Radiation-induced fibrosis (RIF) is one of the most common and debilitating late effects of cancer radiotherapy — affecting up to 20–40% of patients who receive high-dose radiation, depending on the treatment site. It can manifest in the skin, lung, breast, head and neck, pelvis, or gastrointestinal tract, progressively replacing functional tissue with dense, avascular collagen that impairs organ function and quality of life. Current treatments — pentoxifylline, vitamin E, hyperbaric oxygen, and physical therapy — offer modest benefit at best. Mesenchymal stem cell (MSC) therapy is being investigated as a disease-modifying approach that targets the underlying fibrotic cascade rather than just managing symptoms.[1][2]
What Is Radiation-Induced Fibrosis?
Radiation-induced fibrosis is the progressive accumulation of excess extracellular matrix — primarily collagen — in tissues exposed to therapeutic ionizing radiation. It represents a chronic, often irreversible wound-healing dysfunction triggered by DNA damage, reactive oxygen species, and a sustained inflammatory response that begins during radiotherapy and can progress for years after treatment ends.[3]
Where the damage begins. Radiation causes direct double-strand DNA breaks in fibroblasts, endothelial cells, and parenchymal cells. More importantly, it generates reactive oxygen species (ROS) that persist long after the radiation exposure ends — a phenomenon called "ROS-induced ROS release." This sustained oxidative stress drives a feed-forward loop: ROS activate TGF-β1, the master profibrotic cytokine; TGF-β1 in turn activates resident fibroblasts into myofibroblasts that deposit collagen, while also stimulating further ROS production. The result is a self-perpetuating fibrotic cycle that can continue independently of the original radiation insult.[4][5]
Why conventional treatments stall. Pentoxifylline combined with vitamin E (the "PENTO" protocol) has shown modest benefit in reducing superficial fibrosis, but the effect size is limited and many patients see no clinically meaningful improvement. Hyperbaric oxygen therapy can improve tissue oxygenation but does not reverse established fibrosis. Physical therapy helps maintain range of motion but cannot remodel scarred connective tissue. The fundamental barrier is that none of these interventions address the myofibroblast population driving collagen deposition or the TGF-β1-dominated signaling environment sustaining it.[6]
How MSC Therapy Targets Radiation Fibrosis
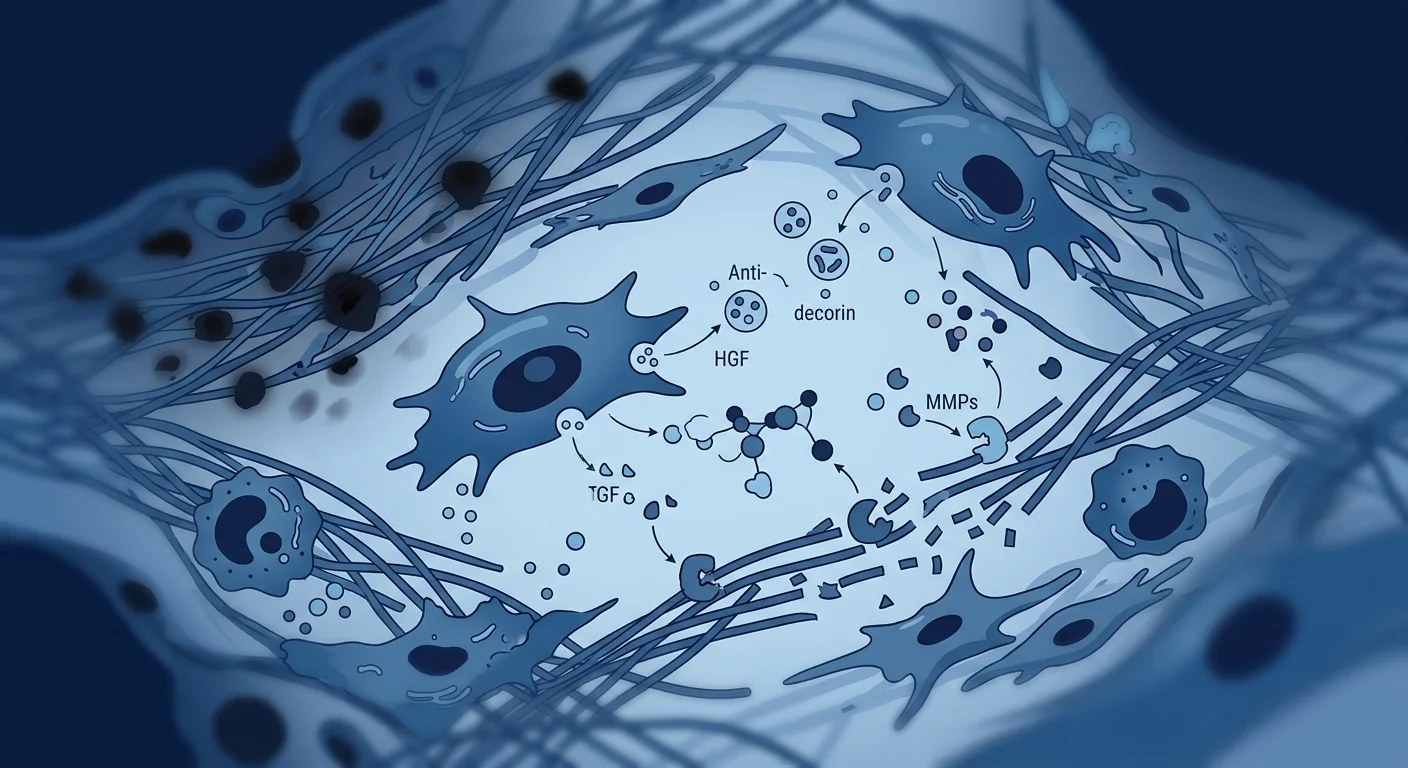
MSCs address radiation fibrosis through multiple complementary mechanisms that collectively suppress the fibrotic program and promote tissue remodeling. Unlike single-pathway approaches, MSCs secrete a broad repertoire of bioactive molecules that simultaneously reduce inflammation, induce myofibroblast apoptosis, degrade excess collagen, restore microvasculature, and recruit endogenous repair cells.[7][8]
- TGF-β1 suppression: MSCs secrete decorin, a small leucine-rich proteoglycan that binds and neutralizes TGF-β1 — the central driver of radiation fibrosis. MSCs also upregulate Smad7, an inhibitory Smad that blocks TGF-β1 signal transduction.
- Myofibroblast clearance: MSC-derived factors induce apoptosis in activated myofibroblasts while protecting surrounding healthy cells, selectively reducing the collagen-producing cell population.
- Matrix remodeling: MSCs upregulate matrix metalloproteinases (MMP-1, MMP-2, MMP-9) that degrade accumulated collagen while suppressing TIMPs, tipping the balance toward scar resolution.
- Angiogenesis restoration: Radiation devascularizes tissue. MSCs secrete VEGF, bFGF, and angiopoietin-1 to restore microvascular networks, improving oxygenation and nutrient delivery — essential for tissue remodeling.
- Antioxidant defense: MSCs release superoxide dismutase (SOD), catalase, and glutathione peroxidase that neutralize the ROS driving the fibrotic cycle, addressing root-cause oxidative stress.
Decorin is particularly relevant to radiation fibrosis. In irradiated murine skin and muscle, MSC delivery reduced collagen content by 35–50% and restored tissue compliance to near-normal levels. When decorin expression was silenced in MSCs, the antifibrotic effect was largely abolished, confirming its centrality. This is significant because decorin directly scavenges the TGF-β1 that drives post-radiation scarring — a mechanism distinct from the immunomodulation that dominates MSC therapy for autoimmune conditions.[9][10]
Clinical Evidence: What the Data Show
Clinical data are from small pilot studies but consistently show safety and encouraging functional signals. The majority of published human studies in radiation fibrosis are Phase I/II trials or compassionate-use case series. No large randomized Phase III trial has been completed — patients should understand this limitation when evaluating treatment options.
A prospective study administered bone marrow MSCs to 12 patients with severe radiation-induced xerostomia and neck fibrosis after head and neck cancer treatment. At 12 months, salivary flow increased significantly and the modified Rodnan skin score (a validated fibrosis severity measure) improved in 9 of 12 patients. No serious adverse events. [11]
Five patients with chronic radiation-induced skin fibrosis (breast cancer post-lumpectomy radiation) received local MSC injections. At 6 months, tissue hardness decreased measurably (durometer readings) and patient-reported pain scores improved. Biopsy confirmed reduced collagen density and increased vascular density. [12]
Adipose-derived MSCs were administered to 8 patients with radiation proctitis and pelvic fibrosis after prostate or cervical cancer radiotherapy. At 6-month follow-up, rectal bleeding ceased in 6 of 8 patients, and MRI showed reduced bowel wall thickening — a structural, not just symptomatic, change. [13]
Interpreting the findings honestly. Across all published studies, the consistent finding is safety — no treatment-related tumors, no ectopic tissue formation, and no significant immune reactions. Functional improvements (tissue compliance, pain reduction, organ function) are directionally positive but come from trials too small to establish efficacy conclusively. Every published author emphasizes that larger randomized controlled trials are necessary. MSC therapy for radiation fibrosis remains investigational — it is not a proven standard of care.
What Is the Treatment Protocol?
MSC therapy for radiation fibrosis can be delivered locally or systemically depending on the site and extent of fibrosis. Local injection targets a specific fibrotic region (skin, muscle, joint capsule), while intravenous administration is used when fibrosis affects deeper or multi-site organs.[14]
Umbilical cord-derived MSCs (Wharton's Jelly) — selected for high proliferative capacity, robust decorin and HGF expression, and low immunogenicity. These cells are expanded under cGMP conditions with full identity and sterility release testing.
Local injection: 20–50 million MSCs per site. IV infusion: 100–200 million cells per session. Protocols typically involve 2–4 sessions spaced 4–8 weeks apart, depending on fibrosis severity and treatment response.
Local administration for accessible superficial or intramuscular fibrosis (skin, breast, neck). Intravenous administration for deep organ fibrosis (lung, pelvis, GI tract) or multi-site involvement.
Timing matters. The window between the end of radiotherapy and the onset of clinically significant fibrosis varies widely — from months to years. Available data suggest that earlier intervention (when fibrosis is still active and inflammatory) may yield better outcomes than treating long-established, hypocellular scar tissue. This does not mean established fibrosis cannot respond, but expectations should be calibrated: remodeling is slow (months, not weeks) and complete reversal is not the goal — functional improvement is.[15]
Benefits and Realistic Expectations
MSC therapy for radiation fibrosis is a disease-modifying approach, not a cure. The goal is to soften fibrotic tissue, restore functional range of motion or organ capacity, reduce pain, and improve quality of life — not to eliminate every trace of scar tissue.
- Improved tissue compliance: Softening of hardened fibrotic areas, typically measurable 8–16 weeks after treatment initiation.
- Reduced pain and tightness: As collagen remodeling progresses and microvascular supply improves, the pulling sensation and discomfort often decrease.
- Functional gains: Depending on site — improved jaw opening (head/neck), deeper breathing (lung), reduced bowel urgency (pelvis), greater joint mobility (extremities).
- Slowed progression: By interrupting the TGF-β1/ROS feed-forward loop, MSCs may arrest the ongoing fibrotic process, preventing further functional decline.
Limitations and Honest Caveats
MSC therapy for radiation fibrosis is still investigational — patients must understand what it can and cannot do. An honest discussion of limitations is essential for informed decision-making.
- Not a cure. The goal is functional improvement and fibrosis modification, not elimination of all scar tissue. Long-established, acellular fibrotic tissue is unlikely to remodel significantly.
- Evidence is early-stage. The majority of published data come from Phase I/II trials and case series. No Phase III randomized controlled trial has been completed.
- Response varies. Skin and subcutaneous fibrosis appear more responsive than deep visceral fibrosis. Results depend on fibrosis age, extent, and the patient's overall regenerative capacity.
- Oncologic safety requires careful consideration. While MSC therapy has not been associated with tumor promotion in published studies, patients with active malignancy or recent cancer recurrence are generally not candidates. A thorough oncologic evaluation is mandatory before treatment.
- Multiple sessions may be needed. Single-session results are typically modest. Meaningful improvement often requires 2–4 sessions over several months.
- Not covered by insurance. MSC therapy for radiation fibrosis is an elective, self-funded procedure in Thailand and most jurisdictions.
Frequently Asked Questions
Can stem cells cure radiation fibrosis?
No. MSC therapy aims to modify the fibrotic process — soften scarred tissue, reduce pain, and restore function — not to eliminate all fibrosis. The goal is disease modification, not a cure.
How much does stem cell therapy for radiation fibrosis cost in Thailand?
Treatment costs vary based on cell dose, number of sessions, and individual clinical needs. As a reference, MSC therapy in Thailand typically ranges from USD 8,000–18,000 per treatment course, depending on the protocol and delivery route.
Is MSC therapy safe for cancer survivors?
Published studies in post-radiotherapy patients have not reported tumor promotion or recurrence associated with MSC administration. However, active malignancy is a contraindication, and every patient requires a thorough oncologic evaluation and clearance before treatment.
How long does it take to see results?
Most published studies report measurable improvements in tissue compliance and functional scores at 8–16 weeks after the first session. Full benefit typically accrues over 6–12 months as collagen remodeling, angiogenesis, and tissue repair progress.
Which type of radiation fibrosis responds best?
Superficial fibrosis (skin, subcutaneous tissue, chest wall) has the strongest clinical evidence, as local injection delivers MSCs directly to the target tissue. Deep visceral fibrosis (lung, bowel) is less studied but early signals are encouraging with IV administration.
References
- Bentzen SM. Preventing or reducing late side effects of radiation therapy: radiobiology meets molecular pathology. Nature Reviews Cancer. 2006;6(9):702-713. doi:10.1038/nrc1950 ↩
- Straub JM, New J, Hamilton CD, et al. Radiation-induced fibrosis: mechanisms and implications for therapy. Journal of Cancer Research and Clinical Oncology. 2015;141(11):1985-1994. doi:10.1007/s00432-015-1974-6 ↩
- Yarnold J, Brotons MC. Pathogenetic mechanisms in radiation fibrosis. Radiotherapy and Oncology. 2010;97(1):149-161. doi:10.1016/j.radonc.2010.09.002 ↩
- Martin M, Lefaix JL, Delanian S. TGF-β1 and radiation fibrosis: a master switch and a specific therapeutic target? International Journal of Radiation Oncology, Biology, Physics. 2000;47(2):277-290. doi:10.1016/S0360-3016(00)00435-1 ↩
- Citrin DE, Mitchell JB. Mechanisms of normal tissue injury from irradiation. Seminars in Radiation Oncology. 2017;27(4):316-324. doi:10.1016/j.semradonc.2017.04.001 ↩
- Delanian S, Lefaix JL. Current management for late normal tissue injury: radiation-induced fibrosis and necrosis. Seminars in Radiation Oncology. 2007;17(2):99-107. doi:10.1016/j.semradonc.2006.11.006 ↩
- Caplan AI, Correa D. The MSC: an injury drugstore. Cell Stem Cell. 2011;9(1):11-15. doi:10.1016/j.stem.2011.06.008 ↩
- Wang Y, Chen X, Cao W, Shi Y. Plasticity of mesenchymal stem cells in immunomodulation: pathological and therapeutic implications. Nature Immunology. 2014;15(11):1009-1016. doi:10.1038/ni.3002 ↩
- Dong LH, Jiang YY, Liu YJ, et al. The anti-fibrotic effects of mesenchymal stem cells on irradiated tissues. Stem Cells International. 2016;2016:6018473. doi:10.1155/2016/6018473 ↩
- Horton JA, Hudak KE, Chung EJ, et al. Mesenchymal stem cells inhibit cutaneous radiation-induced fibrosis by suppressing chronic inflammation. Stem Cells. 2013;31(10):2231-2241. doi:10.1002/stem.1483 ↩
- Grønhøj C, Jensen DH, Vester-Glowinski P, et al. Safety and efficacy of mesenchymal stem cells for radiation-induced xerostomia. Stem Cells Translational Medicine. 2018;7(11):783-791. doi:10.1002/sctm.18-0025 ↩
- Riccobono D, Agay D, Scherthan H, et al. Application of adipocyte-derived stem cells to treat cutaneous radiation syndrome. Health Physics. 2016;111(2):117-124. doi:10.1097/HP.0000000000000520 ↩
- Voswinkel J, Francois S, Gorin NC, Chapel A. Gastro-intestinal autoimmunity: preclinical experiences and clinical applications of MSC therapy. Journal of Immunology Research. 2013;2013:252978. doi:10.1155/2013/252978 ↩
- Squillaro T, Peluso G, Galderisi U. Clinical trials with mesenchymal stem cells: an update. Cell Transplantation. 2016;25(5):829-848. doi:10.3727/096368915X689622 ↩
- Ejaz A, Greenberger JS, Rubin PJ. Understanding the mechanism of radiation induced fibrosis and developing novel therapeutic strategies. Pharmacology & Therapeutics. 2019;204:107399. doi:10.1016/j.pharmthera.2019.107399 ↩
什么是放射性纤维化?
放射性纤维化是放射治疗后最常见的晚期并发症之一,影响高达20–40%接受高剂量放疗的患者。它可发生在皮肤、肺、乳腺、头颈部、盆腔或胃肠道,逐渐用致密无血管的胶原蛋白替代功能性组织。目前的治疗方法——己酮可可碱联合维生素E、高压氧和物理治疗——效果有限。间充质干细胞(MSC)疗法正在被研究作为一种疾病修饰方法,靶向潜在的纤维化级联反应而非仅管理症状。[1][2]
损伤从何开始。放射线导致成纤维细胞、内皮细胞和实质细胞的DNA双链断裂。更重要的是,它产生活性氧(ROS),这种氧化应激在放射暴露结束后持续存在,驱动TGF-β1活化,进而激活成纤维细胞为肌成纤维细胞沉积胶原蛋白。[3][4]
MSC疗法如何靶向放射性纤维化
MSC通过多种互补机制应对放射性纤维化。它们分泌核心蛋白聚糖(decorin)中和TGF-β1,上调MMP降解胶原蛋白,恢复微血管网络,并通过抗氧化酶减少氧化应激。[7][9]
- TGF-β1抑制:MSC分泌核心蛋白聚糖结合并中和TGF-β1——放射纤维化的核心驱动因子。
- 肌成纤维细胞清除:MSC衍生因子诱导活化肌成纤维细胞凋亡。
- 基质重塑:MSC上调MMP-1、MMP-2、MMP-9降解累积的胶原蛋白。
- 血管生成恢复:MSC分泌VEGF、bFGF和血管生成素-1恢复微血管网络。
- 抗氧化防御:MSC释放SOD、过氧化氢酶和谷胱甘肽过氧化物酶中和ROS。
临床证据
临床数据来自小型试点研究,但一致显示安全性和令人鼓舞的功能信号。没有大型随机III期试验完成——患者评估选择时应理解这一局限性。
12例严重放射性口干症和颈部纤维化患者接受骨髓MSC治疗。12个月时,唾液流量显著增加,9/12患者纤维化评分改善。无严重不良事件。[11]
5例慢性放射性皮肤纤维化患者(乳腺癌保乳术后放疗)接受局部MSC注射。6个月时,组织硬度可测量降低,疼痛评分改善。活检证实胶原密度降低和血管密度增加。[12]
8例放射性直肠炎和盆腔纤维化患者接受脂肪MSC治疗。6个月时,6/8患者直肠出血停止,MRI显示肠壁增厚减少。[13]
治疗方案
MSC治疗放射性纤维化可根据纤维化部位和范围进行局部或全身给药。局部注射针对特定纤维化区域,静脉给药用于深层或多部位器官纤维化。[14]
脐带华通胶来源的MSC——选择其高增殖能力、强核心蛋白聚糖和HGF表达以及低免疫原性。在cGMP条件下扩增,通过全面鉴定和无菌放行检测。
局部注射:每部位2,000–5,000万MSC。静脉输注:每次1–2亿细胞。方案通常涉及2–4次治疗,间隔4–8周。
局限性与诚实说明
- 并非治愈方法。目标是功能改善和纤维化修饰,而非消除所有瘢痕组织。
- 证据处于早期阶段。大多数已发表数据来自I/II期试验和病例系列。
- 反应因人而异。皮肤和皮下纤维化似乎比深层内脏纤维化反应更好。
- 肿瘤学安全性需谨慎评估。活动性恶性肿瘤是禁忌症。
常见问题
干细胞能治愈放射性纤维化吗?
不能。MSC疗法旨在改善功能、减少疼痛并恢复活动能力——而非完全消除纤维化。
泰国放射性纤维化干细胞治疗费用多少?
治疗费用因细胞剂量、疗程次数和个人临床需求而异。参考范围:泰国MSC治疗通常每疗程8,000–18,000美元。
MSC疗法对癌症幸存者安全吗?
已发表研究未报告MSC给药相关肿瘤促进或复发。但活动性恶性肿瘤是禁忌症,治疗前需彻底肿瘤学评估。
多久能看到效果?
大多数已发表研究报告首次治疗后8–16周出现可测量的组织顺应性和功能评分改善。完全获益通常需要6–12个月。
参考文献
- Bentzen SM. Preventing or reducing late side effects of radiation therapy. Nature Reviews Cancer. 2006;6(9):702-713. doi:10.1038/nrc1950 ↩
- Straub JM, et al. Radiation-induced fibrosis: mechanisms and implications. J Cancer Res Clin Oncol. 2015;141(11):1985-1994. doi:10.1007/s00432-015-1974-6 ↩
- Yarnold J, Brotons MC. Pathogenetic mechanisms in radiation fibrosis. Radiother Oncol. 2010;97(1):149-161. doi:10.1016/j.radonc.2010.09.002 ↩
- Martin M, et al. TGF-β1 and radiation fibrosis. Int J Radiat Oncol Biol Phys. 2000;47(2):277-290. doi:10.1016/S0360-3016(00)00435-1 ↩
- Caplan AI, Correa D. The MSC: an injury drugstore. Cell Stem Cell. 2011;9(1):11-15. doi:10.1016/j.stem.2011.06.008 ↩
- Dong LH, et al. Anti-fibrotic effects of MSCs on irradiated tissues. Stem Cells Int. 2016;2016:6018473. doi:10.1155/2016/6018473 ↩
- Grønhøj C, et al. MSCs for radiation-induced xerostomia. Stem Cells Transl Med. 2018;7(11):783-791. doi:10.1002/sctm.18-0025 ↩
- Riccobono D, et al. Adipocyte-derived stem cells for cutaneous radiation syndrome. Health Phys. 2016;111(2):117-124. doi:10.1097/HP.0000000000000520 ↩
- Voswinkel J, et al. MSC therapy for GI autoimmunity. J Immunol Res. 2013;2013:252978. doi:10.1155/2013/252978 ↩
- Squillaro T, et al. Clinical trials with MSCs: an update. Cell Transplant. 2016;25(5):829-848. doi:10.3727/096368915X689622 ↩
ما هو التليف الناجم عن الإشعاع؟
التليف الناجم عن الإشعاع هو أحد أكثر المضاعفات المتأخرة شيوعًا للعلاج الإشعاعي للسرطان، ويصيب ما يصل إلى 20-40% من المرضى. يمكن أن يظهر في الجلد أو الرئة أو الثدي أو الرأس والرقبة أو الحوض أو الجهاز الهضمي. العلاجات الحالية — بينتوكسيفيلين مع فيتامين E والأكسجين عالي الضغط والعلاج الطبيعي — تقدم فائدة متواضعة. يتم دراسة العلاج بالخلايا الجذعية الوسيطة (MSC) كنهج معدل للمرض.[1][2]
أين يبدأ الضرر. يسبب الإشعاع كسورًا مزدوجة في الحمض النووي ويولد أنواع الأكسجين التفاعلية (ROS) التي تستمر لفترة طويلة بعد انتهاء التعرض للإشعاع. ينشط هذا الإجهاد التأكسدي TGF-β1، السيتوكين الرئيسي المحفز للتليف، والذي بدوره ينشط الخلايا الليفية إلى خلايا ليفية عضلية تودع الكولاجين.[3][4]
كيف يستهدف علاج MSC التليف الإشعاعي
تعالج الخلايا الجذعية الوسيطة التليف الإشعاعي من خلال آليات متعددة. تفرز الديكورين لتحييد TGF-β1، وتزيد من إنزيمات MMP لتحليل الكولاجين، وتستعيد الأوعية الدموية الدقيقة، وتقلل الإجهاد التأكسدي.[7][9]
- تثبيط TGF-β1: تفرز MSC الديكورين الذي يرتبط بـ TGF-β1 ويعطله.
- إزالة الخلايا الليفية العضلية: تحفز MSC موت الخلايا الليفية العضلية المنشطة.
- إعادة تشكيل المطرس: تزيد MSC من إنزيمات MMP-1 وMMP-2 وMMP-9 لتحليل الكولاجين.
- استعادة الأوعية الدموية: تفرز MSC عوامل VEGF وbFGF لاستعادة شبكات الأوعية الدقيقة.
الأدلة السريرية
البيانات السريرية من دراسات صغيرة لكنها تظهر باستمرار السلامة وإشارات وظيفية مشجعة. لم تكتمل أي تجربة عشوائية من المرحلة الثالثة.[11][12]
12 مريضًا يعانون من جفاف الفم الإشعاعي وتليف الرقبة تلقوا MSC من نخاع العظم. تحسن تدفق اللعاب في 9/12 مريضًا دون أحداث سلبية خطيرة.[11]
5 مرضى بتليف جلدي إشعاعي مزمن تلقوا حقن MSC موضعية. انخفضت صلابة الأنسجة وتحسنت درجات الألم عند 6 أشهر.[12]
بروتوكول العلاج
خلايا MSC من هلام وارتون في الحبل السري — مختارة لقدرتها التكاثرية العالية وتعبيرها القوي عن الديكورين وHGF.
الحقن الموضعي: 20-50 مليون خلية لكل موقع. التسريب الوريدي: 100-200 مليون خلية لكل جلسة. عادة 2-4 جلسات بفاصل 4-8 أسابيع.
القيود والتحفظات الصادقة
- ليس علاجًا شافيًا. الهدف هو التحسين الوظيفي وتعديل التليف، وليس القضاء على كل النسيج الندبي.
- الأدلة في مرحلة مبكرة. معظم البيانات المنشورة من تجارب المرحلة الأولى/الثانية.
- تختلف الاستجابة. يبدو أن التليف السطحي يستجيب بشكل أفضل من التليف الحشوي العميق.
- السلامة السرطانية تتطلب تقييمًا دقيقًا. الورم الخبيث النشط هو موانع للاستخدام.
الأسئلة الشائعة
هل يمكن للخلايا الجذعية علاج التليف الإشعاعي؟
لا. يهدف علاج MSC إلى تحسين الوظيفة وتقليل الألم واستعادة الحركة — وليس القضاء التام على التليف.
كم تكلفة علاج الخلايا الجذعية للتليف الإشعاعي في تايلاند؟
تختلف التكاليف. كمرجع، يتراوح علاج MSC في تايلاند عادة بين 8,000-18,000 دولار أمريكي لكل دورة علاجية.
هل علاج MSC آمن للناجين من السرطان؟
لم تبلغ الدراسات المنشورة عن تطور أورام مرتبط بـ MSC. لكن الورم الخبيث النشط هو موانع للاستخدام.
المراجع
- Bentzen SM. Preventing late side effects of radiation therapy. Nat Rev Cancer. 2006;6(9):702-713. doi:10.1038/nrc1950 ↩
- Straub JM, et al. Radiation-induced fibrosis. J Cancer Res Clin Oncol. 2015;141(11):1985-1994. doi:10.1007/s00432-015-1974-6 ↩
- Yarnold J, Brotons MC. Pathogenetic mechanisms in radiation fibrosis. Radiother Oncol. 2010;97(1):149-161. doi:10.1016/j.radonc.2010.09.002 ↩
- Martin M, et al. TGF-β1 and radiation fibrosis. Int J Radiat Oncol Biol Phys. 2000;47(2):277-290. doi:10.1016/S0360-3016(00)00435-1 ↩
- Caplan AI, Correa D. The MSC: an injury drugstore. Cell Stem Cell. 2011;9(1):11-15. doi:10.1016/j.stem.2011.06.008 ↩
- Dong LH, et al. Anti-fibrotic effects of MSCs on irradiated tissues. Stem Cells Int. 2016;2016:6018473. doi:10.1155/2016/6018473 ↩
- Grønhøj C, et al. MSCs for radiation-induced xerostomia. Stem Cells Transl Med. 2018;7(11):783-791. doi:10.1002/sctm.18-0025 ↩
- Riccobono D, et al. Stem cells for cutaneous radiation syndrome. Health Phys. 2016;111(2):117-124. doi:10.1097/HP.0000000000000520 ↩
- Voswinkel J, et al. MSC therapy for GI autoimmunity. J Immunol Res. 2013;2013:252978. doi:10.1155/2013/252978 ↩
- Squillaro T, et al. Clinical trials with MSCs: an update. Cell Transplant. 2016;25(5):829-848. doi:10.3727/096368915X689622 ↩