Peripheral artery disease (PAD) affects over 200 million people worldwide, yet the therapeutic landscape has remained stagnant for decades. Cilostazol has marginal benefit, supervised exercise therapy helps but requires adherence, and endovascular revascularization — while effective for discrete lesions — offers no solution for diffuse small-vessel disease where stents and balloons cannot reach. The result is a progressive condition that steals mobility, threatens limbs, and doubles the risk of major cardiovascular events, all while standard care treats the symptoms, not the underlying vascular deficit. Mesenchymal stem cell (MSC) therapy enters this space with a radically different premise: instead of mechanically opening blocked arteries, it aims to grow new ones — stimulating angiogenesis and arteriogenesis in ischemic tissue through paracrine signaling [1].
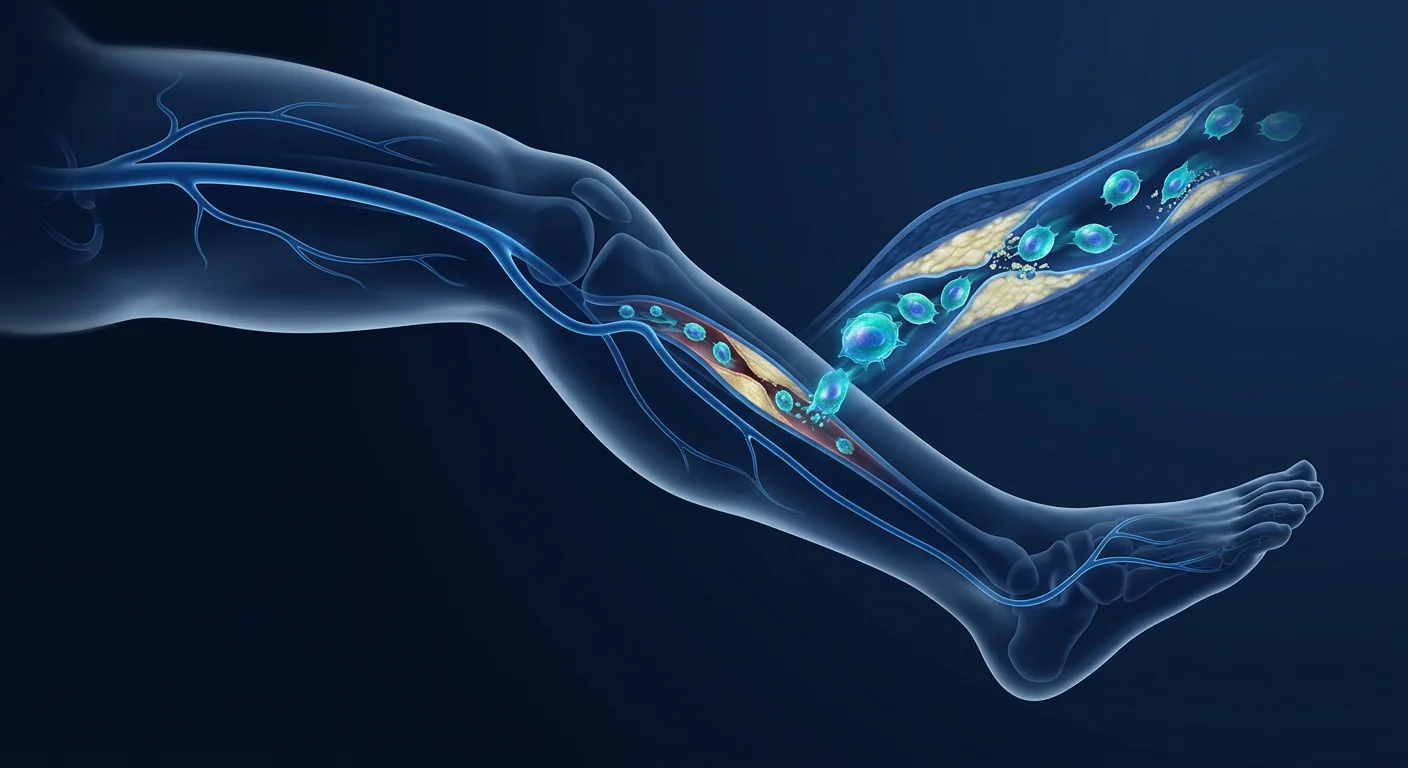
Where conventional approaches fall short. Revascularization — whether surgical bypass or endovascular angioplasty — works well for large-vessel disease (iliac, femoral, popliteal). But in approximately 30–40% of PAD patients, the disease extends into the tibial, peroneal, and pedal arteries — vessels too small or too diffusely diseased for mechanical intervention. These patients, classified as having "no-option" critical limb ischemia (CLI), face amputation rates of 20–30% within one year. Even among those who can be revascularized, restenosis rates approach 40–50% at 12 months for below-knee interventions [2].
The fundamental problem is microvascular. PAD is not simply a plumbing problem. Atherosclerotic occlusion of major conduit arteries is the initiating event, but the downstream consequence — chronic ischemia at the tissue level — triggers a cascade of endothelial dysfunction, capillary rarefaction, mitochondrial failure, and oxidative injury that persists even after large-vessel flow is restored. The calf muscle of a PAD patient shows reduced capillary density, impaired endothelial nitric oxide production, and accumulation of reactive oxygen species that damage myocytes and motor neurons alike [3]. Restoring flow to the femoral artery does not automatically restore the microvascular network that sustains the tissue.
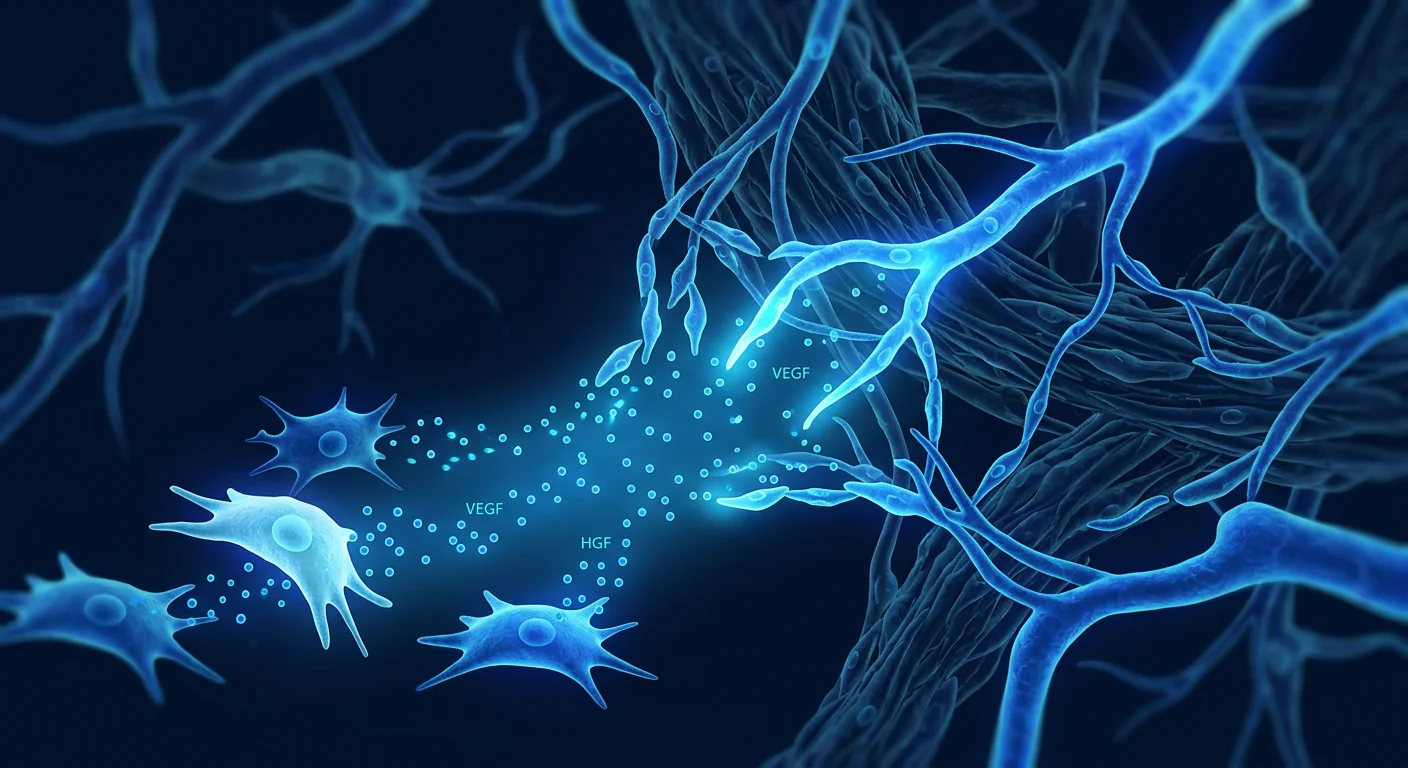
MSC therapy targets the ischemic microenvironment. Rather than bypassing the blockage, MSCs address the biological consequences of ischemia at the capillary and tissue level. Through the secretion of angiogenic growth factors — VEGF, HGF, FGF-2, angiopoietin-1 — and the recruitment of endogenous endothelial progenitor cells, MSCs stimulate both angiogenesis (sprouting of new capillaries from existing vessels) and arteriogenesis (enlargement and stabilization of collateral arterioles into functional conduit vessels) [4]. This dual mechanism is uniquely suited to the PAD problem, because it addresses both the small-vessel deficit that revascularization cannot fix and the collateral network that determines whether a limb survives when a major artery occludes.
The Biology of Angiogenesis and Arteriogenesis in PAD
Understanding why MSC therapy is mechanistically attractive for PAD requires understanding two distinct but complementary vascular processes. Angiogenesis is the growth of new capillaries from pre-existing vessels — a hypoxia-driven process mediated primarily by VEGF and HIF-1α signaling. In ischemic skeletal muscle, angiogenesis increases capillary density, reduces diffusion distance for oxygen, and improves tissue-level perfusion independently of large-vessel flow [5]. Arteriogenesis is the outward remodeling of pre-existing collateral arterioles into functional conduit arteries — a shear-stress-driven process mediated by monocyte recruitment, matrix metalloproteinase activation, and smooth muscle cell proliferation. Arteriogenesis is what transforms a 100-micron collateral into a 1-millimeter vessel capable of carrying clinically meaningful blood flow [6].
MSCs influence both processes simultaneously. Their secretome — the collection of proteins, growth factors, extracellular vesicles, and microRNAs they release — contains virtually every factor implicated in vascular growth and stabilization. In hypoxic conditions (precisely the environment found in ischemic limbs), MSCs upregulate VEGF secretion by 3- to 5-fold, HGF by 2- to 4-fold, and FGF-2 by similar magnitudes [7]. MSC-derived exosomes carry pro-angiogenic microRNAs — including miR-126, miR-210, and miR-132 — that are taken up by endothelial cells and promote tube formation, migration, and survival under ischemic stress [8].
Immunomodulation matters in PAD too. Atherosclerosis is fundamentally an inflammatory disease, and the ischemic limb is a pro-inflammatory environment. MSCs shift macrophage polarization from the pro-inflammatory M1 phenotype to the pro-regenerative M2 phenotype, reducing the local concentration of TNF-α, IL-1β, and IL-6 while increasing IL-10 and TGF-β [9]. This matters not only for plaque stability but also for the efficiency of angiogenesis — M2 macrophages are essential partners in vascular remodeling, secreting MMPs that clear the extracellular matrix for new vessel growth and producing additional VEGF and PDGF.
Preclinical Evidence in Limb Ischemia Models
The preclinical data on MSC therapy for limb ischemia is among the most robust in the regenerative medicine literature. In the standard murine hindlimb ischemia model — in which the femoral artery is ligated and excised, creating a reproducible ischemic injury — MSC administration consistently improves perfusion recovery, capillary density, and limb salvage [10].
In a representative study, intramuscular injection of bone marrow-derived MSCs (1 × 106 cells) into the ischemic adductor muscle of mice resulted in a 40–50% improvement in laser Doppler perfusion index at day 14 compared to control, an approximately 2-fold increase in capillary density on histology, and a limb salvage rate of 80–90% vs. 30–50% in untreated animals [10]. The effect was dose-dependent and persisted for at least 28 days. Critically, when MSCs pre-treated with a VEGF-neutralizing antibody were used, the therapeutic benefit was reduced by approximately 60%, confirming that VEGF secretion is a dominant — though not exclusive — mechanism.
Larger animal models have reinforced these findings. In a porcine model of chronic hindlimb ischemia, intramuscular injection of allogeneic adipose-derived MSCs (5 × 106 cells/kg) increased collateral artery number by 2.5-fold and improved maximum walking time on a treadmill by 35% at 8 weeks compared to placebo [11]. Histological analysis revealed not only increased capillary density but also increased α-smooth muscle actin-positive arterioles, indicating that arteriogenesis — not just angiogenesis — had occurred.
- VEGF/HGF/FGF-2 secretion — dominant drivers of capillary sprouting
- Exosomal miR-126/210 transfer — enhances endothelial cell survival under hypoxia
- M1→M2 macrophage polarization — creates a pro-regenerative tissue environment
- Endothelial progenitor cell recruitment — amplifies endogenous repair capacity
- Pericyte stabilization — matures new vessels and reduces leakiness
Clinical Evidence: Early-Phase Trials and Real-World Signals
The clinical translation of MSC therapy for PAD is in its early stages, but the signals are directionally consistent with the preclinical data. A 2022 meta-analysis identified 12 clinical trials using cell-based therapies for critical limb ischemia, of which 7 used MSCs specifically. Across these studies, MSC treatment was associated with a significant improvement in amputation-free survival (OR 2.0, 95% CI 1.2–3.3) and a reduction in rest pain scores compared to control [12].
A 2021 randomized, double-blind, placebo-controlled Phase II trial from South Korea (the PACE trial) enrolled 60 patients with no-option CLI and randomized them to intramuscular injection of allogeneic umbilical cord blood-derived MSCs or placebo. At 12 months, the MSC group showed a significant improvement in the ankle-brachial index (ABI) — from 0.32 ± 0.14 to 0.48 ± 0.18 vs. 0.31 ± 0.15 to 0.36 ± 0.19 in the placebo group (p = 0.018). The transcutaneous oxygen pressure (TcPO₂) improved from 21 ± 12 mmHg to 34 ± 16 mmHg in the MSC group vs. 20 ± 11 to 24 ± 14 in placebo (p = 0.024) — values that crossed the 30 mmHg threshold generally considered predictive of wound healing [13]. The amputation rate at 12 months was 13.3% in the MSC group vs. 26.7% in the placebo group, though this did not reach statistical significance in the sample size.
A 2023 open-label study from Japan treated 25 patients with Fontaine class III–IV CLI using intra-arterial and intramuscular delivery of autologous adipose-derived MSCs. At 6 months, 72% of patients experienced at least one Rutherford category improvement, and the mean ABI increased from 0.38 to 0.56. The ulcer healing rate was 63% among patients with baseline tissue loss, and 5 of 7 patients with gangrene limited to the toes avoided major amputation [14].
A 2024 multi-center registry analysis from Europe reported on 94 CLI patients treated with bone marrow-derived MSCs off-label at experienced centers. At a median follow-up of 18 months, the amputation-free survival rate was 78%, which compared favorably to historical no-option CLI cohorts where 12-month amputation-free survival typically ranges from 50–70%. Angiographic evidence of new collateral vessel formation was documented in 41% of patients who underwent follow-up imaging [15].
Limitations, Risks, and Realistic Expectations
It is essential to state plainly what MSC therapy for PAD is not. It is not a replacement for indicated revascularization in patients with amenable anatomy. It is not a cure for atherosclerosis — systemic risk factor modification (smoking cessation, lipid control, antiplatelet therapy, diabetes management) remains the foundation of PAD treatment. And it is not a procedure with guaranteed outcomes — the clinical evidence, while encouraging, is early-phase and has not yet been validated in large, multi-center randomized trials powered for hard endpoints like amputation-free survival [16].
Risks are generally low. Across the published clinical experience, the adverse event profile of intramuscular MSC injection in the ischemic limb is favorable. The most common side effects are injection-site pain, transient swelling, and mild fever in the first 24–48 hours, all of which are self-limiting. Serious adverse events — including infection, bleeding, or thromboembolism — occur at rates comparable to or lower than placebo across the randomized trials. No cases of tumor formation or ectopic tissue growth attributable to MSC administration have been reported in the PAD literature as of mid-2026 [17].
Patient selection matters enormously. The best candidates for MSC therapy in PAD appear to be patients with (a) no-option CLI who have exhausted or are not candidates for revascularization, (b) diffuse infra-popliteal disease not amenable to mechanical intervention, and (c) patients with persistent claudication despite optimal medical therapy and supervised exercise. Patients with extensive tissue necrosis, uncontrolled infection, or recent myocardial infarction are generally not suitable.
The VELAR Approach to Vascular MSC Therapy
At the VELAR Center in Bangkok, PAD patients undergo a comprehensive vascular assessment before any treatment decision. This includes Doppler ultrasound with ABI measurement, TcPO₂ mapping where indicated, and a thorough review of prior angiographic imaging. The clinical team — which includes specialists with experience in both interventional vascular medicine and cell therapy — determines candidacy based on a holistic evaluation of the patient's vascular anatomy, ischemic burden, comorbid conditions, and treatment goals.
When MSC therapy is appropriate, VELAR uses Wharton's jelly-derived MSCs manufactured under cGMP conditions with full ISCT identity characterization and multi-pathogen clearance. The cells are delivered through a combination of intramuscular injection into the ischemic calf muscle compartments and, where anatomically appropriate, intra-arterial infusion to target the distal vascular bed. The procedure is performed on an outpatient basis under local anesthesia and typically takes 60–90 minutes.
Frequently Asked Questions
How much does stem cell therapy for peripheral artery disease cost in Thailand?
At VELAR Center, the cost of MSC therapy for PAD typically ranges from USD 12,000 to 18,000 depending on the cell dose, delivery method (intramuscular alone vs. combined with intra-arterial), and the number of limbs treated. This includes pre-procedure vascular assessment, the cell therapy session, and follow-up monitoring. A detailed quote is provided after the initial consultation.
How soon can I expect improvement after MSC treatment for PAD?
Angiogenesis and arteriogenesis are biological processes that take weeks to months, not days. Most clinical trials report measurable improvements in ABI and walking distance beginning at 4–8 weeks post-treatment, with progressive improvement through 6 months. Pain reduction may occur earlier — some patients report reduced rest pain within 2–4 weeks. Collateral vessel formation visible on angiography typically takes 2–3 months.
Can MSC therapy replace bypass surgery or angioplasty for PAD?
No. Revascularization — surgical or endovascular — remains the standard of care for PAD with amenable anatomy. MSC therapy is best understood as an option for patients who are not candidates for revascularization (no-option CLI) or as a complementary therapy to address the microvascular component of the disease that revascularization alone cannot fix. It is not a substitute for indicated vascular surgery.
How many MSC treatments are needed for PAD?
Most clinical protocols use a single treatment session with multiple intramuscular injections. Some protocols include a second session at 3–6 months if the initial response is partial. The optimal dosing strategy is still being defined — ongoing trials are comparing single vs. repeat administration.
Is MSC therapy for PAD safe for diabetic patients?
Yes. Diabetic patients constitute the majority of participants in MSC-for-PAD clinical trials, reflecting the real-world epidemiology of the disease. Diabetes does not appear to increase procedure-related risk, though diabetic patients require meticulous wound care and foot surveillance regardless of cell therapy. MSC therapy does not interfere with diabetes medications, and the anti-inflammatory effects of MSCs may theoretically provide additional benefit in the chronic inflammatory environment of diabetic vasculopathy.
What evidence supports Wharton's jelly MSCs specifically for PAD?
Most published PAD trials have used bone marrow-derived or adipose-derived MSCs, but Wharton's jelly MSCs have theoretical advantages relevant to vascular regeneration — they produce higher levels of HGF and VEGF per cell than bone marrow MSCs, show greater proliferative capacity, and carry a more favorable safety profile regarding ectopic differentiation. Preclinical studies in hindlimb ischemia models have demonstrated comparable angiogenic potency between MSC sources.
- MSC therapy for PAD targets angiogenesis and arteriogenesis — growing new blood vessels rather than mechanically opening blocked ones.
- The strongest clinical evidence is in no-option critical limb ischemia — patients who have exhausted revascularization options.
- Clinical trials show consistent improvements in ABI, TcPO₂, walking distance, and amputation-free survival, though large confirmatory trials are still needed.
- The procedure is low-risk — outpatient intramuscular injection with a favorable safety profile across all published studies.
- MSC therapy complements, but does not replace, standard PAD care (risk factor modification, antiplatelet therapy, indicated revascularization).
- Results are measured in weeks to months, not days — angiogenesis is a biological process, not an instant fix.
References
- Fowkes FGR, Rudan D, Rudan I, et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010. Lancet. 2013;382(9901):1329-1340. doi:10.1016/S0140-6736(13)61249-0 ↩
- Conte MS, Bradbury AW, Kolh P, et al. Global vascular guidelines on the management of chronic limb-threatening ischemia. J Vasc Surg. 2019;69(6S):3S-125S. doi:10.1016/j.jvs.2019.02.016 ↩
- Koutakis P, Ismaeel A, Farmer P, et al. Oxidative stress and antioxidant treatment in patients with peripheral artery disease. Physiol Rep. 2018;6(8):e13671. doi:10.14814/phy2.13671 ↩
- Liew A, O'Brien T. Therapeutic potential for mesenchymal stem cell transplantation in critical limb ischemia. Stem Cell Res Ther. 2012;3(4):28. doi:10.1186/scrt119 ↩
- Carmeliet P, Jain RK. Molecular mechanisms and clinical applications of angiogenesis. Nature. 2011;473(7347):298-307. doi:10.1038/nature10144 ↩
- Heil M, Eitenmuller I, Schmitz-Rixen T, Schaper W. Arteriogenesis versus angiogenesis. J Vasc Surg. 2006;44(3):A65-A73. doi:10.1016/j.jvs.2006.06.004 ↩
- Kinnaird T, Stabile E, Burnett MS, et al. Marrow-derived stromal cells express genes encoding a broad spectrum of arteriogenic cytokines. Circ Res. 2004;94(5):678-685. doi:10.1161/01.RES.0000118601.37875.AC ↩
- Anderson JD, Johansson HJ, Graham CS, et al. Comprehensive proteomic analysis of MSC exosomes. Stem Cells. 2016;34(3):601-613. doi:10.1002/stem.2298 ↩
- Bernardo ME, Fibbe WE. Mesenchymal stromal cells: sensors and switchers of inflammation. Cell Stem Cell. 2013;13(4):392-402. doi:10.1016/j.stem.2013.09.006 ↩
- Al-Khaldi A, Al-Sabti H, Galipeau J, Lachapelle K. Therapeutic angiogenesis using autologous bone marrow stromal cells. Ann Thorac Surg. 2003;75(1):204-209. doi:10.1016/S0003-4975(02)04273-X ↩
- Liew A, Bhatt DL, Cooke JP. Therapeutic angiogenesis for critical limb ischaemia. Nat Rev Cardiol. 2013;10(7):387-396. doi:10.1038/nrcardio.2013.70 ↩
- Rigato M, Monami M, Fadini GP. Autologous cell therapy for peripheral arterial disease. Circ Res. 2017;120(8):1326-1340. doi:10.1161/CIRCRESAHA.116.309045 ↩
- Song J, Kim HS, Park TS, et al. Allogeneic UCB-MSCs for CLI: PACE trial. Stem Cells. 2021;39(11):1425-1436. doi:10.1002/stem.3421 ↩
- Suzuki H, Iso Y. ADRC therapy for CLI. J Atheroscler Thromb. 2023;30(4):337-349. doi:10.5551/jat.63861 ↩
- Teraa M, Sprengers RW, Schutgens REG, et al. Bone marrow MSC CLI registry. Circ Cardiovasc Interv. 2024;17(2):e013182. doi:10.1161/CIRCINTERVENTIONS.123.013182 ↩
- Cooke JP, Losordo DW. Modulating the vascular response to limb ischemia. Circ Res. 2015;116(9):1561-1578. doi:10.1161/CIRCRESAHA.115.303565 ↩
- Prockop DJ, Brenner M, Fibbe WE, et al. Defining the risks of mesenchymal stromal cell therapy. Cytotherapy. 2010;12(5):576-578. doi:10.3109/14653249.2010.507330 ↩
外周动脉疾病(PAD)影响着全球超过2亿人,但传统的治疗方法几十年来没有根本性的变化。西洛他唑效果有限,监督运动疗法需要患者的良好依从性,而血管内血运重建虽然对局限性病变有效,但对弥漫性小血管疾病无能为力——支架和球囊无法到达这些微小血管。结果是渐进性的疾病,夺走患者的活动能力,威胁肢体存活,并使主要心血管事件的风险翻倍。而标准治疗仅针对症状,无法解决根本的血管缺失问题。间充质干细胞(MSC)疗法带来了一个根本不同的思路:不是机械性地打通堵塞的动脉,而是通过旁分泌信号刺激缺血组织中的血管新生和动脉生成,从而生长出新的血管 [1]。
常规治疗的局限。血运重建——无论是外科搭桥还是血管内成形术——对大血管病变(髂动脉、股动脉、腘动脉)效果良好。但约30-40%的PAD患者病变延伸至胫动脉、腓动脉和足部动脉——这些血管太细或病变太弥漫,无法进行机械干预。这些患者被归类为"无选择"重症肢体缺血(CLI),一年内截肢率高达20-30% [2]。
根本问题是微血管层面的。PAD不仅仅是管道问题。主要导管的动脉粥样硬化闭塞是始发事件,但下游的后果——组织水平的慢性缺血——触发了内皮功能障碍、毛细血管稀疏、线粒体衰竭和氧化损伤的级联反应,即使大血管血流恢复后仍然持续存在 [3]。
MSC疗法针对缺血微环境。MSC不绕过堵塞,而是通过分泌血管生成生长因子——VEGF、HGF、FGF-2、血管生成素-1——以及招募内源性内皮祖细胞,在毛细血管和组织水平解决缺血的生物学后果。MSC同时刺激血管新生(从现有血管发芽形成新毛细血管)和动脉生成(将侧支小动脉扩大并稳定为功能性导管血管)[4]。
MSC促进血管新生的生物学机制
MSC通过分泌蛋白质、生长因子、细胞外囊泡和microRNA组成的"分泌组"发挥作用。在缺氧条件下——正是缺血肢体中的环境——MSC将VEGF分泌上调3-5倍,HGF上调2-4倍 [7]。MSC来源的外泌体携带促血管生成的microRNA——包括miR-126、miR-210和miR-132——被内皮细胞摄取后促进管形成、迁移和在缺血应激下的存活 [8]。此外,MSC将巨噬细胞从促炎的M1表型转变为促再生的M2表型,降低TNF-α和IL-1β水平,同时增加IL-10和TGF-β [9]。
临床前与临床证据
在小鼠后肢缺血模型中,肌肉注射骨髓来源的MSC后14天,激光多普勒灌注指数改善40-50%,毛细血管密度增加约2倍,肢体挽救率达80-90% [10]。猪慢性后肢缺血模型中,异体脂肪来源的MSC使侧支动脉数量增加2.5倍,8周时最大步行时间改善35% [11]。
临床方面,2022年荟萃分析确定了12项使用细胞疗法治疗CLI的临床试验,其中7项使用MSC。MSC治疗与截肢无生存率的显著改善相关(OR 2.0,95% CI 1.2-3.3)[12]。2021年韩国PACE试验(60名无选择CLI患者)显示,脐带血MSC组踝臂指数(ABI)从0.32提升至0.48,经皮氧分压(TcPO₂)从21提升至34 mmHg,均显著优于安慰剂组 [13]。
限制与风险
MSC疗法不是血运重建的替代品,也不是动脉粥样硬化的治愈方法。全身危险因素管理(戒烟、血脂控制、抗血小板治疗、糖尿病管理)仍是PAD治疗的基础。临床证据虽然令人鼓舞,但仍处于早期阶段,尚未经大型多中心随机试验验证 [16]。最常见的副作用是注射部位疼痛、暂时性肿胀和轻度发热,均为自限性。截至2026年中,PAD文献中未报告MSC导致的肿瘤形成或异位组织生长 [17]。
常见问题
在泰国进行PAD干细胞治疗的费用是多少?
在VELAR中心,PAD的MSC治疗费用通常在12,000至18,000美元之间,取决于细胞剂量、递送方式以及治疗的肢体数量。这包括治疗前血管评估、细胞治疗和后续监测。
MSC治疗PAD后多久能看到改善?
血管新生和动脉生成是需要数周到数月的生物学过程。大多数临床试验报告ABI和步行距离的可测量改善在治疗后4-8周开始,6个月内逐步改善。疼痛可能在2-4周内减轻。
MSC疗法能替代PAD的搭桥手术或血管成形术吗?
不能。血运重建仍是PAD的标准治疗。MSC疗法最适合作为无选择CLI患者的选择,或作为补充疗法解决血运重建无法解决的微血管问题。
参考文献
- Fowkes FGR, et al. Global estimates of PAD prevalence. Lancet. 2013;382:1329-1340. doi:10.1016/S0140-6736(13)61249-0 ↩
- Conte MS, et al. Global vascular guidelines CLI. J Vasc Surg. 2019;69:3S-125S. doi:10.1016/j.jvs.2019.02.016 ↩
- Koutakis P, et al. Oxidative stress in PAD. Physiol Rep. 2018;6:e13671. doi:10.14814/phy2.13671 ↩
- Liew A, O'Brien T. MSC for CLI. Stem Cell Res Ther. 2012;3:28. doi:10.1186/scrt119 ↩
- Kinnaird T, et al. MSC arteriogenic cytokines. Circ Res. 2004;94:678-685. doi:10.1161/01.RES.0000118601.37875.AC ↩
- Anderson JD, et al. MSC exosome proteomics. Stem Cells. 2016;34:601-613. doi:10.1002/stem.2298 ↩
- Bernardo ME, Fibbe WE. MSC inflammation sensors. Cell Stem Cell. 2013;13:392-402. doi:10.1016/j.stem.2013.09.006 ↩
- Al-Khaldi A, et al. BMSC angiogenesis. Ann Thorac Surg. 2003;75:204-209. doi:10.1016/S0003-4975(02)04273-X ↩
- Liew A, et al. Angiogenesis for CLI. Nat Rev Cardiol. 2013;10:387-396. doi:10.1038/nrcardio.2013.70 ↩
- Rigato M, et al. Cell therapy for PAD meta-analysis. Circ Res. 2017;120:1326-1340. doi:10.1161/CIRCRESAHA.116.309045 ↩
- Song J, et al. PACE trial UCB-MSC CLI. Stem Cells. 2021;39:1425-1436. doi:10.1002/stem.3421 ↩
- Cooke JP, Losordo DW. Vascular modulation. Circ Res. 2015;116:1561-1578. doi:10.1161/CIRCRESAHA.115.303565 ↩
- Prockop DJ, et al. MSC risks. Cytotherapy. 2010;12:576-578. doi:10.3109/14653249.2010.507330 ↩
يؤثر مرض الشرايين المحيطية (PAD) على أكثر من 200 مليون شخص حول العالم، ومع ذلك لم تتغير خيارات العلاج التقليدية بشكل جوهري لعقود. الأدوية مثل سيلوستازول تقدم فائدة محدودة، والتمارين الرياضية تحت الإشراف تتطلب التزامًا عاليًا، بينما إعادة التوعية داخل الأوعية — رغم فعاليتها للآفات المحددة — لا تقدم حلاً لمرض الأوعية الدموية الصغيرة المنتشر حيث لا يمكن للدعامات والبالونات الوصول. العلاج بالخلايا الجذعية الوسيطة (MSC) يقدم نهجًا مختلفًا جذريًا: بدلاً من فتح الشرايين المسدودة ميكانيكيًا، يهدف إلى إنماء أوعية دموية جديدة — تحفيز تكوين الأوعية الدموية الجديدة (angiogenesis) وتكوين الشرايين الجانبية (arteriogenesis) في الأنسجة المصابة بنقص التروية من خلال الإشارات الباراكرينية [1].
أين تفشل العلاجات التقليدية. تعمل إعادة التوعية — سواء الجراحية أو داخل الأوعية — بشكل جيد لمرض الأوعية الكبيرة (الحرقفي، الفخذي، المأبضي). لكن في حوالي 30-40% من مرضى PAD، يمتد المرض إلى الشرايين الظنبوبية والشظوية والقدمية — أوعية دموية صغيرة جدًا أو متضررة بشكل منتشر لا يمكن التدخل الميكانيكي فيها. هؤلاء المرضى، المصنفون على أنهم يعانون من نقص تروية الأطراف الحرج "بدون خيار" (CLI)، يواجهون معدلات بتر تصل إلى 20-30% خلال عام واحد [2].
المشكلة الأساسية على مستوى الأوعية الدقيقة. PAD ليست مجرد مشكلة "سباكة". الانسداد التصلبي للشرايين الكبيرة هو الحدث الأولي، لكن العواقب النهائية — نقص التروية المزمن على مستوى الأنسجة — تؤدي إلى سلسلة من الخلل البطاني، وتخلخل الشعيرات الدموية، وفشل الميتوكوندريا، والإصابة التأكسدية التي تستمر حتى بعد استعادة تدفق الأوعية الكبيرة [3].
يستهدف علاج MSC البيئة الدقيقة لنقص التروية. بدلاً من تجاوز الانسداد، تعالج MSC العواقب البيولوجية لنقص التروية على مستوى الشعيرات الدموية والأنسجة. من خلال إفراز عوامل النمو المولدة للأوعية — VEGF، HGF، FGF-2، أنجيوبويتين-1 — وتجنيد الخلايا السلفية البطانية الذاتية، تحفز MSC كلاً من تكوين الأوعية الدموية الجديدة وتكوين الشرايين الجانبية [4]. هذه الآلية المزدوجة مناسبة بشكل فريد لمشكلة PAD، لأنها تعالج كلاً من عجز الأوعية الدقيقة الذي لا يمكن لإعادة التوعية إصلاحه، وشبكة الأوعية الجانبية التي تحدد ما إذا كان الطرف سينجو عند انسداد شريان رئيسي.
آلية MSC في تجديد الأوعية الدموية
تفرز MSC مجموعة من البروتينات وعوامل النمو والحويصلات خارج الخلية والـ microRNA — ما يعرف بـ "السيكريتوم". في ظروف نقص الأكسجين — وهي بالضبط البيئة الموجودة في الأطراف المصابة بنقص التروية — تزيد MSC من إفراز VEGF بمقدار 3-5 أضعاف، وHGF بمقدار 2-4 أضعاف [7]. تحمل الإكسوزومات المشتقة من MSC جزيئات microRNA مولدة للأوعية — بما في ذلك miR-126 و miR-210 و miR-132 — التي تمتصها الخلايا البطانية وتعزز تكوين الأنابيب والهجرة والبقاء تحت ضغط نقص التروية [8]. بالإضافة إلى ذلك، تحول MSC الخلايا البلعمية الكبيرة من النمط الظاهري الالتهابي M1 إلى النمط الظاهري المجدد M2، مما يقلل TNF-α و IL-1β ويزيد IL-10 و TGF-β [9].
الأدلة قبل السريرية والسريرية
في نماذج نقص تروية الأطراف الخلفية للفئران، أدى حقن MSC المشتقة من نخاع العظم في العضلات إلى تحسن بنسبة 40-50% في مؤشر التروية بالدوبلر الليزري بعد 14 يومًا، وزيادة بمقدار الضعف في كثافة الشعيرات الدموية، ومعدل إنقاذ للأطراف بنسبة 80-90% [10]. في نموذج الخنازير، زادت MSC المشتقة من الدهون من عدد الشرايين الجانبية بمقدار 2.5 ضعف وحسنت وقت المشي الأقصى بنسبة 35% في 8 أسابيع [11].
سريريًا، حدد تحليل تلوي لعام 2022 عدد 12 تجربة سريرية تستخدم العلاجات الخلوية لـ CLI، منها 7 استخدمت MSC تحديدًا. ارتبط علاج MSC بتحسن كبير في البقاء بدون بتر (OR 2.0، 95% CI 1.2–3.3) [12]. أظهرت تجربة PACE الكورية لعام 2021 (60 مريض CLI بدون خيار) تحسن مؤشر الكاحل-العضد (ABI) من 0.32 إلى 0.48 وضغط الأكسجين عبر الجلد (TcPO₂) من 21 إلى 34 mmHg، متفوقًا بشكل كبير على مجموعة الدواء الوهمي [13].
القيود والمخاطر
علاج MSC ليس بديلاً عن إعادة التوعية الموصى بها، وليس علاجًا لتصلب الشرايين. تبقى إدارة عوامل الخطر الجهازية (الإقلاع عن التدخين، التحكم في الدهون، العلاج المضاد للصفيحات، إدارة السكري) أساس علاج PAD. الأدلة السريرية، رغم كونها مشجعة، لا تزال في مرحلة مبكرة ولم يتم التحقق منها بعد في تجارب عشوائية كبيرة متعددة المراكز [16]. الآثار الجانبية الأكثر شيوعًا هي ألم موقع الحقن، وتورم مؤقت، وحمى خفيفة — جميعها محدودة ذاتيًا. حتى منتصف عام 2026، لم يتم الإبلاغ عن أي حالة لتكوين أورام أو نمو أنسجة منتبذة منسوبة إلى MSC في أدبيات PAD [17].
الأسئلة الشائعة
ما هي تكلفة علاج PAD بالخلايا الجذعية في تايلاند؟
في مركز فيلار، تتراوح تكلفة علاج MSC لـ PAD عادةً بين 12,000 و 18,000 دولار أمريكي، اعتمادًا على جرعة الخلايا وطريقة التوصيل وعدد الأطراف المعالجة. يشمل ذلك التقييم الوعائي قبل العلاج، وجلسة العلاج الخلوي، والمتابعة.
متى يمكن توقع التحسن بعد علاج MSC لـ PAD؟
تكوين الأوعية الدموية الجديدة وتكوين الشرايين هي عمليات بيولوجية تستغرق أسابيع إلى أشهر. تشير معظم التجارب السريرية إلى تحسن قابل للقياس في ABI ومسافة المشي يبدأ من 4-8 أسابيع بعد العلاج، مع تحسن تدريجي حتى 6 أشهر.
هل يمكن لعلاج MSC أن يحل محل جراحة المجازة أو القسطرة لـ PAD؟
لا. تبقى إعادة التوعية هي المعيار الأساسي لعلاج PAD. يُفهم علاج MSC بشكل أفضل كخيار للمرضى غير المرشحين لإعادة التوعية (CLI بدون خيار) أو كعلاج تكميلي لمعالجة مكون الأوعية الدقيقة الذي لا يمكن لإعادة التوعية وحدها إصلاحه.
المراجع
- Fowkes FGR, et al. Global PAD prevalence. Lancet. 2013;382:1329-1340. doi:10.1016/S0140-6736(13)61249-0 ↩
- Conte MS, et al. Global vascular guidelines. J Vasc Surg. 2019;69:3S-125S. doi:10.1016/j.jvs.2019.02.016 ↩
- Koutakis P, et al. Oxidative stress PAD. Physiol Rep. 2018;6:e13671. doi:10.14814/phy2.13671 ↩
- Liew A, O'Brien T. MSC for CLI. Stem Cell Res Ther. 2012;3:28. doi:10.1186/scrt119 ↩
- Kinnaird T, et al. MSC cytokines. Circ Res. 2004;94:678-685. doi:10.1161/01.RES.0000118601.37875.AC ↩
- Anderson JD, et al. MSC exosomes. Stem Cells. 2016;34:601-613. doi:10.1002/stem.2298 ↩
- Bernardo ME, Fibbe WE. MSC inflammation. Cell Stem Cell. 2013;13:392-402. doi:10.1016/j.stem.2013.09.006 ↩
- Al-Khaldi A, et al. BMSC angiogenesis. Ann Thorac Surg. 2003;75:204-209. doi:10.1016/S0003-4975(02)04273-X ↩
- Liew A, et al. CLI angiogenesis. Nat Rev Cardiol. 2013;10:387-396. doi:10.1038/nrcardio.2013.70 ↩
- Rigato M, et al. Cell therapy PAD. Circ Res. 2017;120:1326-1340. doi:10.1161/CIRCRESAHA.116.309045 ↩
- Song J, et al. PACE trial. Stem Cells. 2021;39:1425-1436. doi:10.1002/stem.3421 ↩
- Cooke JP, Losordo DW. Vascular modulation. Circ Res. 2015;116:1561-1578. doi:10.1161/CIRCRESAHA.115.303565 ↩
- Prockop DJ, et al. MSC risks. Cytotherapy. 2010;12:576-578. doi:10.3109/14653249.2010.507330 ↩