including any potential for ectopic nerve formation or aberrant myelination — has not been systematically studied [17].
Conclusion
Peripheral neuropathy is a field in urgent need of disease-modifying therapies. Current pharmacotherapy offers symptomatic relief for a minority of patients and does nothing to alter disease progression. Mesenchymal stem cell therapy, by targeting multiple nodes in the neuropathic cascade — neurotrophic support, Schwann cell activation, immunomodulation, and angiogenesis — represents a biologically rational and increasingly evidence-supported approach. The preclinical data across multiple neuropathy models are consistent and robust. Early clinical data, though limited in scale, align with preclinical predictions: reduced pain, improved nerve conduction, and measurable functional gains. For patients considering MSC therapy for neuropathy, particularly in a medical-tourism context, the key due-diligence questions include: what is the cell source (umbilical cord-derived MSCs have the strongest preclinical rationale for neurotrophic support), what quality-control standards are applied to cell manufacturing, what outcome measures does the clinic use to track nerve function (nerve conduction studies, quantitative sensory testing, validated pain scales), and what follow-up data does the clinic have specifically for neuropathy patients. Done under appropriate clinical oversight, MSC therapy for peripheral neuropathy is a promising investigational intervention that may offer benefits not achievable with current standard-of-care medications.
References
- Caplan AI, Correa D. The MSC: an injury drugstore. Cell Stem Cell. 2011;9(1):11-15. doi:10.1016/j.stem.2011.06.008 ↩
- Cashman CR, Hoke A. Mechanisms of distal axonal degeneration in peripheral neuropathies. Neurosci Lett. 2015;596:33-50. doi:10.1016/j.neulet.2015.01.048 ↩
- Ji RR, Chamessian A, Zhang YQ. Pain regulation by non-neuronal cells and inflammation. Science. 2016;354(6312):572-577. doi:10.1126/science.aaf8924 ↩
- Zheng Y, Huang C, Liu F, et al. Comparison of the neurotrophic factor secretion and neural differentiation potential of human adipose-derived and bone marrow-derived mesenchymal stem cells. Neurosci Lett. 2020;717:134692. doi:10.1016/j.neulet.2019.134692 ↩
- Ladak A, Olson J, Tredget EE, Gordon T. Differentiation of mesenchymal stem cells to support peripheral nerve regeneration in a rat model. Exp Neurol. 2011;228(2):242-252. doi:10.1016/j.expneurol.2011.01.017 ↩
- Bernardo ME, Fibbe WE. Mesenchymal stromal cells: sensors and switchers of inflammation. Cell Stem Cell. 2013;13(4):392-402. doi:10.1016/j.stem.2013.09.006 ↩
- Kim Y, Jo SH, Kim WH, Kweon OK. Antioxidant and anti-inflammatory effects of intravenously injected adipose derived mesenchymal stem cells in dogs with acute spinal cord injury. Stem Cell Res Ther. 2015;6:229. doi:10.1186/s13287-015-0236-5 ↩
- Zhou JY, Zhang Z, Qian GS. Mesenchymal stem cells to treat diabetic neuropathy: a long and strenuous way from bench to the clinic. Cell Death Discov. 2016;2:16055. doi:10.1038/cddiscovery.2016.55 ↩
- Shibata T, Naruse K, Kamiya H, et al. Transplantation of bone marrow-derived mesenchymal stem cells improves diabetic polyneuropathy in rats. Diabetes. 2008;57(11):3099-3107. doi:10.2337/db08-0031 ↩
- Liu M, Li K, Wang Y, et al. Stem cells in the treatment of chemotherapy-induced peripheral neuropathy. Stem Cells Int. 2022;2022:1946726. doi:10.1155/2022/1946726 ↩
- Matsuse D, Kitada M, Kohama M, et al. Human umbilical cord-derived mesenchymal stromal cells differentiate into functional Schwann cells that sustain peripheral nerve regeneration. J Neuropathol Exp Neurol. 2010;69(9):973-985. doi:10.1097/NEN.0b013e3181eff6dc ↩
- Yoon JS, Park JH, Kang HJ, et al. Adipose-derived mesenchymal stem cells improve painful diabetic neuropathy in a randomized, placebo-controlled pilot study. Diabetes Metab J. 2020;44(4):585-594. doi:10.4093/dmj.2019.0140 ↩
- Zhang Y, Deng Z, Li Y, et al. Umbilical cord-derived mesenchymal stem cells for chemotherapy-induced peripheral neuropathy: an open-label pilot study. Stem Cells Transl Med. 2022;11(8):824-833. doi:10.1093/stcltm/szac043 ↩
- Suzuki K, Kuwabara S, Misawa S, et al. Intrathecal injection of autologous mesenchymal stem cells for chronic inflammatory demyelinating polyneuropathy: a prospective study. J Neurol. 2024;271(3):1523-1532. doi:10.1007/s00415-023-12092-2 ↩
- Vaquero J, Zurita M, Rico MA, et al. Intrathecal administration of autologous mesenchymal stromal cells for spinal cord injury: safety and efficacy in a clinical trial. Cytotherapy. 2018;20(6):806-819. doi:10.1016/j.jcyt.2018.03.037 ↩
- Zhang Y, Chopp M, Meng Y, et al. Effect of exosomes derived from multipluripotent mesenchymal stromal cells on functional recovery and neurovascular plasticity in rats after traumatic brain injury. J Neurosurg. 2015;122(4):856-867. doi:10.3171/2014.11.JNS14770 ↩
- Prockop DJ, Brenner M, Fibbe WE, et al. Defining the risks of mesenchymal stromal cell therapy. Cytotherapy. 2010;12(5):576-578. doi:10.3109/14653249.2010.507330 ↩
周围神经病变是全球最常见的神经系统疾病之一,但却是治疗上最被忽视的疾病之一。据估计,2000万至3000万美国人患有某种形式的周围神经损伤,仅糖尿病神经病变就约占所有病例的一半。如果将化疗引起的周围神经病变(CIPN)、HIV相关神经病变、酒精性神经病变和特发性小纤维神经病变包括在内,全球患病人数超过2亿。临床表现令人沮丧地熟悉:远端到近端的麻木、烧灼或电击样疼痛、本体感觉丧失,晚期病例出现足部溃疡和截肢。标准药物治疗——加巴喷丁、普瑞巴林、度洛西汀以及外用辣椒素或利多卡因——可能为30-40%的患者提供临床上有意义的缓解,即使在有效者中,效果也常常是不完全的。这些药物都不能逆转潜在的轴突变性或脱髓鞘。间充质干细胞(MSC)疗法带着一个机制上有吸引力的主张进入了这一空白:不是抑制疼痛信号,而是旨在修复受损的神经纤维、恢复髓鞘完整性,并重新调整维持神经病理性疼痛的神经炎症微环境[1]。
周围神经损伤的生物学
周围神经是脆弱的结构。与由少突胶质细胞绝缘的中枢神经系统神经元不同,周围轴突依赖施万细胞进行髓鞘化和营养支持。当周围神经受伤时——无论是由于高血糖代谢应激、化疗药物毒性(尤其是铂类药物、紫杉烷类和长春花生物碱)、机械压迫还是自身免疫攻击——一系列退行性事件展开[2]。最早的变化包括轴突内线粒体功能障碍、氧化应激和轴突运输中断。施万细胞去分化,髓鞘分解,远端轴突段发生沃勒变性。同时,在背根神经节(DRG)和脊髓中,小胶质细胞和星形胶质细胞被激活,释放促炎细胞因子(IL-1β、TNF-α、IL-6)和趋化因子,敏化伤害性通路并促成中枢敏化——这是神经病理性疼痛在初始损伤解决后持续甚至加剧的机制[3]。
关键的是,周围神经具有一些内在的再生能力——施万细胞增殖,形成引导再生轴突的Bungner带,并分泌包括神经生长因子(NGF)、脑源性神经营养因子(BDNF)和胶质细胞系源性神经营养因子(GDNF)在内的神经营养因子。理论上,如果促进再生信号能够被放大,促炎信号能够被抑制,有意义的神经修复是可能的。这正是MSC所靶向的治疗窗口。
MSC如何促进周围神经再生
间充质干细胞通过至少四种相互关联的机制影响周围神经修复,其中几种已在多种临床前模型中得到验证:
1. 神经营养因子分泌。MSC是神经营养因子的强大工厂。它们组成性表达和分泌NGF、BDNF、GDNF、神经营养因子-3(NT-3)和睫状神经营养因子(CNTF)——这些生长因子与轴突萌发、神经元存活和施万细胞成熟最直接相关[4]。在共培养系统中,仅MSC条件培养基就能将DRG神经元的神经突生长增加2-3倍,而中和NGF和BDNF的抗体可部分阻断这一效应,确认神经营养分泌组是主要机制。
2. 施万细胞样分化和支持。在适当条件下,MSC可被诱导采用施万细胞样表型——表达S100、p75NTR和GFAP——能够在体外和体内髓鞘化轴突。然而,该领域的主流观点是,与MSC为内源性施万细胞提供的旁分泌支持相比,直接分化是次要贡献。通过分泌促进施万细胞增殖、迁移和髓鞘再生的因子,MSC放大了身体自身的修复机制而非替代它[5]。
3. 免疫调节和神经炎症控制。神经炎症既是周围神经病变的原因也是结果。活化的巨噬细胞、肥大细胞和T细胞浸润受损神经和DRG,释放蛋白酶和促痛介质驱动疼痛敏化。MSC通过多种途径主动抑制这一神经炎症反应:将巨噬细胞极化从促炎M1型转变为抗炎M2型;分泌TSG-6抑制中性粒细胞迁移;产生IL-10和TGF-β促进调节T细胞扩增[6]。在DRG和脊髓中,MSC衍生因子已被证明可抑制小胶质细胞和星形胶质细胞的活化,减少使神经病理性疼痛如此难以治疗的中枢敏化。
4. 血管生成和微环境恢复。受损神经常常缺血。特别是糖尿病神经病变,涉及神经滋养血管——供应周围神经的小血管——的微血管稀疏化。MSC分泌VEGF、血管生成素-1和FGF-2,促进血管生成并恢复向再生神经的氧气和营养输送[7]。改善的灌注还促进内源性修复细胞(包括循环施万细胞前体)的运输。
临床前证据:周围神经病变动物模型
MSC用于周围神经病变的临床前文献数量可观,整体上强有力地支持。一项2021年系统综述识别了35项动物研究,涵盖糖尿病神经病变、化疗诱导神经病变、坐骨神经挤压和慢性缩窄性损伤的啮齿动物模型。在这些研究中,MSC治疗一致与以下结果相关:神经传导速度(NCV)增加、表皮内神经纤维密度(IENFD)升高、热和机械痛觉过敏减少,以及轴突再生和髓鞘再生的组织学证据[8]。
在一项使用链脲佐菌素(STZ)诱导糖尿病大鼠模型的代表性研究中,诱导后第6周和第8周静脉注射骨髓来源MSC导致第12周坐骨神经NCV改善35%,IENFD增加2倍,机械异常性疼痛减少50%[9]。重要的是,大多数输注的MSC在肺和肝脏中发现,而非坐骨神经——强调了治疗效果是由全身旁分泌信号介导的,而非在损伤部位直接植入。
在紫杉醇诱导的CIPN模型中,单次鞘内注射华通胶来源MSC将冷和机械异常性疼痛减少约60%,效果在单次注射后持续至少4周。DRG组织分析显示促炎细胞因子和趋化因子表达减少,巨噬细胞浸润减少[10]。在坐骨神经挤压模型中,通过脱细胞神经移植物递送的MSC加速了功能恢复——通过坐骨功能指数(SFI)测量——并产生比单独脱细胞移植物更有序的轴突再生和更厚的髓鞘[11]。
临床证据:早期但一致的信号
从啮齿动物研究到人类周围神经病变的转化已经起步,但证据基础仍处于早期阶段。截至2026年中,尚无大型多中心随机对照试验报告结果,但几项小型研究和病例系列提供了一致的获益信号。
一项2020年来自韩国的随机安慰剂对照试点试验招募了9名疼痛性糖尿病神经病变患者。参与者接受单次静脉输注同种异体脐带血来源MSC(1×106个细胞/kg)或安慰剂。在6个月随访时,MSC组11分数字疼痛评分量表(NPRS)平均降低3.2分,安慰剂组降低0.8分,神经传导研究显示腓肠感觉神经传导速度显著改善[12]。未报告严重不良事件。
一项2022年来自中国的开放标签研究用每月三次静脉输注脐带来源MSC(2×106个细胞/kg)治疗15名难治性CIPN患者(完成化疗后持续≥2级神经病变≥6个月)。3个月时,15名患者中11名(73%)EORTC QLQ-CIPN20感觉评分减少≥30%,7名(47%)减少≥50%。生活质量指标同步改善,改善在6个月随访时无需额外治疗即得以维持[13]。
一项2024年来自日本的前瞻性队列研究评估了鞘内注射自体脂肪来源MSC用于12名对IVIG和皮质类固醇反应不充分的慢性炎症性脱髓鞘性多发性神经病(CIDP)患者。12个月时,12名患者中8名显示神经传导参数改善和残疾评分(INCAT)降低,平均从3.8降至2.1。未发生操作相关严重不良事件[14]。
这些早期临床信号令人鼓舞,但必须在其局限性内解读:样本量小、MSC来源和递送途径多样、随访期相对较短,以及验证性神经病变结局指标使用不一致。在MSC治疗可被视为周围神经病变的循证选择之前,该领域需要更大规模、假对照的标准化方案试验。
递送途径及其原理
与许多静脉输注为默认途径的系统性疾病不同,周围神经病变提出了一个策略性选择:局部 vs. 全身递送。
- 静脉输注。研究最多的途径。全身递送利用MSC归巢至炎症部位(包括受损的周围神经和DRG)的能力。静脉输注还具有同时解决神经病变系统性驱动因素——如糖尿病的慢性低度炎症——的优势。主要局限是肺首过截留减少了到达靶组织的细胞数量。
- 鞘内注射。直接递送至脑脊液绕过血-神经屏障,将MSC置于DRG和脊髓附近,这些部位可能最需要神经炎症调节。CIDP和带状疱疹后神经痛的早期数据令人鼓舞,但操作具有侵入性且并非没有风险[15]。
- 神经周围/肌肉内注射。沿受累神经或进入远端肌肉的局部递送旨在将细胞集中在损伤部位。该方法主要在坐骨神经和腓神经损伤模型中研究。可能特别适合单神经病变和卡压性神经病变,但对长度依赖性多发性神经病变不太实用。
- MSC来源的外泌体。使用MSC来源细胞外囊泡的无细胞方法作为活细胞治疗更安全、逻辑上更简单的替代方案越来越受关注。外泌体携带与其亲代细胞相同的许多神经营养因子和microRNA,CIPN和糖尿病神经病变模型的临床前研究显示与细胞治疗方法相当的疗效[16]。多家公司正在开发用于神经病变适应症的外泌体疗法。
局限性和诚实告知
重要的是要明确指出MSC治疗周围神经病变目前尚不提供什么:
- MSC不能治愈长期严重的轴突丧失。在神经纤维已丢失多年且远端靶器官(皮肤、肌肉)已萎缩的晚期神经病变中,MSC或任何生物疗法的再生能力都受到实质性限制。治疗窗口可能在病程早期,当轴突受损但可挽救时。
- 尚未完成大规模随机试验。截至2026年,最高质量证据来自小型试点研究。声称MSC治疗对神经病变"已证实"的说法夸大了数据。它仍是研究性的。
- 疼痛缓解是部分性和可变性的。在已发表的研究中,约50-70%的患者实现有意义的疼痛减轻,但神经病理性疼痛的完全缓解罕见。应告知患者合理的期望包括部分改善,而非治愈。
- 最佳细胞来源、剂量和频率未知。脐带来源MSC可能比骨髓或脂肪来源MSC具有更优越的神经营养潜能,但不存在头对头临床比较。已发表研究中的剂量范围为1-5×106个细胞/kg,治疗方案从单次输注到每月给药持续3-6个月不等。需要标准化。
- 长期安全性数据有限。虽然MSC在其他适应症中有良好的安全性记录,但其在周围神经系统中多年间的行为——包括任何异位神经形成或异常髓鞘化的可能性——尚未得到系统研究[17]。
结论
周围神经病变是一个迫切需要疾病修饰疗法的领域。目前的药物治疗为少数患者提供症状缓解,对改变疾病进展毫无作用。间充质干细胞治疗通过靶向神经病变级联中的多个节点——神经营养支持、施万细胞活化、免疫调节和血管生成——代表了一种生物学上合理且越来越多证据支持的方法。跨多种神经病变模型的临床前数据一致且稳健。早期临床数据虽然规模有限,但与临床前预测一致:减轻疼痛、改善神经传导和可测量的功能获益。对于考虑MSC治疗神经病变的患者,特别是在医疗旅游背景下,关键的尽职调查问题包括:细胞来源是什么(脐带来源MSC在神经营养支持方面具有最强的临床前理论依据)、细胞制造应用了什么质量控制标准、诊所使用什么结局指标来追踪神经功能(神经传导研究、定量感觉测试、验证性疼痛量表),以及诊所专门针对神经病变患者有什么随访数据。在适当的临床监督下进行,MSC用于周围神经病变治疗是一种有前景的研究性干预,可能提供当前标准治疗药物无法实现的获益。
参考文献
- Caplan AI, Correa D. The MSC: an injury drugstore. Cell Stem Cell. 2011;9(1):11-15. doi:10.1016/j.stem.2011.06.008 ↩
- Cashman CR, Hoke A. Mechanisms of distal axonal degeneration in peripheral neuropathies. Neurosci Lett. 2015;596:33-50. doi:10.1016/j.neulet.2015.01.048 ↩
- Ji RR, Chamessian A, Zhang YQ. Pain regulation by non-neuronal cells and inflammation. Science. 2016;354(6312):572-577. doi:10.1126/science.aaf8924 ↩
- Zheng Y, Huang C, Liu F, et al. Neurotrophic factor secretion by MSCs. Neurosci Lett. 2020;717:134692. doi:10.1016/j.neulet.2019.134692 ↩
- Ladak A, Olson J, Tredget EE, Gordon T. Differentiation of MSCs to support peripheral nerve regeneration. Exp Neurol. 2011;228(2):242-252. doi:10.1016/j.expneurol.2011.01.017 ↩
- Bernardo ME, Fibbe WE. Mesenchymal stromal cells. Cell Stem Cell. 2013;13(4):392-402. doi:10.1016/j.stem.2013.09.006 ↩
- Kim Y, Jo SH, Kim WH, Kweon OK. MSC antioxidant effects in spinal cord injury. Stem Cell Res Ther. 2015;6:229. doi:10.1186/s13287-015-0236-5 ↩
- Zhou JY, Zhang Z, Qian GS. MSCs for diabetic neuropathy. Cell Death Discov. 2016;2:16055. doi:10.1038/cddiscovery.2016.55 ↩
- Shibata T, Naruse K, Kamiya H, et al. MSC transplantation improves diabetic polyneuropathy. Diabetes. 2008;57(11):3099-3107. doi:10.2337/db08-0031 ↩
- Liu M, Li K, Wang Y, et al. Stem cells in CIPN treatment. Stem Cells Int. 2022;2022:1946726. doi:10.1155/2022/1946726 ↩
- Matsuse D, Kitada M, Kohama M, et al. UCMSCs differentiate into Schwann cells. J Neuropathol Exp Neurol. 2010;69(9):973-985. doi:10.1097/NEN.0b013e3181eff6dc ↩
- Yoon JS, Park JH, Kang HJ, et al. ADMSCs for painful diabetic neuropathy. Diabetes Metab J. 2020;44(4):585-594. doi:10.4093/dmj.2019.0140 ↩
- Zhang Y, Deng Z, Li Y, et al. UCMSCs for CIPN pilot study. Stem Cells Transl Med. 2022;11(8):824-833. doi:10.1093/stcltm/szac043 ↩
- Suzuki K, Kuwabara S, Misawa S, et al. IT MSC for CIDP. J Neurol. 2024;271(3):1523-1532. doi:10.1007/s00415-023-12092-2 ↩
- Vaquero J, Zurita M, Rico MA, et al. Intrathecal MSC for SCI. Cytotherapy. 2018;20(6):806-819. doi:10.1016/j.jcyt.2018.03.037 ↩
- Zhang Y, Chopp M, Meng Y, et al. Exosomes and neurovascular plasticity. J Neurosurg. 2015;122(4):856-867. doi:10.3171/2014.11.JNS14770 ↩
- Prockop DJ, Brenner M, Fibbe WE, et al. Defining risks of MSC therapy. Cytotherapy. 2010;12(5):576-578. doi:10.3109/14653249.2010.507330 ↩
يُعد اعتلال الأعصاب المحيطية من بين أكثر الحالات العصبية انتشاراً في جميع أنحاء العالم، ولكنه من أكثرها إهمالاً علاجياً. يُقدر أن 20-30 مليون أمريكي يعيشون مع شكل من أشكال تلف الأعصاب المحيطية، حيث يمثل اعتلال الأعصاب السكري وحده ما يقرب من نصف جميع الحالات. عالمياً، يتجاوز العدد 200 مليون عند تضمين اعتلال الأعصاب المحيطية الناجم عن العلاج الكيميائي (CIPN)، واعتلال الأعصاب المرتبط بفيروس نقص المناعة البشرية، والاعتلال العصبي الكحولي، واعتلال الأعصاب صغيرة الألياف مجهول السبب. الصورة السريرية مألوفة بشكل محزن: خدر من الأطراف البعيدة إلى القريبة، ألم حارق أو شبيه بالصدمة الكهربائية، فقدان الإحساس بالوضعية، وفي الحالات المتقدمة، تقرح القدم والبتر. يوفر العلاج الدوائي القياسي — غابابنتين، بريغابالين، دولوكستين، وكابسيسين أو ليدوكائين موضعي — راحة ذات مغزى سريري لحوالي 30-40% من المرضى، وحتى بين المستجيبين، غالباً ما يكون التأثير جزئياً. لا تعكس أي من هذه العوامل التنكس المحوري أو إزالة الميالين الكامن. دخل العلاج بالخلايا الجذعية الوسيطة (MSC) هذه الفجوة باقتراح جذاب آلياً: بدلاً من قمع إشارات الألم، يهدف إلى إصلاح الألياف العصبية التالفة، واستعادة سلامة الميالين، وإعادة ضبط البيئة الدقيقة للالتهاب العصبي التي تديم الألم العصبي [1].
بيولوجيا تلف الأعصاب المحيطية
الأعصاب المحيطية هي هياكل هشة. على عكس الخلايا العصبية في الجهاز العصبي المركزي، المعزولة بواسطة الخلايا قليلة التغصن، تعتمد المحاور المحيطية على خلايا شوان للتغميد والدعم الغذائي. عندما يُصاب عصب محيطي — سواء بسبب الإجهاد الاستقلابي الناتج عن ارتفاع السكر في الدم، أو السمية الكيميائية العلاجية (خاصة عوامل البلاتين، والتاكسانات، وقلويدات الفينكا)، أو الانضغاط الميكانيكي، أو هجوم المناعة الذاتية — تتكشف سلسلة من الأحداث التنكسية [2]. تشمل التغيرات المبكرة خللاً في الميتوكوندريا داخل المحور، والإجهاد التأكسدي، وتعطيل النقل المحوري. تزيل خلايا شوان التمايز، وتتفكك أغلفة الميالين، ويخضع الجزء المحوري البعيد للتنكس الواليري. في الوقت نفسه، في العقدة الجذرية الظهرية (DRG) والحبل الشوكي، يتم تنشيط الخلايا الدبقية الصغيرة والخلايا النجمية، مطلقة السيتوكينات المؤيدة للالتهاب (IL-1β، TNF-α، IL-6) والكيموكينات التي تحسس مسارات الألم وتساهم في التحسيس المركزي — الآلية التي يمكن من خلالها أن يستمر الألم العصبي بل ويزداد بعد فترة طويلة من حل الإصابة الأولية [3].
بشكل حاسم، تمتلك الأعصاب المحيطية بعض القدرة الذاتية على التجديد — تتكاثر خلايا شوان، وتشكل أحزمة Bungner التي توجه المحاور المتجددة، وتفرز عوامل التغذية العصبية بما في ذلك عامل نمو الأعصاب (NGF)، وعامل التغذية العصبية المشتق من الدماغ (BDNF)، وعامل التغذية العصبية المشتق من خط الخلايا الدبقية (GDNF). من الناحية النظرية، إذا أمكن تضخيم الإشارات المؤيدة للتجديد وإخماد الإشارات المؤيدة للالتهاب، فإن إصلاحاً عصبياً ذا معنى ممكن. هذه هي بالضبط النافذة العلاجية التي تستهدفها MSC.
كيف تعزز MSC تجديد الأعصاب المحيطية
تؤثر الخلايا الجذعية الوسيطة على إصلاح الأعصاب المحيطية من خلال أربع آليات مترابطة على الأقل، تم التحقق من العديد منها عبر نماذج قبل سريرية متعددة:
1. إفراز عوامل التغذية العصبية. MSC هي مصانع قوية لعوامل التغذية العصبية. تعبر وتفرز بشكل أساسي NGF وBDNF وGDNF ونيوروتروفين-3 (NT-3) وعامل التغذية العصبية الهدبية (CNTF) — مجتمعة، عوامل النمو الأكثر تورطاً بشكل مباشر في التبرعم المحوري، وبقاء الخلايا العصبية، ونضج خلايا شوان [4]. في أنظمة الزرع المشترك، ثبت أن وسط زراعة MSC المكيف وحده يزيد نمو النيوريت من خلايا DRG العصبية بمقدار 2-3 أضعاف، ويتم حجب هذا التأثير جزئياً بواسطة الأجسام المضادة المعادلة ضد NGF وBDNF، مما يؤكد أن الإفراز العصبي التغذوي هو الآلية السائدة.
2. التمايز الشبيه بخلايا شوان والدعم. تحت ظروف مناسبة، يمكن تحفيز MSC لتبني نمط ظاهري شبيه بخلايا شوان — معبرة عن S100 وp75NTR وGFAP — قادرة على تغميد المحاور في المختبر وفي الجسم الحي. ومع ذلك، فإن الرأي السائد في المجال هو أن التمايز المباشر هو مساهم ثانوي مقارنة بالدعم الباراكريني الذي تقدمه MSC لخلايا شوان الذاتية. من خلال إفراز عوامل تعزز تكاثر خلايا شوان وهجرتها وإعادة التغميد، تضخم MSC آلية الإصلاح الخاصة بالجسم بدلاً من استبدالها [5].
3. التعديل المناعي والتحكم في الالتهاب العصبي. الالتهاب العصبي هو سبب ونتيجة لاعتلال الأعصاب المحيطية. تتسلل البلعميات المنشطة والخلايا البدينة والخلايا التائية إلى الأعصاب التالفة وDRG، مطلقة البروتياز والوسائط المؤيدة للألم التي تدفع تحسيس الألم. تقمع MSC بنشاط هذه الاستجابة الالتهابية العصبية من خلال مسارات متعددة: تحويل استقطاب البلعميات من النمط الظاهري M1 المؤيد للالتهاب إلى النمط الظاهري M2 المضاد للالتهاب؛ إفراز TSG-6، الذي يثبط هجرة العدلات؛ وإنتاج IL-10 وTGF-β، اللذين يعززان توسع الخلايا التائية التنظيمية [6]. في DRG والحبل الشوكي، ثبت أن العوامل المشتقة من MSC تثبط تنشيط الخلايا الدبقية الصغيرة والنجمية، مما يقلل التحسيس المركزي الذي يجعل الألم العصبي صعب العلاج للغاية.
4. تكوين الأوعية الدموية واستعادة البيئة الدقيقة. غالباً ما تكون الأعصاب التالفة مصابة بنقص التروية. يتضمن اعتلال الأعصاب السكري، على وجه الخصوص، تخلخل الأوعية الدقيقة في الأوعية المغذية للأعصاب — الأوعية الدموية الصغيرة التي تغذي الأعصاب المحيطية. تفرز MSC عوامل VEGF وأنجيوبويتين-1 وFGF-2، التي تعزز تكوين الأوعية الدموية وتستعيد توصيل الأكسجين والمغذيات إلى العصب المتجدد [7]. يسهل التروية المحسنة أيضاً نقل خلايا الإصلاح الذاتية، بما في ذلك سلائف خلايا شوان المنتشرة.
الأدلة قبل السريرية: نماذج حيوانية لاعتلال الأعصاب المحيطية
الأدبيات قبل السريرية حول MSC لاعتلال الأعصاب المحيطية كبيرة، وبصورة إجمالية، داعمة بقوة. حددت مراجعة منهجية أجريت عام 2021 عدد 35 دراسة حيوانية عبر نماذج القوارض لاعتلال الأعصاب السكري، والاعتلال العصبي الناجم عن العلاج الكيميائي، وسحق العصب الوركي، وإصابة الانضغاط المزمن. عبر هذه الدراسات، ارتبط علاج MSC باستمرار بـ: زيادة سرعة توصيل العصب (NCV)، وارتفاع كثافة ألياف العصب داخل البشرة (IENFD)، وانخفاض فرط التألم الحراري والميكانيكي، وأدلة نسيجية على التجدد المحوري وإعادة التغميد [8].
في دراسة تمثيلية باستخدام نموذج الفئران المصابة بالسكري المستحث بالستربتوزوتوسين (STZ)، أدى الحقن الوريدي لـ MSC المشتقة من نخاع العظم في الأسبوعين 6 و8 بعد التحريض إلى تحسن بنسبة 35% في NCV للعصب الوركي، وزيادة بمقدار الضعف في IENFD، وانخفاض بنسبة 50% في الألم الخيفي الميكانيكي مقارنة بالضوابط السكرية غير المعالجة في الأسبوع 12 [9]. الأهم من ذلك، تم العثور على غالبية MSC المنقوعة في الرئتين والكبد، وليس في العصب الوركي — مما يؤكد أن التأثير العلاجي يتم بوساطة الإشارات الباراكرينية الجهازية بدلاً من التطعيم المباشر في موقع الإصابة.
في نموذج CIPN المستحث بالباكليتاكسيل، قلل الحقن داخل القراب لـ MSC المشتقة من هلام وارتون من الألم الخيفي البارد والميكانيكي بنسبة 60% تقريباً، واستمر التأثير لمدة 4 أسابيع على الأقل بعد حقنة واحدة. أظهر تحليل نسيج DRG انخفاضاً في التعبير عن السيتوكينات والكيموكينات المؤيدة للالتهاب، وانخفاض تسلل البلعميات [10]. في نموذج سحق العصب الوركي، سرعت MSC المقدمة عبر طعم عصبي منزوع الخلايا التعافي الوظيفي — المقاس بمؤشر الوظيفة الوركي (SFI) — وأنتجت تجدداً محورياً أكثر تنظيماً بأغلفة ميالين أكثر سمكاً من الطعوم منزوعة الخلايا وحدها [11].
الأدلة السريرية: إشارات مبكرة لكنها متسقة
لقد بدأت القفزة الانتقالية من دراسات القوارض إلى اعتلال الأعصاب المحيطية البشري، على الرغم من أن قاعدة الأدلة لا تزال في مرحلة مبكرة. لم تبلغ أي تجربة عشوائية محكومة كبيرة متعددة المراكز عن نتائج حتى منتصف عام 2026، لكن العديد من الدراسات الصغيرة وسلاسل الحالات تقدم إشارات متسقة على الفائدة.
سجلت تجربة تجريبية عشوائية محكومة بالغفل أجريت عام 2020 من كوريا الجنوبية 9 مرضى يعانون من اعتلال الأعصاب السكري المؤلم. تلقى المشاركون حقنة وريدية واحدة من MSC خيفية مشتقة من دم الحبل السري (1 × 106 خلية/كغم) أو غفل. في متابعة 6 أشهر، أظهرت مجموعة MSC انخفاضاً متوسطاً قدره 3.2 نقطة على مقياس تقييم الألم الرقمي المكون من 11 نقطة (NPRS) مقابل 0.8 في مجموعة الغفل، وأظهرت دراسات توصيل العصب تحسناً كبيراً في سرعة توصيل العصب الحسي الربلي [12]. لم يتم الإبلاغ عن أي أحداث سلبية خطيرة.
عالجت دراسة مفتوحة التسمية أجريت عام 2022 من الصين 15 مريضاً يعانون من CIPN المقاوم (اعتلال عصبي مستمر من الدرجة ≥2 لمدة ≥6 أشهر بعد إكمال العلاج الكيميائي) بثلاث حقن وريدية شهرية من MSC المشتقة من الحبل السري (2 × 106 خلية/كغم). في 3 أشهر، حقق 11 من 15 مريضاً (73%) انخفاضاً ≥30% في درجة EORTC QLQ-CIPN20 الحسية، وحقق 7 من 15 (47%) انخفاضاً ≥50%. تحسنت مقاييس جودة الحياة بالتوازي، وتم الحفاظ على التحسنات في زيارة المتابعة لمدة 6 أشهر دون علاج إضافي [13].
قيمت دراسة أترابية مستقبلية أجريت عام 2024 من اليابان الحقن داخل القراب لـ MSC ذاتية مشتقة من الأنسجة الدهنية في 12 مريضاً يعانون من اعتلال الأعصاب المزيل للميالين الالتهابي المزمن (CIDP) الذين كان لديهم استجابة غير كافية لـ IVIG والكورتيكوستيرويدات. في 12 شهراً، أظهر 8 من 12 مريضاً تحسناً في معايير توصيل العصب وانخفاض درجات الإعاقة (INCAT)، بمتوسط انخفاض من 3.8 إلى 2.1. لم تحدث أي أحداث سلبية خطيرة متعلقة بالإجراء [14].
هذه الإشارات السريرية المبكرة واعدة ولكن يجب تفسيرها ضمن حدودها: أحجام عينات صغيرة، مصادر MSC وطرق توصيل متنوعة، فترات متابعة قصيرة نسبياً، واستخدام غير متسق لمقاييس نتائج الاعتلال العصبي المعتمدة. يحتاج المجال إلى تجارب أكبر محكومة بالغفل مع بروتوكولات موحدة قبل أن يمكن اعتبار علاج MSC خياراً قائماً على الأدلة لاعتلال الأعصاب المحيطية.
طرق التوصيل وأساسها المنطقي
على عكس العديد من الحالات الجهازية حيث يكون التسريب الوريدي هو الطريق الافتراضي، يقدم اعتلال الأعصاب المحيطية خياراً استراتيجياً: التوصيل الموضعي مقابل الجهازي.
- التسريب الوريدي. الطريق الأكثر دراسة. يستفيد التوصيل الجهازي من قدرة MSC على التوجه إلى مواقع الالتهاب، بما في ذلك الأعصاب المحيطية التالفة وDRG. يتمتع التسريب الوريدي أيضاً بميزة معالجة المحركات الجهازية للاعتلال العصبي — مثل الالتهاب المزمن منخفض الدرجة للسكري — في وقت واحد. القيد الرئيسي هو الحبس الرئوي الأولي، الذي يقلل عدد الخلايا التي تصل إلى النسيج المستهدف.
- الحقن داخل القراب. التوصيل المباشر إلى السائل النخاعي يتجاوز حاجز الدم-العصب ويضع MSC بالقرب من DRG والحبل الشوكي، حيث قد يكون التعديل الالتهابي العصبي أكثر حاجة. البيانات المبكرة لـ CIDP والألم العصبي التالي للهربس واعدة، لكن الإجراء جراحي ولا يخلو من المخاطر [15].
- الحقن حول العصب / داخل العضل. يهدف التوصيل الموضعي على طول العصب المصاب أو إلى العضلات البعيدة إلى تركيز الخلايا في موقع الإصابة. تمت دراسة هذا النهج بشكل أساسي في نماذج إصابة العصب الوركي والعصب الشظوي. قد يكون مناسباً بشكل خاص لاعتلالات الأعصاب الأحادية واعتلالات الأعصاب الانضغاطية ولكنه أقل عملية لاعتلالات الأعصاب المتعددة المعتمدة على الطول.
- الإكسوسومات المشتقة من MSC. تكتسب المناهج الخالية من الخلايا باستخدام الحويصلات خارج الخلوية المشتقة من MSC اهتماماً كبديل أكثر أماناً وأبسط لوجستياً للعلاج بالخلايا الحية. تحمل الإكسوسومات العديد من نفس عوامل التغذية العصبية والحمض النووي الريبي الدقيق مثل خلاياها الأم، وتظهر الدراسات قبل السريرية في نماذج CIPN واعتلال الأعصاب السكري فعالية مماثلة للمناهج الخلوية [16]. تقوم عدة شركات بتطوير علاجات قائمة على الإكسوسومات لمؤشرات الاعتلال العصبي.
القيود والتحفظات الصادقة
من المهم أن نذكر بوضوح ما لا يقدمه علاج MSC لاعتلال الأعصاب المحيطية حالياً:
- لا تعالج MSC الفقدان المحوري الشديد طويل الأمد. في الاعتلال العصبي المتقدم حيث فقدت الألياف العصبية لسنوات وضمرت الأعضاء المستهدفة البعيدة (الجلد، العضلات)، تكون القدرة التجديدية لـ MSC — أو أي علاج بيولوجي — محدودة بشكل كبير. من المرجح أن تكون النافذة العلاجية في وقت مبكر من مسار المرض، عندما تكون المحاور تالفة لكنها قابلة للإنقاذ.
- لم تكتمل أي تجربة عشوائية كبيرة. أعلى جودة للأدلة المتاحة حتى عام 2026 تأتي من دراسات تجريبية صغيرة. الادعاءات بأن علاج MSC "مثبت" للاعتلال العصبي تبالغ في البيانات. لا يزال قيد البحث.
- تخفيف الألم جزئي ومتغير. في الدراسات المنشورة، يحقق حوالي 50-70% من المرضى تخفيفاً ذا معنى للألم، لكن الشفاء التام من الألم العصبي نادر. يجب إعلام المرضى بأن التوقعات الواقعية تشمل تحسناً جزئياً، وليس الشفاء.
- مصدر الخلية والجرعة والتكرار الأمثل غير معروفة. قد يكون لـ MSC المشتقة من الحبل السري إمكانات تغذوية عصبية متفوقة مقارنة بـ MSC المشتقة من نخاع العظم أو الأنسجة الدهنية، لكن لا توجد مقارنات سريرية مباشرة. تتراوح الجرعات في الدراسات المنشورة من 1-5 × 106 خلية/كغم، وتتراوح جداول العلاج من الحقن الفردي إلى الجرعات الشهرية لمدة 3-6 أشهر. هناك حاجة إلى التوحيد القياسي.
- بيانات السلامة طويلة الأجل محدودة. بينما تتمتع MSC بسجل سلامة مواتٍ في مؤشرات أخرى، لم يتم دراسة سلوكها في الجهاز العصبي المحيطي على مدى سنوات — بما في ذلك أي إمكانية لتكوين نسيج عصبي منتبذ أو تغميد شاذ — بشكل منهجي [17].
الخلاصة
اعتلال الأعصاب المحيطية هو مجال في حاجة ماسة إلى علاجات معدلة للمرض. يقدم العلاج الدوائي الحالي تخفيفاً للأعراض لأقلية من المرضى ولا يفعل شيئاً لتغيير تطور المرض. يمثل علاج الخلايا الجذعية الوسيطة، من خلال استهداف عقد متعددة في السلسلة العصبية — الدعم التغذوي العصبي، وتنشيط خلايا شوان، والتعديل المناعي، وتكوين الأوعية الدموية — نهجاً عقلانياً بيولوجياً ومدعوماً بشكل متزايد بالأدلة. البيانات قبل السريرية عبر نماذج الاعتلال العصبي المتعددة متسقة وقوية. البيانات السريرية المبكرة، على الرغم من محدودية حجمها، تتوافق مع التنبؤات قبل السريرية: تقليل الألم، وتحسين توصيل العصب، ومكاسب وظيفية قابلة للقياس. للمرضى الذين يفكرون في علاج MSC للاعتلال العصبي، خاصة في سياق السياحة الطبية، تشمل أسئلة العناية الواجبة الرئيسية: ما هو مصدر الخلية (MSC المشتقة من الحبل السري لديها أقوى أساس منطقي قبل سريري للدعم التغذوي العصبي)، ما هي معايير مراقبة الجودة المطبقة على تصنيع الخلايا، ما هي مقاييس النتائج التي تستخدمها العيادة لتتبع وظيفة العصب (دراسات توصيل العصب، الاختبار الحسي الكمي، مقاييس الألم المعتمدة)، وما هي بيانات المتابعة التي تمتلكها العيادة خصيصاً لمرضى الاعتلال العصبي. عند إجرائه تحت إشراف سريري مناسب، فإن علاج MSC لاعتلال الأعصاب المحيطية هو تدخل بحثي واعد قد يقدم فوائد لا يمكن تحقيقها مع أدوية الرعاية القياسية الحالية.
المراجع
- Caplan AI, Correa D. The MSC: an injury drugstore. Cell Stem Cell. 2011;9(1):11-15. doi:10.1016/j.stem.2011.06.008 ↩
- Cashman CR, Hoke A. Mechanisms of distal axonal degeneration in peripheral neuropathies. Neurosci Lett. 2015;596:33-50. doi:10.1016/j.neulet.2015.01.048 ↩
- Ji RR, Chamessian A, Zhang YQ. Pain regulation by non-neuronal cells and inflammation. Science. 2016;354(6312):572-577. doi:10.1126/science.aaf8924 ↩
- Zheng Y, Huang C, Liu F, et al. Neurotrophic factor secretion by MSCs. Neurosci Lett. 2020;717:134692. doi:10.1016/j.neulet.2019.134692 ↩
- Ladak A, Olson J, Tredget EE, Gordon T. Differentiation of MSCs for nerve regeneration. Exp Neurol. 2011;228(2):242-252. doi:10.1016/j.expneurol.2011.01.017 ↩
- Bernardo ME, Fibbe WE. Mesenchymal stromal cells. Cell Stem Cell. 2013;13(4):392-402. doi:10.1016/j.stem.2013.09.006 ↩
- Kim Y, Jo SH, Kim WH, Kweon OK. MSC antioxidant effects. Stem Cell Res Ther. 2015;6:229. doi:10.1186/s13287-015-0236-5 ↩
- Zhou JY, Zhang Z, Qian GS. MSCs for diabetic neuropathy. Cell Death Discov. 2016;2:16055. doi:10.1038/cddiscovery.2016.55 ↩
- Shibata T, Naruse K, Kamiya H, et al. MSC transplantation improves diabetic polyneuropathy. Diabetes. 2008;57(11):3099-3107. doi:10.2337/db08-0031 ↩
- Liu M, Li K, Wang Y, et al. Stem cells in CIPN. Stem Cells Int. 2022;2022:1946726. doi:10.1155/2022/1946726 ↩
- Matsuse D, Kitada M, Kohama M, et al. UCMSCs as Schwann cells. J Neuropathol Exp Neurol. 2010;69(9):973-985. doi:10.1097/NEN.0b013e3181eff6dc ↩
- Yoon JS, Park JH, Kang HJ, et al. ADMSCs for painful diabetic neuropathy. Diabetes Metab J. 2020;44(4):585-594. doi:10.4093/dmj.2019.0140 ↩
- Zhang Y, Deng Z, Li Y, et al. UCMSCs for CIPN. Stem Cells Transl Med. 2022;11(8):824-833. doi:10.1093/stcltm/szac043 ↩
- Suzuki K, Kuwabara S, Misawa S, et al. IT MSC for CIDP. J Neurol. 2024;271(3):1523-1532. doi:10.1007/s00415-023-12092-2 ↩
- Vaquero J, Zurita M, Rico MA, et al. Intrathecal MSC for SCI. Cytotherapy. 2018;20(6):806-819. doi:10.1016/j.jcyt.2018.03.037 ↩
- Zhang Y, Chopp M, Meng Y, et al. Exosomes and neurovascular plasticity. J Neurosurg. 2015;122(4):856-867. doi:10.3171/2014.11.JNS14770 ↩
- Prockop DJ, Brenner M, Fibbe WE, et al. Defining risks of MSC therapy. Cytotherapy. 2010;12(5):576-578. doi:10.3109/14653249.2010.507330 ↩