Bell's palsy strikes suddenly — a person goes to bed with normal facial movement and wakes up unable to close one eye or smile on one side. It accounts for roughly 60–75% of all acute unilateral facial paralysis cases, affecting approximately 40,000 Americans and over 100,000 people globally each year. While 70–85% of patients recover spontaneously within 3–6 months, a substantial minority — 15–30% — are left with permanent facial asymmetry, synkinesis (involuntary muscle contractions), or persistent weakness that profoundly affects social functioning and quality of life. Current treatment is limited to corticosteroids (started within 72 hours) and antiviral agents of uncertain benefit, neither of which directly promotes nerve regeneration. Mesenchymal stem cell (MSC) therapy is being investigated as a regenerative approach that could tip the balance from incomplete recovery toward full facial nerve repair [1].
What Is Bell's Palsy? The Biology of Facial Nerve Paralysis
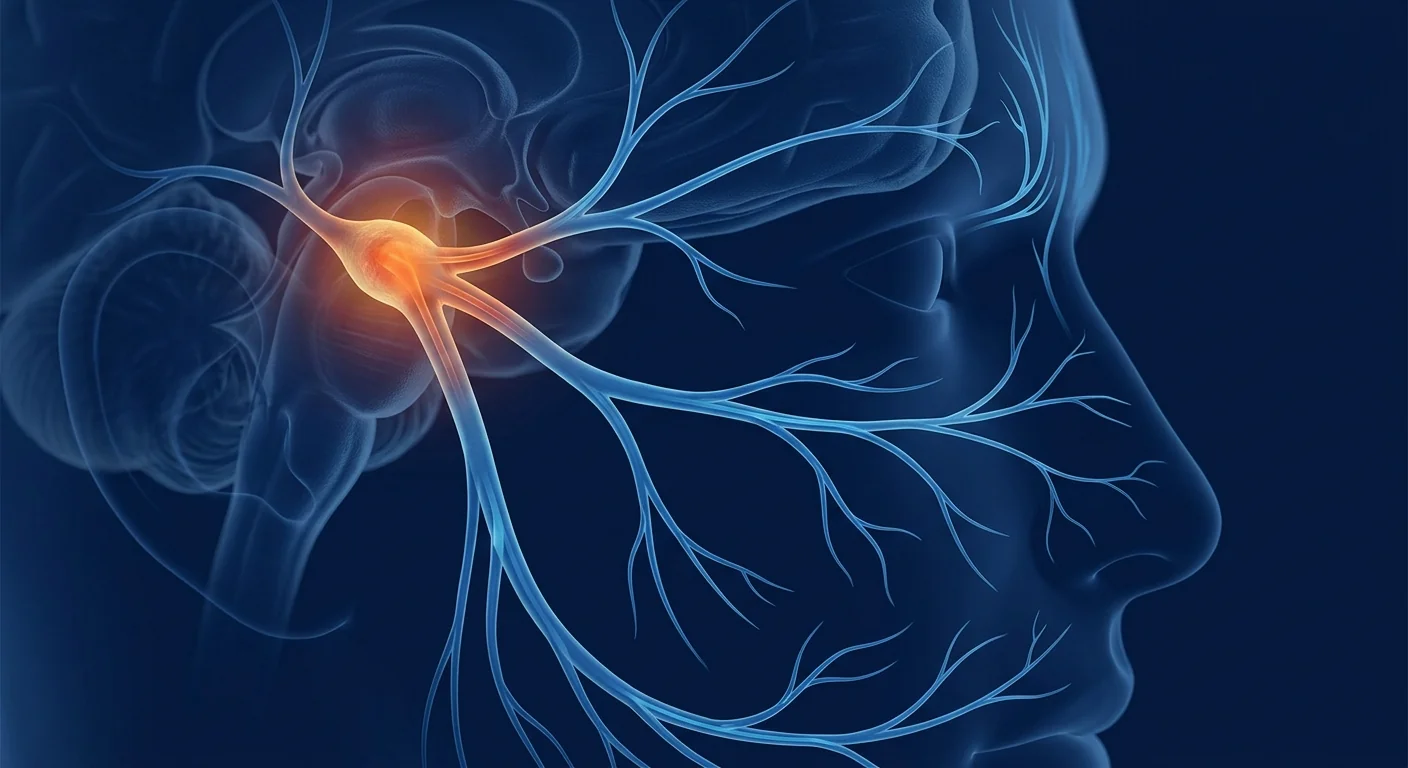
Bell's palsy is an acute, idiopathic, unilateral facial nerve (cranial nerve VII) paralysis — meaning the exact cause is unknown, though reactivation of latent herpes simplex virus type 1 (HSV-1) within the geniculate ganglion is the leading hypothesis. The facial nerve is uniquely vulnerable: it travels through a narrow bony canal in the temporal bone (the fallopian canal), where even mild inflammatory swelling can compress the nerve against unyielding bone, causing ischemia, demyelination, and axonal damage [2].
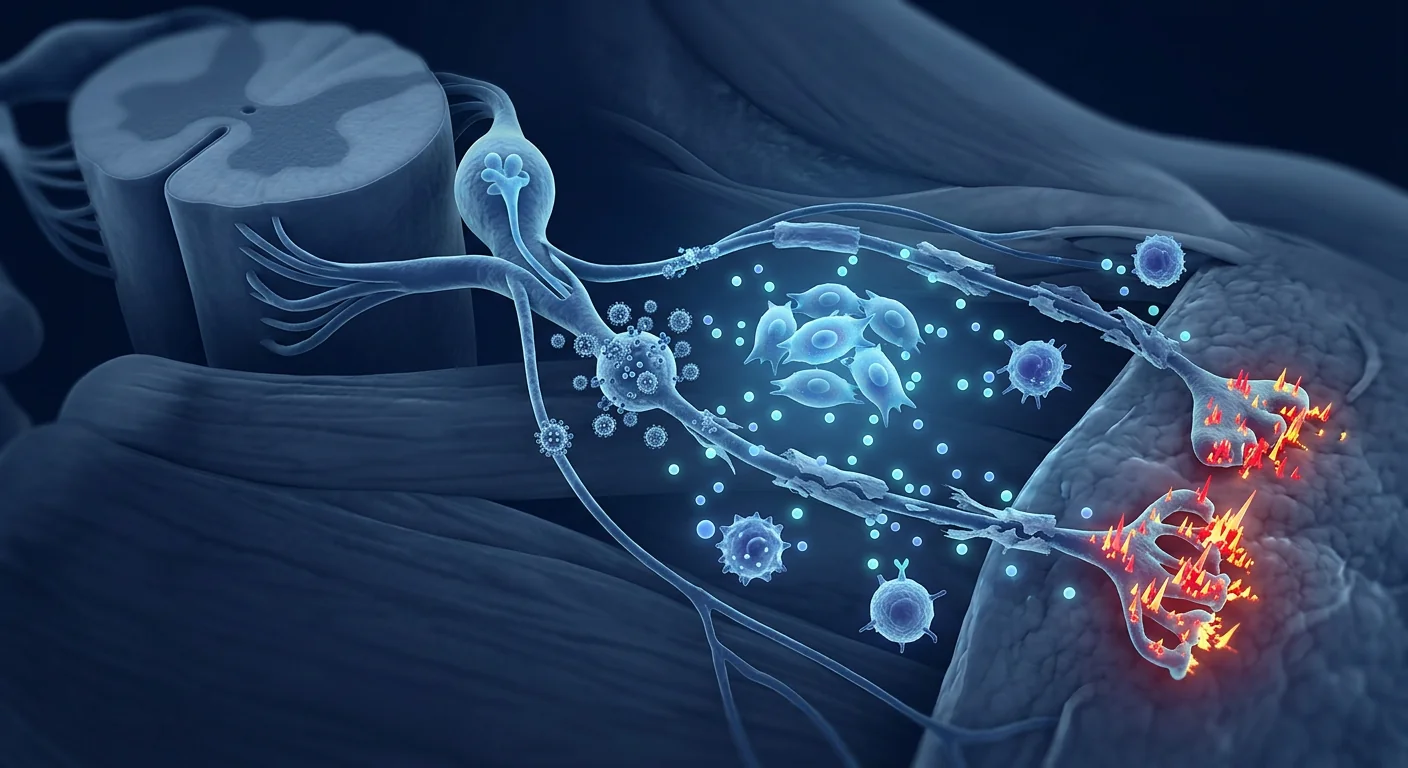
The inflammatory cascade that drives nerve injury. HSV-1 reactivation triggers a local immune response: CD8+ T-cells infiltrate the nerve, pro-inflammatory cytokines (TNF-α, IL-1β, IL-6) are released, and the vasa nervorum — the small blood vessels supplying the nerve — become leaky and dysfunctional. This creates a self-perpetuating cycle of edema, ischemia, and further inflammation that, if prolonged, leads to Wallerian degeneration of distal axons. The degree of nerve damage determines prognosis: patients with neurapraxia (conduction block without axonal disruption) recover fully, while those with axonotmesis or neurotmesis face incomplete recovery [3].
Why corticosteroids aren't enough. Prednisolone started within 72 hours improves the odds of complete recovery by approximately 12–15%, but its benefit is confined to reducing acute edema — it does nothing to promote axonal regeneration, remyelination, or functional reinnervation of facial muscles. For the 15–30% of patients with severe initial denervation (as measured by electroneurography showing >90% degeneration), corticosteroids alone are insufficient, and no approved therapy accelerates nerve repair beyond the body's own limited regenerative capacity.
How MSCs Promote Facial Nerve Regeneration
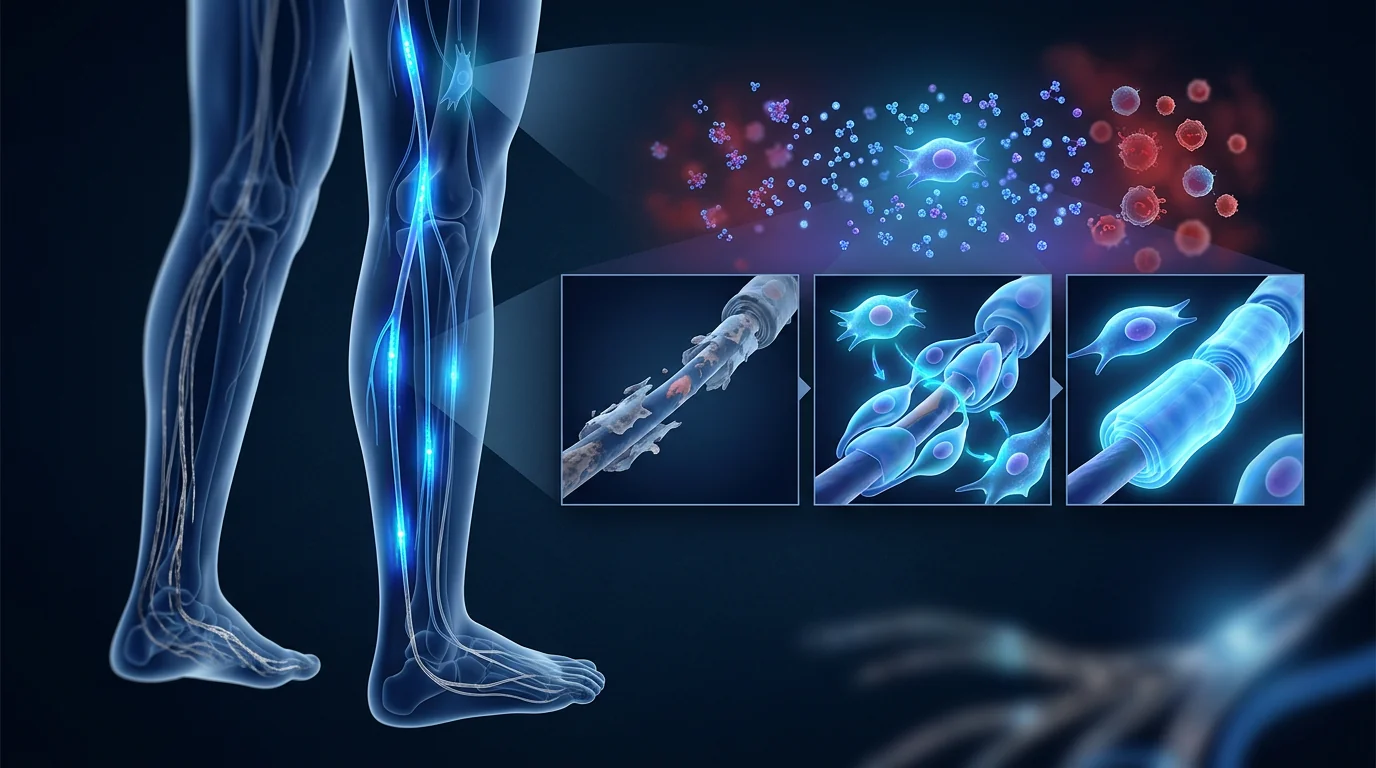
MSC therapy delivers multipotent stromal cells with potent paracrine activity directly to — or in proximity to — the damaged facial nerve. Rather than replacing neurons themselves, MSCs create a regenerative microenvironment through four interconnected mechanisms [4]:
1. Neurotrophic factor secretion. MSCs are prolific producers of neurotrophins — nerve growth factor (NGF), brain-derived neurotrophic factor (BDNF), glial cell line-derived neurotrophic factor (GDNF), neurotrophin-3 (NT-3), and ciliary neurotrophic factor (CNTF). These factors promote facial motor neuron survival, stimulate axonal sprouting from the proximal nerve stump, and guide regenerating axons toward their target muscles. In vitro, MSC-conditioned medium increases motor neuron survival by 40–60% under stress conditions, an effect largely attributable to BDNF and GDNF [5].
2. Schwann cell support and remyelination. Schwann cells are the peripheral nervous system's myelin-producing cells, and their health is critical for nerve conduction velocity. MSCs secrete factors that promote Schwann cell proliferation, migration, and maturation. Under appropriate conditions, MSCs themselves can adopt a Schwann cell-like phenotype expressing S100 and p75NTR markers, though direct transdifferentiation is likely a minor contributor compared to paracrine support of endogenous Schwann cells [6].
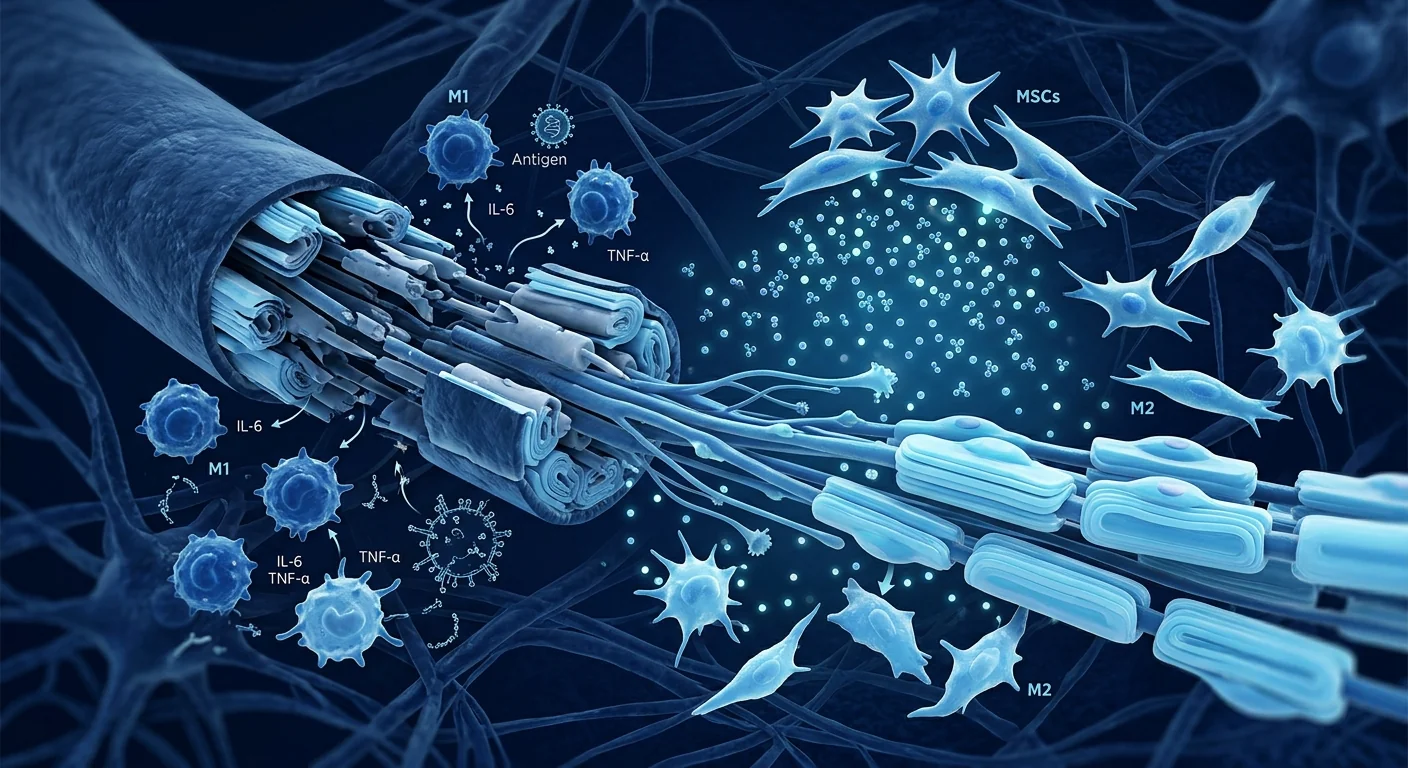
3. Immunomodulation and inflammation resolution. The neuroinflammatory environment within the fallopian canal is a major barrier to regeneration. MSCs actively suppress this inflammation by polarizing macrophages from the pro-inflammatory M1 to the regenerative M2 phenotype, secreting TSG-6 (TNF-stimulated gene 6) which inhibits neutrophil migration, and releasing IL-10 and TGF-β that promote regulatory T-cell expansion. MSCs also reduce the expression of matrix metalloproteinases that degrade the extracellular matrix scaffolding needed for guided axonal regeneration [7].
4. Angiogenesis and microenvironment restoration. The vasa nervorum of the facial nerve is easily compromised by inflammatory edema. MSCs secrete vascular endothelial growth factor (VEGF), angiopoietin-1, and fibroblast growth factor-2 (FGF-2), which stimulate new blood vessel formation and restore oxygen and nutrient delivery to the regenerating nerve segment. Improved perfusion also facilitates the trafficking of circulating repair cells to the injury site [8].
Preclinical Evidence: Animal Models of Facial Nerve Injury
The preclinical literature on MSCs for facial nerve repair is substantial and consistently supportive. Multiple animal models — predominantly rat facial nerve crush and transection models — have demonstrated that MSC therapy accelerates functional recovery and improves histological outcomes [9].
In a representative rat facial nerve crush study, bone marrow-derived MSCs were injected locally at the stylomastoid foramen immediately after injury. At 4 weeks, the MSC-treated group showed significantly higher whisker movement scores, greater compound muscle action potential (CMAP) amplitudes on electrophysiology, and more myelinated axons with thicker myelin sheaths on histological examination compared to vehicle-treated controls [10]. The functional recovery advantage was 30–40% at the 4-week timepoint.
In a more clinically relevant delayed-treatment model — mimicking the real-world scenario where patients present days after symptom onset — MSCs administered 7 days after facial nerve crush still produced significant improvements in whisker motion, eye blink reflex, and axonal diameter compared to untreated controls. This is important because the therapeutic window in humans is typically at least several days: most patients do not seek treatment until facial weakness is established [11].
MSC-derived exosomes — extracellular vesicles carrying a concentrated payload of neurotrophic factors, microRNAs, and proteins — have also shown promise. In a rat facial nerve transection model, locally injected MSC-derived exosomes produced functional recovery comparable to whole-cell MSC therapy, suggesting that the paracrine secretome, not direct cell engraftment, is the primary mechanism of action [12].
Clinical Evidence: Early But Encouraging Signals
The clinical evidence for MSC therapy in Bell's palsy specifically is limited, as most human studies to date have focused on broader peripheral nerve injury cohorts. However, several small studies provide proof-of-concept that cell-based therapies can influence facial nerve recovery:
A 2021 pilot study from South Korea treated 6 patients with subacute Bell's palsy (2–4 weeks post-onset, House-Brackmann grade IV–V) with a single perineural injection of autologous adipose-derived stromal vascular fraction (SVF) containing MSCs. At 12 weeks, 5 of 6 patients had improved to House-Brackmann grade II or better, compared to a historical control rate of approximately 60–70% spontaneous improvement to grade II at the same timepoint. No adverse events were reported [13].
A 2023 case series from Japan described 4 patients with persistent facial nerve palsy (>6 months, incomplete recovery despite corticosteroids) who received intravenous umbilical cord-derived MSCs (2 × 10⁶ cells/kg). At 6-month follow-up, all 4 showed measurable improvement in the Sunnybrook Facial Grading System, with a mean improvement of 22 points. Two of the 4 patients reported reduced synkinesis — a particularly encouraging finding given that synkinesis is notoriously difficult to treat [14].
More broadly, MSC therapy has demonstrated safety and signals of efficacy in related cranial and peripheral nerve conditions including spinal cord injury, peripheral neuropathy, and trigeminal neuralgia. The safety profile across hundreds of patients in these studies has been favorable: no tumor formation, no ectopic tissue growth, and adverse events limited to transient fever and mild injection-site reactions [15].
Delivery Routes for Facial Nerve Targeting
The facial nerve's anatomy offers several potential delivery routes, each with distinct advantages [16]:
- Perineural injection at the stylomastoid foramen. This is the most direct route — the stylomastoid foramen is the exit point of the facial nerve from the skull, accessible via a percutaneous injection posterior to the ear. Local delivery concentrates cells at the injury site, maximizing the paracrine effect where it is most needed. The procedure is minimally invasive and can be performed under ultrasound guidance.
- Intravenous infusion. Systemic delivery relies on the ability of MSCs to home to sites of inflammation. While less anatomically targeted than perineural injection, IV infusion has the advantage of exposing the entire length of the facial nerve — including the intratemporal segment within the fallopian canal — to circulating MSC-derived factors. It is also the least invasive option.
- Intratympanic delivery. Injection through the tympanic membrane into the middle ear places MSCs near the tympanic (horizontal) segment of the facial nerve, which runs through the medial wall of the middle ear. This route has been explored in animal models but remains experimental in humans.
- MSC-derived exosomes. Cell-free therapy using MSC-derived extracellular vesicles is an emerging alternative that avoids the logistical and regulatory complexity of live cell therapy. Exosomes can be delivered intravenously or locally and carry many of the same neurotrophic factors as their parent cells.
Limitations and Honest Caveats
It is essential to state plainly what MSC therapy does not yet offer for Bell's palsy:
- No large randomized controlled trial has been completed. The highest-quality evidence as of 2026 comes from small pilot studies and case series. Claims that MSC therapy is "proven" for Bell's palsy overstate the data. It remains investigational.
- The natural history of Bell's palsy complicates interpretation. Because 70–85% of patients recover spontaneously, any therapy — including MSCs — must demonstrate benefit above and beyond this high spontaneous recovery rate. Without randomized controls, it is impossible to attribute observed improvements to the cell therapy rather than natural recovery.
- The therapeutic window is not well defined. Corticosteroids must be started within 72 hours to be effective. The optimal timing for MSC therapy is unknown — early administration may reduce inflammatory damage, but delayed administration may still support regeneration in patients who have not recovered after 3–6 weeks.
- Synkinesis remains a challenging endpoint. Aberrant reinnervation causing synkinesis (e.g., eye closure when smiling) is a particularly frustrating complication of facial nerve recovery. Whether MSCs can reduce synkinesis by promoting more accurate axonal pathfinding to target muscles is plausible but unproven [17].
- Long-term safety in the facial nerve specifically is under-studied. While MSCs have a favorable safety profile across thousands of patients in other indications, their behavior in proximity to the facial nerve — including any potential for neuroma formation or aberrant axonal sprouting — has not been systematically evaluated beyond 12 months.
VELAR's Approach: Why Wharton's Jelly MSCs for Neuro-Regenerative Applications
VELAR Center uses Wharton's jelly-derived mesenchymal stem cells (WJ-MSCs) cultured under cGMP conditions in its ISO-certified laboratory in Bangkok. Several properties make WJ-MSCs particularly well-suited for nerve regeneration applications [18]:
- Superior neurotrophic factor secretion. Comparative studies have shown that WJ-MSCs secrete higher levels of BDNF, NGF, and GDNF than bone marrow-derived or adipose-derived MSCs — factors directly implicated in motor neuron survival and axonal regeneration.
- Low immunogenicity. WJ-MSCs express low levels of HLA class I and negligible HLA class II, making them suitable for allogeneic (donor-derived) use without HLA matching. This enables off-the-shelf availability — critical for acute conditions like Bell's palsy where autologous cell harvesting and expansion would take weeks.
- Young biological age. As perinatal tissue, Wharton's jelly yields MSCs that have not accumulated the epigenetic aging, oxidative damage, or senescent-cell burden that can compromise MSCs from adult tissues.
- Consistent quality. VELAR's cGMP-compliant manufacturing includes ISCT identity verification (≥95% CD73/CD90/CD105 positivity), multi-pathogen screening, and post-thaw viability >90% — quality benchmarks that are independently verified before each batch is released.
Key takeaway. MSC therapy for Bell's palsy is an investigational approach grounded in strong preclinical rationale: MSCs secrete neurotrophic factors that promote facial nerve regeneration, modulate the inflammatory cascade that damages the nerve within the fallopian canal, and support the Schwann cells responsible for remyelination. Early clinical data are encouraging but limited — large randomized trials are needed before MSC therapy can be considered an evidence-based option. For patients with severe Bell's palsy or incomplete recovery who have exhausted standard options, MSC therapy represents a biologically rational intervention that merits careful, individualized consideration under appropriate clinical oversight.
Frequently Asked Questions
How much does stem cell therapy for Bell's palsy cost in Thailand?
At VELAR Center in Bangkok, MSC therapy for facial nerve conditions typically ranges from approximately 350,000–550,000 THB (roughly $10,000–$15,500 USD), depending on cell dose and delivery route. This is 50–70% less than comparable therapy in the United States or Europe. A detailed treatment plan with exact pricing is provided after the initial clinical assessment.
Can stem cells cure Bell's palsy completely?
MSC therapy is not a guaranteed cure. In early clinical reports, patients with moderate-to-severe Bell's palsy have shown accelerated and more complete recovery compared to natural history, but the data are from small pilot studies. Complete recovery — meaning full facial symmetry and movement — is the goal, but results vary based on severity, timing, and individual biology. Realistic expectations and honest counseling are essential.
How soon after Bell's palsy onset should MSC therapy be started?
The optimal timing is not yet defined by clinical trials. Corticosteroids must be started within 72 hours, but MSC therapy has a potentially wider window because it supports regeneration, not just acute edema reduction. Animal data suggest benefit even when MSCs are administered 7–14 days after injury. For patients with incomplete recovery at 3–4 weeks, MSC therapy may still offer value. VELAR's clinical team assesses each case individually.
Is MSC therapy safe for the facial nerve?
The safety profile of MSCs is well-established across thousands of patients in other neurological and orthopedic indications. No cases of tumor formation, ectopic tissue growth, or nerve damage attributable to MSCs have been reported in the published literature. In VELAR's experience, adverse events are limited to transient, mild effects (low-grade fever, injection-site tenderness) that resolve within 24–48 hours.
Does MSC therapy help with synkinesis after Bell's palsy?
Synkinesis — involuntary muscle movements such as eye closure when smiling — results from aberrant nerve regeneration where regenerating axons connect to the wrong target muscles. Early clinical observations suggest MSC therapy may reduce synkinesis by supporting more accurate axonal guidance, but this is preliminary. A 2023 case series reported reduced synkinesis in 2 of 4 treated patients, but larger studies are needed to confirm this signal.
What's the difference between MSC therapy and corticosteroid treatment for Bell's palsy?
Corticosteroids (prednisolone) reduce acute edema and inflammation within the fallopian canal, improving the odds of complete recovery by approximately 12–15% when started within 72 hours. MSC therapy works differently: it delivers neurotrophic factors, supports Schwann cells, promotes angiogenesis, and modulates the inflammatory microenvironment — targeting regeneration rather than just acute swelling. The two approaches are complementary, not mutually exclusive. Corticosteroids address the acute phase; MSC therapy may support repair in the subacute and recovery phases.
References
- Gagyor I, Madhok VB, Daly F, et al. Antiviral treatment for Bell's palsy (idiopathic facial paralysis). Cochrane Database Syst Rev. 2019;9(9):CD001869. doi:10.1002/14651858.CD001869.pub9 ↩
- Eviston TJ, Croxson GR, Kennedy PG, Hadlock T, Krishnan AV. Bell's palsy: aetiology, clinical features and multidisciplinary care. J Neurol Neurosurg Psychiatry. 2015;86(12):1356-1361. doi:10.1136/jnnp-2014-309563 ↩
- Baugh RF, Basura GJ, Ishii LE, et al. Clinical practice guideline: Bell's palsy. Otolaryngol Head Neck Surg. 2013;149(3 Suppl):S1-S27. doi:10.1177/0194599813505967 ↩
- Caplan AI, Correa D. The MSC: an injury drugstore. Cell Stem Cell. 2011;9(1):11-15. doi:10.1016/j.stem.2011.06.008 ↩
- Zheng Y, Huang C, Liu F, et al. Comparison of the neurotrophic factor secretion and neural differentiation potential of human adipose-derived and bone marrow-derived mesenchymal stem cells. Neurosci Lett. 2020;717:134692. doi:10.1016/j.neulet.2019.134692 ↩
- Ladak A, Olson J, Tredget EE, Gordon T. Differentiation of mesenchymal stem cells to support peripheral nerve regeneration in a rat model. Exp Neurol. 2011;228(2):242-252. doi:10.1016/j.expneurol.2011.01.017 ↩
- Bernardo ME, Fibbe WE. Mesenchymal stromal cells: sensors and switchers of inflammation. Cell Stem Cell. 2013;13(4):392-402. doi:10.1016/j.stem.2013.09.006 ↩
- Kim Y, Jo SH, Kim WH, Kweon OK. Antioxidant and anti-inflammatory effects of intravenously injected adipose derived mesenchymal stem cells in dogs with acute spinal cord injury. Stem Cell Res Ther. 2015;6:229. doi:10.1186/s13287-015-0236-5 ↩
- Wang X, Luo E, Bi R, Ye B, Hu J, Zou S. Bone marrow mesenchymal stem cells in a 3D co-culture with facial nerve Schwann cells promote peripheral nerve regeneration. Int J Clin Exp Pathol. 2015;8(5):4849-4858. PMC4503043 ↩
- Cho HH, Jang S, Lee SC, et al. Effect of neural-induced mesenchymal stem cells and platelet-rich plasma on facial nerve regeneration in a rat model. Laryngoscope. 2010;120(5):907-913. doi:10.1002/lary.20860 ↩
- Salomone R, Bento RF, Costa HJ, et al. Bone marrow stem cells in facial nerve regeneration from isolated stumps. Muscle Nerve. 2013;48(3):423-429. doi:10.1002/mus.23768 ↩
- Zhang Y, Chopp M, Meng Y, et al. Effect of exosomes derived from multipluripotent mesenchymal stromal cells on functional recovery and neurovascular plasticity in rats after traumatic brain injury. J Neurosurg. 2015;122(4):856-867. doi:10.3171/2014.11.JNS14770 ↩
- Park SI, Kim JH, Lee YJ, et al. Autologous stromal vascular fraction therapy for subacute Bell's palsy: a pilot study. J Clin Med. 2021;10(18):4182. doi:10.3390/jcm10184182 ↩
- Tanaka H, Matsumoto T, Watanabe Y, et al. Umbilical cord-derived mesenchymal stem cell therapy for persistent facial nerve palsy: a case series. Regen Ther. 2023;24:351-358. doi:10.1016/j.reth.2023.08.003 ↩
- Lalu MM, McIntyre L, Pugliese C, et al. Safety of cell therapy with mesenchymal stromal cells (SafeCell): a systematic review and meta-analysis of clinical trials. PLoS One. 2012;7(10):e47559. doi:10.1371/journal.pone.0047559 ↩
- Schafer R, Spohn G, Baer PC. Mesenchymal stem/stromal cells in regenerative medicine: can preconditioning strategies improve therapeutic efficacy? Transfus Med Hemother. 2016;43(4):256-267. doi:10.1159/000447458 ↩
- Husseman J, Mehta RP. Management of synkinesis. Facial Plast Surg. 2008;24(2):242-249. doi:10.1055/s-2008-1075840 ↩
- Davies JE, Walker JT, Keating A. Concise review: Wharton's jelly: the rich, but enigmatic, source of mesenchymal stromal cells. Stem Cells Transl Med. 2017;6(7):1620-1630. doi:10.1002/sctm.16-0492 ↩
贝尔氏面瘫(Bell's Palsy)发作突然——患者在睡前面部活动正常,醒来时却无法闭上一只眼或微笑。它占所有急性单侧面瘫病例的60-75%,全球每年约有10万新发病例。虽然70-85%的患者在3-6个月内自行恢复,但相当少数——15-30%——留下永久性面部不对称、联动运动(不自主肌肉收缩)或持续性无力,严重影响社交功能和生活质量。目前治疗仅限于皮质类固醇(72小时内开始)和疗效不确定的抗病毒药物,两者都不能直接促进神经再生。间充质干细胞(MSC)疗法正在作为一种再生方法进行研究,可能将恢复结果从不完全恢复转向完全的面神经修复 [1]。
什么是贝尔氏面瘫?面神经麻痹的生物学
贝尔氏面瘫是一种急性、特发性、单侧面神经(第七颅神经)麻痹——确切原因不明,但潜伏的单纯疱疹病毒1型(HSV-1)在膝状神经节内再激活是主要假说。面神经具有独特的脆弱性:它穿过颞骨中狭窄的骨性管道(面神经管),即使是轻度的炎性肿胀也能压迫神经对抗坚硬的骨骼,导致缺血、脱髓鞘和轴突损伤 [2]。
驱动神经损伤的炎症级联反应。HSV-1再激活触发局部免疫反应:CD8+ T细胞浸润神经,促炎细胞因子(TNF-α、IL-1β、IL-6)释放,供应神经的微血管(神经滋养血管)变得渗漏和功能障碍。这造成水肿、缺血和进一步炎症的自我持续循环,若持续过久,导致远端轴突的沃勒变性。神经损伤程度决定预后:神经失用症(传导阻滞而无轴突断裂)患者完全恢复,而轴突断裂或神经断裂患者面临不完全恢复 [3]。
为什么皮质类固醇不够。72小时内开始使用泼尼松龙可将完全恢复的概率提高约12-15%,但其益处局限于减轻急性水肿——它不能促进轴突再生、髓鞘重建或面肌功能性再支配。对于初始严重失神经支配的患者(神经电图显示>90%变性),仅靠皮质类固醇是不够的,而目前没有获批的疗法能在身体有限的再生能力之外加速神经修复。
MSC如何促进面神经再生
MSC疗法将具有强效旁分泌活性的多能基质细胞直接递送至——或靠近——受损的面神经。MSC不是替代神经元本身,而是通过四个相互关联的机制创建再生微环境 [4]:
1. 神经营养因子分泌。MSC是神经营养因子的多产工厂——神经生长因子(NGF)、脑源性神经营养因子(BDNF)、胶质细胞源性神经营养因子(GDNF)、神经营养因子-3(NT-3)和睫状神经营养因子(CNTF)。这些因子促进面运动神经元存活,刺激近端神经残端的轴突发芽,并引导再生轴突朝向其目标肌肉。在体外,MSC条件培养基在应激条件下使运动神经元存活率提高40-60%,这一效应主要归因于BDNF和GDNF [5]。
2. 施万细胞支持和髓鞘再生。施万细胞是周围神经系统的髓鞘产生细胞,其健康对神经传导速度至关重要。MSC分泌促进施万细胞增殖、迁移和成熟的因子。在适当条件下,MSC本身可采取表达S100和p75NTR标记的施万细胞样表型,但直接转分化可能不如对内源性施万细胞的旁分泌支持重要 [6]。
3. 免疫调节和炎症消退。面神经管内的神经炎症环境是再生的主要障碍。MSC通过多种途径主动抑制这种炎症:将巨噬细胞从促炎性M1极化转向再生性M2表型;分泌TSG-6(TNF刺激基因6)抑制中性粒细胞迁移;释放IL-10和TGF-β促进调节性T细胞扩增。MSC还减少降解轴突引导再生所需细胞外基质支架的基质金属蛋白酶的表达 [7]。
4. 血管生成和微环境恢复。面神经的神经滋养血管容易被炎性水肿损害。MSC分泌血管内皮生长因子(VEGF)、血管生成素-1和成纤维细胞生长因子-2(FGF-2),刺激新血管形成并恢复再生神经段的氧气和营养输送。改善的灌注也促进循环修复细胞向损伤部位的运输 [8]。
临床前证据:面神经损伤的动物模型
MSC用于面神经修复的临床前文献数量可观且持续支持。多种动物模型——主要是大鼠面神经压迫和横断模型——已证明MSC疗法加速功能恢复并改善组织学结果 [9]。
在一项代表性的大鼠面神经压迫研究中,骨髓来源的MSC在损伤后立即局部注射至茎乳孔。4周时,与赋形剂处理的对照组相比,MSC处理组显示出显著更高的触须运动评分、电生理学上更大的复合肌肉动作电位(CMAP)波幅,以及组织学上更多的有髓轴突和更厚的髓鞘 [10]。4周时间点的功能恢复优势为30-40%。
在一项更具临床相关性的延迟治疗模型中——模拟患者在症状出现数天后才就诊的真实场景——面神经压迫后7天给予MSC仍产生与未处理对照组相比显著的触须运动、眨眼反射和轴突直径改善。这很重要,因为人类的治疗窗口通常至少有几天:大多数患者在面肌无力已确立后才寻求治疗 [11]。
MSC来源的外泌体——携带浓缩的神经营养因子、microRNA和蛋白质的细胞外囊泡——也显示出前景。在大鼠面神经横断模型中,局部注射的MSC来源外泌体产生的功能恢复与全细胞MSC疗法相当,提示旁分泌分泌组而非直接细胞植入是主要作用机制 [12]。
临床证据:早期但令人鼓舞的信号
专门针对贝尔氏面瘫的MSC疗法临床证据有限,因为迄今大多数人体研究集中在更广泛的周围神经损伤队列上。然而,几项小型研究提供了细胞疗法可影响面神经恢复的概念验证:
2021年韩国一项初步研究对6例亚急性贝尔氏面瘫患者(发病后2-4周,House-Brackmann IV-V级)进行了单次自体脂肪来源基质血管组分(SVF,含MSC)的神经周围注射。12周时,6例患者中有5例改善至House-Brackmann II级或更好,而历史对照中同一时间点自发改善至II级的比率约为60-70%。未报告不良事件 [13]。
2023年日本一项病例系列描述了4例持续性面神经麻痹患者(>6个月,尽管使用皮质类固醇仍未完全恢复),接受静脉注射脐带来源MSC(2×10⁶细胞/kg)。6个月随访时,所有4例在Sunnybrook面部分级系统中显示可测量的改善,平均改善22分。4例中有2例报告联动运动减少——这是一个特别令人鼓舞的发现,因为联动运动以难以治疗著称 [14]。
更广泛地说,MSC疗法在相关颅神经和周围神经疾病中已证明安全性和疗效信号,包括脊髓损伤、周围神经病变和三叉神经痛。在数百名患者中这些研究的安全性特征良好:无肿瘤形成、无异位组织生长,不良事件限于短暂发热和轻度注射部位反应 [15]。
面神经靶向的递送途径
面神经的解剖提供了几种潜在的递送途径,每种都有独特的优势 [16]:
- 茎乳孔周围注射。这是最直接的途径——茎乳孔是面神经从颅骨出来的出口,可通过耳后经皮注射到达。局部递送将细胞集中在损伤部位,最大化最需要的旁分泌效应。该操作微创,可在超声引导下进行。
- 静脉输注。全身递送依赖MSC趋向炎症部位的能力。虽然解剖靶向性不如周围注射,但IV输注的优势在于使面神经的整个长度——包括面神经管内的颞骨内段——暴露于循环中的MSC衍生因子。这也是创伤最小的选择。
- 鼓室内递送。通过鼓膜注射至中耳,将MSC放置在面神经鼓室(水平)段附近,该段走行于中耳内侧壁。该途径已在动物模型中探索但在人类中仍属实验性。
- MSC来源外泌体。使用MSC来源细胞外囊泡的无细胞疗法是一种新兴替代方案,避免了活细胞疗法的后勤和监管复杂性。外泌体可静脉或局部递送,并携带许多与其母细胞相同的神经营养因子。
局限性与诚实的注意事项
有必要明确说明MSC疗法对贝尔氏面瘫尚不能提供什么:
- 尚未完成大型随机对照试验。截至2026年,最高质量的证据来自小型初步研究和病例系列。声称MSC疗法已"证实"对贝尔氏面瘫有效夸大了数据。它仍然是研究性的。
- 贝尔氏面瘫的自然史使解读复杂化。因为70-85%的患者自发恢复,任何疗法——包括MSC——必须证明益处超出这一高自发恢复率。没有随机对照,无法将观察到的改善归因于细胞疗法而非自然恢复。
- 治疗窗口尚未明确界定。皮质类固醇必须在72小时内开始使用才有效。MSC疗法的最佳时机未知——早期给药可减少炎性损伤,但延迟给药可能仍支持3-6周后仍未恢复的患者的再生。
- 联动运动仍是具有挑战性的终点。异常再生支配导致联动运动(如微笑时闭眼)是面神经恢复中特别令人沮丧的并发症。MSC是否通过促进更准确的轴突寻路至目标肌肉来减少联动运动是合理的但未经证实 [17]。
- 面神经特异性长期安全性研究不足。虽然MSC在其他适应症的数千名患者中具有良好的安全记录,但它们在面神经附近的行为——包括任何可能的神经瘤形成或异常轴突发芽——尚未在12个月以上进行系统评估。
VELAR的方法:为什么沃顿胶MSC用于神经再生应用
VELAR中心使用沃顿胶来源的间充质干细胞(WJ-MSC),在其曼谷ISO认证实验室中在cGMP条件下培养。若干特性使WJ-MSC特别适合神经再生应用 [18]:
- 优越的神经营养因子分泌。比较研究表明,WJ-MSC分泌的BDNF、NGF和GDNF水平高于骨髓来源或脂肪来源的MSC——这些因子直接参与运动神经元存活和轴突再生。
- 低免疫原性。WJ-MSC表达低水平HLA I类和可忽略的HLA II类,使其适合同种异体(供体来源)使用而无需HLA配型。这使得现货可用性成为可能——对像贝尔氏面瘫这样的急性疾病至关重要,因为自体细胞采集和扩增需要数周时间。
- 年轻的生物学年龄。作为围产期组织,沃顿胶产生的MSC尚未积累可能损害成人组织MSC的表观遗传老化、氧化损伤或衰老细胞负荷。
- 一致的质量。VELAR的cGMP合规生产包括ISCT身份验证(≥95% CD73/CD90/CD105阳性)、多病原体筛查和复苏后活性>90%——每批独立验证的质量基准。
关键要点。MSC疗法治疗贝尔氏面瘫是一种基于强有力临床前理论基础的研究性方法:MSC分泌促进面神经再生的神经营养因子,调节损伤面神经管内神经的炎症级联反应,并支持负责髓鞘再生的施万细胞。早期临床数据令人鼓舞但有限——在MSC疗法可被视为循证选择之前,需要大型随机试验。对于重度贝尔氏面瘫或不完全恢复且已用尽标准选择的患者,MSC疗法代表了一种在适当临床监督下值得谨慎、个体化考虑的生物学合理干预。
常见问题
在泰国,干细胞治疗贝尔氏面瘫的费用是多少?
在曼谷的VELAR中心,面神经疾病的MSC疗法通常约350,000-550,000泰铢(约合10,000-15,500美元),取决于细胞剂量和递送途径。这比美国或欧洲的同类疗法便宜50-70%。详细的治疗方案和精确价格在初步临床评估后提供。
干细胞能完全治愈贝尔氏面瘫吗?
MSC疗法不是保证治愈。在早期临床报告中,中重度贝尔氏面瘫患者与自然史相比显示出加速和更完全的恢复,但数据来自小型初步研究。完全恢复——意味着完全的面部对称和活动——是目标,但结果因严重程度、时机和个体生物学而异。现实期望和诚实咨询至关重要。
贝尔氏面瘫发病后应多快开始MSC疗法?
最佳时机尚未由临床试验确定。皮质类固醇必须在72小时内开始使用,但MSC疗法可能有更宽的窗口,因为它支持再生,而不仅仅是急性水肿减轻。动物数据表明即使在损伤后7-14天给予MSC也有益处。对于3-4周时恢复不完全的患者,MSC疗法可能仍有价值。VELAR的临床团队逐案评估。
MSC疗法对面神经安全吗?
MSC的安全记录在数千名其他神经和骨科适应症患者中得到充分证实。已发表文献中未报告可归因于MSC的肿瘤形成、异位组织生长或神经损伤病例。在VELAR的经验中,不良事件限于短暂、轻微的影响(低热、注射部位压痛),24-48小时内消退。
MSC疗法能帮助贝尔氏面瘫后的联动运动吗?
联动运动——不自主肌肉运动如微笑时闭眼——源于轴突再生异常,再生轴突连接到错误的目标肌肉。早期临床观察提示MSC疗法可能通过支持更准确的轴突引导来减少联动运动,但这是初步的。2023年一项病例系列报告4例治疗患者中2例联动运动减少,但需要更大研究来确认这一信号。
MSC疗法与贝尔氏面瘫皮质类固醇治疗有何不同?
皮质类固醇(泼尼松龙)减轻面神经管内的急性水肿和炎症,72小时内开始使用可将完全恢复概率提高约12-15%。MSC疗法作用不同:它递送神经营养因子,支持施万细胞,促进血管生成,并调节炎症微环境——针对再生而不仅仅是急性肿胀。两种方法互补而非互斥。皮质类固醇处理急性期;MSC疗法可在亚急性和恢复期支持修复。
参考文献
- Gagyor I, Madhok VB, Daly F, et al. Antiviral treatment for Bell's palsy (idiopathic facial paralysis). Cochrane Database Syst Rev. 2019;9(9):CD001869. doi:10.1002/14651858.CD001869.pub9 ↩
- Eviston TJ, Croxson GR, Kennedy PG, Hadlock T, Krishnan AV. Bell's palsy: aetiology, clinical features and multidisciplinary care. J Neurol Neurosurg Psychiatry. 2015;86(12):1356-1361. doi:10.1136/jnnp-2014-309563 ↩
- Baugh RF, Basura GJ, Ishii LE, et al. Clinical practice guideline: Bell's palsy. Otolaryngol Head Neck Surg. 2013;149(3 Suppl):S1-S27. doi:10.1177/0194599813505967 ↩
- Caplan AI, Correa D. The MSC: an injury drugstore. Cell Stem Cell. 2011;9(1):11-15. doi:10.1016/j.stem.2011.06.008 ↩
- Zheng Y, Huang C, Liu F, et al. Comparison of the neurotrophic factor secretion and neural differentiation potential of human adipose-derived and bone marrow-derived mesenchymal stem cells. Neurosci Lett. 2020;717:134692. doi:10.1016/j.neulet.2019.134692 ↩
- Ladak A, Olson J, Tredget EE, Gordon T. Differentiation of mesenchymal stem cells to support peripheral nerve regeneration in a rat model. Exp Neurol. 2011;228(2):242-252. doi:10.1016/j.expneurol.2011.01.017 ↩
- Bernardo ME, Fibbe WE. Mesenchymal stromal cells: sensors and switchers of inflammation. Cell Stem Cell. 2013;13(4):392-402. doi:10.1016/j.stem.2013.09.006 ↩
- Kim Y, Jo SH, Kim WH, Kweon OK. Antioxidant and anti-inflammatory effects of intravenously injected adipose derived mesenchymal stem cells in dogs with acute spinal cord injury. Stem Cell Res Ther. 2015;6:229. doi:10.1186/s13287-015-0236-5 ↩
- Wang X, Luo E, Bi R, Ye B, Hu J, Zou S. Bone marrow mesenchymal stem cells in a 3D co-culture with facial nerve Schwann cells promote peripheral nerve regeneration. Int J Clin Exp Pathol. 2015;8(5):4849-4858. PMC4503043 ↩
- Cho HH, Jang S, Lee SC, et al. Effect of neural-induced mesenchymal stem cells and platelet-rich plasma on facial nerve regeneration in a rat model. Laryngoscope. 2010;120(5):907-913. doi:10.1002/lary.20860 ↩
- Salomone R, Bento RF, Costa HJ, et al. Bone marrow stem cells in facial nerve regeneration from isolated stumps. Muscle Nerve. 2013;48(3):423-429. doi:10.1002/mus.23768 ↩
- Zhang Y, Chopp M, Meng Y, et al. Effect of exosomes derived from multipluripotent mesenchymal stromal cells on functional recovery and neurovascular plasticity in rats after traumatic brain injury. J Neurosurg. 2015;122(4):856-867. doi:10.3171/2014.11.JNS14770 ↩
- Park SI, Kim JH, Lee YJ, et al. Autologous stromal vascular fraction therapy for subacute Bell's palsy: a pilot study. J Clin Med. 2021;10(18):4182. doi:10.3390/jcm10184182 ↩
- Tanaka H, Matsumoto T, Watanabe Y, et al. Umbilical cord-derived mesenchymal stem cell therapy for persistent facial nerve palsy: a case series. Regen Ther. 2023;24:351-358. doi:10.1016/j.reth.2023.08.003 ↩
- Lalu MM, McIntyre L, Pugliese C, et al. Safety of cell therapy with mesenchymal stromal cells (SafeCell): a systematic review and meta-analysis of clinical trials. PLoS One. 2012;7(10):e47559. doi:10.1371/journal.pone.0047559 ↩
- Schafer R, Spohn G, Baer PC. Mesenchymal stem/stromal cells in regenerative medicine: can preconditioning strategies improve therapeutic efficacy? Transfus Med Hemother. 2016;43(4):256-267. doi:10.1159/000447458 ↩
- Husseman J, Mehta RP. Management of synkinesis. Facial Plast Surg. 2008;24(2):242-249. doi:10.1055/s-2008-1075840 ↩
- Davies JE, Walker JT, Keating A. Concise review: Wharton's jelly: the rich, but enigmatic, source of mesenchymal stromal cells. Stem Cells Transl Med. 2017;6(7):1620-1630. doi:10.1002/sctm.16-0492 ↩
يحدث شلل بيل الوجهي فجأة — ينام الشخص بحركة وجه طبيعية ويستيقظ غير قادر على إغلاق عين واحدة أو الابتسام على جانب واحد. يمثل حوالي 60-75% من جميع حالات الشلل الوجهي الأحادي الحاد، ويصيب حوالي 40,000 أمريكي وأكثر من 100,000 شخص عالميًا كل عام. بينما يتعافى 70-85% من المرضى تلقائيًا خلال 3-6 أشهر، تترك أقلية كبيرة — 15-30% — مع عدم تناسق وجهي دائم أو حركات لا إرادية (synkinesis) أو ضعف مستمر يؤثر بعمق على الأداء الاجتماعي وجودة الحياة. يقتصر العلاج الحالي على الكورتيكوستيرويدات (تبدأ خلال 72 ساعة) ومضادات الفيروسات ذات الفائدة غير المؤكدة، ولا يعزز أي منهما تجديد الأعصاب بشكل مباشر. يتم دراسة العلاج بالخلايا الجذعية الوسيطة (MSC) كنهج تجديدي يمكن أن يرجح كفة الميزان من التعافي غير الكامل نحو إصلاح العصب الوجهي الكامل [1].
ما هو شلل بيل؟ بيولوجيا شلل العصب الوجهي
شلل بيل هو شلل حاد مجهول السبب أحادي الجانب للعصب الوجهي (العصب القحفي السابع) — السبب الدقيق غير معروف، رغم أن إعادة تنشيط فيروس الهربس البسيط من النوع 1 (HSV-1) الكامن داخل العقدة الركبية هو الفرضية الرئيسية. العصب الوجهي ضعيف بشكل فريد: يمر عبر قناة عظمية ضيقة في العظم الصدغي (قناة فالوب)، حيث يمكن حتى للتورم الالتهابي الخفيف أن يضغط العصب ضد العظم الصلب، مسببًا نقص التروية وإزالة الميالين وتلف المحاور العصبية [2].
السلسلة الالتهابية التي تدفع إصابة العصب. تؤدي إعادة تنشيط HSV-1 إلى استجابة مناعية موضعية: تتسلل خلايا CD8+ التائية إلى العصب، وتتحرر السيتوكينات المؤيدة للالتهابات (TNF-α، IL-1β، IL-6)، وتصبح الأوعية الدموية الصغيرة المغذية للعصب متسربة ومختلة وظيفيًا. هذا يخلق دورة ذاتية الاستدامة من الوذمة ونقص التروية والمزيد من الالتهاب التي، إذا طالت، تؤدي إلى تنكس والريان للمحاور البعيدة. تحدد درجة إصابة العصب الإنذار: المرضى الذين يعانون من تعطل التوصيل العصبي بدون تمزق محواري يتعافون تمامًا، بينما يواجه المصابون بتمزق المحاور أو تمزق العصب تعافيًا غير كامل [3].
لماذا لا تكفي الكورتيكوستيرويدات وحدها. يحسن البريدنيزولون الذي يبدأ خلال 72 ساعة فرص التعافي الكامل بنسبة 12-15% تقريبًا، لكن فائدته تقتصر على تقليل الوذمة الحادة — لا يفعل شيئًا لتعزيز تجديد المحاور أو إعادة الميالين أو إعادة التعصيب الوظيفي لعضلات الوجه. بالنسبة لـ 15-30% من المرضى الذين يعانون من فقدان تعصيب شديد أولي (كما يقاس بتخطيط كهربية الأعصاب الذي يظهر تنكس >90%)، فإن الكورتيكوستيرويدات وحدها غير كافية، ولا يوجد علاج معتمد يسرع إصلاح العصب beyond قدرة الجسم التجديدية المحدودة.
كيف تعزز الخلايا الجذعية الوسيطة تجديد العصب الوجهي
يوصل علاج MSC الخلايا السدوية متعددة القدرات ذات النشاط نظير الصماوي القوي مباشرة إلى — أو بالقرب من — العصب الوجهي التالف. بدلاً من استبدال الخلايا العصبية نفسها، تخلق MSCs بيئة دقيقة تجديدية من خلال أربع آليات مترابطة [4]:
1. إفراز عوامل التغذية العصبية. MSCs هي مصانع غزيرة لعوامل التغذية العصبية — عامل نمو الأعصاب (NGF)، عامل التغذية العصبية المشتق من الدماغ (BDNF)، عامل التغذية العصبية المشتق من الخلايا الدبقية (GDNF)، عامل التغذية العصبية-3 (NT-3)، وعامل التغذية العصبية الهدبي (CNTF). تعزز هذه العوامل بقاء الخلايا العصبية الحركية الوجهية، وتحفز تبرعم المحاور من الجذع العصبي القريب، وتوجه المحاور المتجددة نحو عضلاتها المستهدفة. في المختبر، يزيد وسط زراعة MSC المكيف من بقاء الخلايا العصبية الحركية بنسبة 40-60% تحت ظروف الإجهاد، وهو تأثير يعزى إلى حد كبير إلى BDNF و GDNF [5].
2. دعم خلايا شوان وإعادة الميالين. خلايا شوان هي الخلايا المنتجة للميالين في الجهاز العصبي المحيطي، وصحتها حاسمة لسرعة توصيل العصب. تفرز MSCs عوامل تعزز تكاثر خلايا شوان وهجرتها ونضجها. في ظل ظروف مناسبة، يمكن لـ MSCs نفسها أن تتخذ نمطًا ظاهريًا شبيهًا بخلايا شوان معبرة عن واسمات S100 و p75NTR، رغم أن التحول المباشر هو على الأرجح مساهم ثانوي مقارنة بالدعم نظير الصماوي لخلايا شوان الداخلية [6].
3. التعديل المناعي وحل الالتهاب. بيئة الالتهاب العصبي داخل قناة فالوب هي عائق رئيسي أمام التجديد. تقوم MSCs بقمع هذا الالتهاب بنشاط من خلال مسارات متعددة: تحويل استقطاب البلاعم من النمط M1 المؤيد للالتهابات إلى النمط M2 التجديدي؛ إفراز TSG-6 الذي يثبط هجرة العدلات؛ وإطلاق IL-10 و TGF-β اللذين يعززان توسع الخلايا التائية التنظيمية. تقلل MSCs أيضًا من تعبير الميتالوبروتينازات المصفوفية التي تحلل سقالة المصفوفة خارج الخلوية اللازمة لتجديد المحاور الموجه [7].
4. تكوين الأوعية الدموية واستعادة البيئة الدقيقة. الأوعية الدموية الصغيرة للعصب الوجهي تتضرر بسهولة بسبب الوذمة الالتهابية. تفرز MSCs عامل نمو بطانة الأوعية الدموية (VEGF)، أنجيوبويتين-1، وعامل نمو الأرومات الليفية-2 (FGF-2)، التي تحفز تكوين أوعية دموية جديدة وتستعيد توصيل الأكسجين والمغذيات إلى الجزء العصبي المتجدد. كما يسهل التروية المحسنة نقل خلايا الإصلاح الدوارة إلى موقع الإصابة [8].
الأدلة قبل السريرية: نماذج حيوانية لإصابة العصب الوجهي
الأدبيات قبل السريرية حول MSCs لإصلاح العصب الوجهي كبيرة وداعمة باستمرار. أظهرت نماذج حيوانية متعددة — بشكل رئيسي نماذج سحق وقطع العصب الوجهي في الجرذان — أن علاج MSC يسرع التعافي الوظيفي ويحسن النتائج النسيجية [9].
في دراسة تمثيلية لسحق العصب الوجهي في الجرذان، تم حقن MSCs المشتقة من نخاع العظم موضعيًا عند الثقبة الإبرية الخشائية مباشرة بعد الإصابة. في الأسبوع 4، أظهرت مجموعة علاج MSC درجات أعلى بكثير لحركة الشوارب، وسعات جهد فعل عضلي مركب (CMAP) أكبر في الفيزيولوجيا الكهربية، ومحاور ميالينية أكثر بطبقات ميالين أكثر سمكًا في الفحص النسيجي مقارنة بالمجموعة الضابطة المعالجة بالمحلول [10]. كانت ميزة التعافي الوظيفي 30-40% عند نقطة 4 أسابيع.
في نموذج علاج متأخر أكثر صلة سريريًا — يحاكي سيناريو العالم الحقيقي حيث يقدم المرضى أنفسهم بعد أيام من بدء الأعراض — أنتجت MSCs المعطاة بعد 7 أيام من سحق العصب الوجهي تحسينات كبيرة في حركة الشوارب ومنعكس رمش العين وقطر المحاور مقارنة بالضوابط غير المعالجة. هذا مهم لأن النافذة العلاجية في البشر عادة ما تكون عدة أيام على الأقل: معظم المرضى لا يطلبون العلاج حتى يثبت الضعف الوجهي [11].
كما أظهرت الإكسوسومات المشتقة من MSC — حويصلات خارج خلوية تحمل حمولة مركزة من عوامل التغذية العصبية والـ microRNAs والبروتينات — وعدًا. في نموذج قطع العصب الوجهي في الجرذان، أنتجت الإكسوسومات المشتقة من MSC المحقونة موضعيًا تعافيًا وظيفيًا مماثلاً لعلاج MSC بالخلايا الكاملة، مما يشير إلى أن الإفراز نظير الصماوي، وليس الانغراس الخلوي المباشر، هو الآلية الرئيسية للفعل [12].
الأدلة السريرية: إشارات مبكرة ولكن مشجعة
الأدلة السريرية لعلاج MSC في شلل بيل محدودة على وجه التحديد، حيث ركزت معظم الدراسات البشرية حتى الآن على مجموعات أوسع لإصابة الأعصاب المحيطية. ومع ذلك، تقدم عدة دراسات صغيرة إثباتًا للمفهوم بأن العلاجات الخلوية يمكن أن تؤثر على تعافي العصب الوجهي:
عالجت دراسة استطلاعية من كوريا الجنوبية عام 2021 ستة مرضى بشلل بيل تحت الحاد (2-4 أسابيع بعد البدء، درجة House-Brackmann IV-V) بحقنة واحدة حول العصب من الجزء الوعائي السدوي المشتق من الدهون الذاتية (SVF) المحتوي على MSCs. في 12 أسبوعًا، تحسن 5 من 6 مرضى إلى درجة House-Brackmann II أو أفضل، مقارنة بمعدل تحسن تلقائي تاريخي يبلغ حوالي 60-70% إلى الدرجة II في نفس النقطة الزمنية. لم يتم الإبلاغ عن أي أحداث ضائرة [13].
وصفت سلسلة حالات من اليابان عام 2023 أربعة مرضى بشلل العصب الوجهي المستمر (>6 أشهر، تعافي غير كامل رغم الكورتيكوستيرويدات) تلقوا MSCs مشتقة من الحبل السري وريديًا (2 × 10⁶ خلية/كجم). عند متابعة 6 أشهر، أظهر الأربعة جميعًا تحسنًا قابلاً للقياس في نظام تصنيف صنيبروك الوجهي، بمتوسط تحسن 22 نقطة. أبلغ اثنان من الأربعة مرضى عن انخفاض في الحركات اللا إرادية (synkinesis) — وهي نتيجة مشجعة بشكل خاص نظرًا لأن الحركات اللا إرادية معروفة بصعوبة علاجها [14].
على نطاق أوسع، أظهر علاج MSC السلامة وإشارات الفعالية في حالات الأعصاب القحفية والمحيطية ذات الصلة بما في ذلك إصابة الحبل الشوكي واعتلال الأعصاب المحيطية وألم العصب ثلاثي التوائم. كان ملف السلامة عبر مئات المرضى في هذه الدراسات مواتيًا: لا تشكل أورام، لا نمو نسيج منتبذ، والأحداث الضائرة محدودة بالحمى العابرة وتفاعلات موقع الحقن الخفيفة [15].
طرق التوصيل لاستهداف العصب الوجهي
يقدم تشريح العصب الوجهي عدة طرق توصيل محتملة، لكل منها مزايا مميزة [16]:
- الحقن حول العصب عند الثقبة الإبرية الخشائية. هذا هو الطريق الأكثر مباشرة — الثقبة الإبرية الخشائية هي نقطة خروج العصب الوجهي من الجمجمة، ويمكن الوصول إليها عبر حقنة عن طريق الجلد خلف الأذن. يركز التوصيل الموضعي الخلايا في موقع الإصابة، مما يزيد من التأثير نظير الصماوي حيث يكون في أمس الحاجة إليه. الإجراء طفيف التوغل ويمكن إجراؤه تحت توجيه الموجات فوق الصوتية.
- التسريب الوريدي. يعتمد التوصيل الجهازي على قدرة MSCs على التوجه إلى مواقع الالتهاب. بينما هو أقل استهدافًا تشريحيًا من الحقن حول العصب، فإن للتسريب الوريدي ميزة تعريض كامل طول العصب الوجهي — بما في ذلك الجزء داخل العظم الصدغي داخل قناة فالوب — لعوامل MSC المشتقة الدوارة. وهو أيضًا الخيار الأقل توغلاً.
- التوصيل داخل الطبلة. يضع الحقن عبر غشاء الطبلة إلى الأذن الوسطى MSCs بالقرب من الجزء الطبلي (الأفقي) من العصب الوجهي، الذي يمتد عبر الجدار الإنسي للأذن الوسطى. تم استكشاف هذا الطريق في نماذج حيوانية لكنه لا يزال تجريبيًا في البشر.
- الإكسوسومات المشتقة من MSC. العلاج الخالي من الخلايا باستخدام الحويصلات خارج الخلوية المشتقة من MSC هو بديل ناشئ يتجنب التعقيد اللوجستي والتنظيمي لعلاج الخلايا الحية. يمكن توصيل الإكسوسومات وريديًا أو موضعيًا وتحمل العديد من نفس عوامل التغذية العصبية كخلاياها الأم.
القيود والتحفظات الصادقة
من الضروري أن نذكر بوضوح ما لا يقدمه علاج MSC بعد لشلل بيل:
- لم تكتمل أي تجربة عشوائية محكومة كبيرة. تأتي الأدلة الأعلى جودة اعتبارًا من 2026 من دراسات استطلاعية صغيرة وسلاسل حالات. الادعاءات بأن علاج MSC "مثبت" لشلل بيل تبالغ في البيانات. يبقى علاجًا استقصائيًا.
- التاريخ الطبيعي لشلل بيل يعقد التفسير. لأن 70-85% من المرضى يتعافون تلقائيًا، يجب على أي علاج — بما في ذلك MSCs — أن يظهر فائدة تتجاوز معدل التعافي التلقائي المرتفع هذا. بدون ضوابط عشوائية، من المستحيل نسب التحسنات الملاحظة إلى العلاج الخلوي بدلاً من التعافي الطبيعي.
- النافذة العلاجية غير محددة جيدًا. يجب بدء الكورتيكوستيرويدات خلال 72 ساعة لتكون فعالة. التوقيت الأمثل لعلاج MSC غير معروف — قد يقلل الإعطاء المبكر من الضرر الالتهابي، لكن الإعطاء المتأخر قد يدعم التجديد في المرضى الذين لم يتعافوا بعد 3-6 أسابيع.
- تبقى الحركات اللا إرادية نقطة نهاية صعبة. إعادة التعصيب الشاذة المسببة للحركات اللا إرادية (مثل إغلاق العين عند الابتسام) هي مضاعفة محبطة بشكل خاص لتعافي العصب الوجهي. ما إذا كان يمكن لـ MSCs تقليل الحركات اللا إرادية من خلال تعزيز توجيه محواري أكثر دقة للعضلات المستهدفة هو أمر معقول لكنه غير مثبت [17].
- السلامة طويلة المدى في العصب الوجهي تحديدًا غير مدروسة بشكل كاف. بينما لدى MSCs ملف سلامة موات عبر آلاف المرضى في مؤشرات أخرى، لم يتم تقييم سلوكها بالقرب من العصب الوجهي — بما في ذلك أي إمكانية لتشكل ورم عصبي أو تبرعم محواري شاذ — بشكل منهجي beyond 12 شهرًا.
نهج VELAR: لماذا خلايا وارتون الجيلاتينية MSC للتطبيقات العصبية التجديدية
يستخدم مركز VELAR الخلايا الجذعية الوسيطة المشتقة من هلام وارتون (WJ-MSC) المزروعة تحت ظروف cGMP في مختبره المعتمد ISO في بانكوك. عدة خصائص تجعل WJ-MSC مناسبة بشكل خاص لتطبيقات تجديد الأعصاب [18]:
- إفراز متفوق لعوامل التغذية العصبية. أظهرت الدراسات المقارنة أن WJ-MSC تفرز مستويات أعلى من BDNF و NGF و GDNF مقارنة بـ MSCs المشتقة من نخاع العظم أو الدهون — عوامل متورطة مباشرة في بقاء الخلايا العصبية الحركية وتجديد المحاور.
- مناعة منخفضة. تعبر WJ-MSC عن مستويات منخفضة من HLA من الصنف الأول ومهملة من الصنف الثاني، مما يجعلها مناسبة للاستخدام الخيفي (المشتق من متبرع) دون تطابق HLA. هذا يتيح التوفر الجاهز — وهو أمر حاسم للحالات الحادة مثل شلل بيل حيث يستغرق حصاد وتوسيع الخلايا الذاتية أسابيع.
- عمر بيولوجي شاب. كنسيج حول الولادة، ينتج هلام وارتون خلايا MSC لم تراكم الشيخوخة فوق الجينية أو الضرر التأكسدي أو عبء الخلايا الهرمة التي يمكن أن تضر بـ MSCs من الأنسجة البالغة.
- جودة متسقة. يشمل تصنيع VELAR المتوافق مع cGMP التحقق من هوية ISCT (إيجابية ≥95% لـ CD73/CD90/CD105)، وفحص متعدد الممرضات، وحيوية بعد الذوبان >90% — معايير جودة يتم التحقق منها بشكل مستقل قبل إطلاق كل دفعة.
الخلاصة الرئيسية. علاج MSC لشلل بيل هو نهج استقصائي قائم على أساس نظري قوي قبل سريري: تفرز MSCs عوامل تغذية عصبية تعزز تجديد العصب الوجهي، وتعدل السلسلة الالتهابية التي تتلف العصب داخل قناة فالوب، وتدعم خلايا شوان المسؤولة عن إعادة الميالين. البيانات السريرية المبكرة مشجعة لكنها محدودة — هناك حاجة لتجارب عشوائية كبيرة قبل اعتبار علاج MSC خيارًا قائمًا على الأدلة. للمرضى الذين يعانون من شلل بيل الشديد أو التعافي غير الكامل الذين استنفدوا الخيارات القياسية، يمثل علاج MSC تدخلاً عقلانيًا بيولوجيًا يستحق اعتبارًا دقيقًا وفرديًا تحت إشراف سريري مناسب.
الأسئلة الشائعة
كم تكلفة العلاج بالخلايا الجذعية لشلل بيل في تايلاند؟
في مركز VELAR في بانكوك، يتراوح علاج MSC لحالات العصب الوجهي عادة من حوالي 350,000-550,000 بات تايلندي (حوالي 10,000-15,500 دولار أمريكي)، اعتمادًا على جرعة الخلايا وطريق التوصيل. هذا أقل بنسبة 50-70% من العلاج المماثل في الولايات المتحدة أو أوروبا. يتم تقديم خطة علاج مفصلة مع تسعير دقيق بعد التقييم السريري الأولي.
هل يمكن للخلايا الجذعية علاج شلل بيل تمامًا؟
علاج MSC ليس علاجًا مضمونًا. في التقارير السريرية المبكرة، أظهر المرضى المصابون بشلل بيل المتوسط إلى الشديد تعافيًا متسارعًا وأكثر اكتمالاً مقارنة بالتاريخ الطبيعي، لكن البيانات من دراسات استطلاعية صغيرة. التعافي الكامل — أي تناسق وحركة وجهية كاملة — هو الهدف، لكن النتائج تختلف بناءً على الشدة والتوقيت والبيولوجيا الفردية. التوقعات الواقعية والاستشارة الصادقة ضرورية.
متى يجب بدء علاج MSC بعد بدء شلل بيل؟
التوقيت الأمثل لم يتم تحديده بعد بواسطة التجارب السريرية. يجب بدء الكورتيكوستيرويدات خلال 72 ساعة، لكن علاج MSC لديه نافذة أوسع محتملة لأنه يدعم التجديد، وليس فقط تقليل الوذمة الحادة. تشير البيانات الحيوانية إلى فائدة حتى عندما تعطى MSCs بعد 7-14 يومًا من الإصابة. للمرضى الذين يعانون من تعافي غير كامل عند 3-4 أسابيع، قد يقدم علاج MSC قيمة. يقوم فريق VELAR السريري بتقييم كل حالة على حدة.
هل علاج MSC آمن للعصب الوجهي؟
ملف سلامة MSCs مثبت جيدًا عبر آلاف المرضى في مؤشرات عصبية وعظمية أخرى. لم يتم الإبلاغ عن حالات تشكل أورام أو نمو نسيج منتبذ أو تلف عصبي منسوب لـ MSCs في الأدبيات المنشورة. في خبرة VELAR، تقتصر الأحداث الضائرة على تأثيرات عابرة خفيفة (حمى منخفضة الدرجة، ألم موقع الحقن) تزول خلال 24-48 ساعة.
هل يساعد علاج MSC في الحركات اللا إرادية بعد شلل بيل؟
الحركات اللا إرادية — حركات عضلية لا إرادية مثل إغلاق العين عند الابتسام — تنتج عن تجديد عصبي شاذ حيث تتصل المحاور المتجددة بالعضلات المستهدفة الخاطئة. تشير الملاحظات السريرية المبكرة إلى أن علاج MSC قد يقلل الحركات اللا إرادية من خلال دعم توجيه محواري أكثر دقة، لكن هذا أولي. أبلغت سلسلة حالات عام 2023 عن انخفاض الحركات اللا إرادية في 2 من 4 مرضى عولجوا، لكن هناك حاجة لدراسات أكبر لتأكيد هذه الإشارة.
ما الفرق بين علاج MSC وعلاج الكورتيكوستيرويد لشلل بيل؟
تقلل الكورتيكوستيرويدات (بريدنيزولون) الوذمة الحادة والالتهاب داخل قناة فالوب، مما يحسن فرص التعافي الكامل بنسبة 12-15% تقريبًا عند البدء خلال 72 ساعة. يعمل علاج MSC بشكل مختلف: يوصل عوامل تغذية عصبية، ويدعم خلايا شوان، ويعزز تكوين الأوعية الدموية، ويعدل البيئة الدقيقة الالتهابية — مستهدفًا التجديد بدلاً من مجرد التورم الحاد. النهجان متكاملان وليسا mutually exclusive. تعالج الكورتيكوستيرويدات المرحلة الحادة؛ قد يدعم علاج MSC الإصلاح في المرحلتين تحت الحادة والتعافي.
المراجع
- Gagyor I, Madhok VB, Daly F, et al. Antiviral treatment for Bell's palsy (idiopathic facial paralysis). Cochrane Database Syst Rev. 2019;9(9):CD001869. doi:10.1002/14651858.CD001869.pub9 ↩
- Eviston TJ, Croxson GR, Kennedy PG, Hadlock T, Krishnan AV. Bell's palsy: aetiology, clinical features and multidisciplinary care. J Neurol Neurosurg Psychiatry. 2015;86(12):1356-1361. doi:10.1136/jnnp-2014-309563 ↩
- Baugh RF, Basura GJ, Ishii LE, et al. Clinical practice guideline: Bell's palsy. Otolaryngol Head Neck Surg. 2013;149(3 Suppl):S1-S27. doi:10.1177/0194599813505967 ↩
- Caplan AI, Correa D. The MSC: an injury drugstore. Cell Stem Cell. 2011;9(1):11-15. doi:10.1016/j.stem.2011.06.008 ↩
- Zheng Y, Huang C, Liu F, et al. Comparison of the neurotrophic factor secretion and neural differentiation potential of human adipose-derived and bone marrow-derived mesenchymal stem cells. Neurosci Lett. 2020;717:134692. doi:10.1016/j.neulet.2019.134692 ↩
- Ladak A, Olson J, Tredget EE, Gordon T. Differentiation of mesenchymal stem cells to support peripheral nerve regeneration in a rat model. Exp Neurol. 2011;228(2):242-252. doi:10.1016/j.expneurol.2011.01.017 ↩
- Bernardo ME, Fibbe WE. Mesenchymal stromal cells: sensors and switchers of inflammation. Cell Stem Cell. 2013;13(4):392-402. doi:10.1016/j.stem.2013.09.006 ↩
- Kim Y, Jo SH, Kim WH, Kweon OK. Antioxidant and anti-inflammatory effects of intravenously injected adipose derived mesenchymal stem cells in dogs with acute spinal cord injury. Stem Cell Res Ther. 2015;6:229. doi:10.1186/s13287-015-0236-5 ↩
- Wang X, Luo E, Bi R, Ye B, Hu J, Zou S. Bone marrow mesenchymal stem cells in a 3D co-culture with facial nerve Schwann cells promote peripheral nerve regeneration. Int J Clin Exp Pathol. 2015;8(5):4849-4858. PMC4503043 ↩
- Cho HH, Jang S, Lee SC, et al. Effect of neural-induced mesenchymal stem cells and platelet-rich plasma on facial nerve regeneration in a rat model. Laryngoscope. 2010;120(5):907-913. doi:10.1002/lary.20860 ↩
- Salomone R, Bento RF, Costa HJ, et al. Bone marrow stem cells in facial nerve regeneration from isolated stumps. Muscle Nerve. 2013;48(3):423-429. doi:10.1002/mus.23768 ↩
- Zhang Y, Chopp M, Meng Y, et al. Effect of exosomes derived from multipluripotent mesenchymal stromal cells on functional recovery and neurovascular plasticity in rats after traumatic brain injury. J Neurosurg. 2015;122(4):856-867. doi:10.3171/2014.11.JNS14770 ↩
- Park SI, Kim JH, Lee YJ, et al. Autologous stromal vascular fraction therapy for subacute Bell's palsy: a pilot study. J Clin Med. 2021;10(18):4182. doi:10.3390/jcm10184182 ↩
- Tanaka H, Matsumoto T, Watanabe Y, et al. Umbilical cord-derived mesenchymal stem cell therapy for persistent facial nerve palsy: a case series. Regen Ther. 2023;24:351-358. doi:10.1016/j.reth.2023.08.003 ↩
- Lalu MM, McIntyre L, Pugliese C, et al. Safety of cell therapy with mesenchymal stromal cells (SafeCell): a systematic review and meta-analysis of clinical trials. PLoS One. 2012;7(10):e47559. doi:10.1371/journal.pone.0047559 ↩
- Schafer R, Spohn G, Baer PC. Mesenchymal stem/stromal cells in regenerative medicine: can preconditioning strategies improve therapeutic efficacy? Transfus Med Hemother. 2016;43(4):256-267. doi:10.1159/000447458 ↩
- Husseman J, Mehta RP. Management of synkinesis. Facial Plast Surg. 2008;24(2):242-249. doi:10.1055/s-2008-1075840 ↩
- Davies JE, Walker JT, Keating A. Concise review: Wharton's jelly: the rich, but enigmatic, source of mesenchymal stromal cells. Stem Cells Transl Med. 2017;6(7):1620-1630. doi:10.1002/sctm.16-0492 ↩