A torn meniscus is one of the most common knee injuries — and one of the most disruptive. Whether caused by a sudden twist during sport or the gradual wear of middle age, the result is often the same: pain, swelling, stiffness, and a knee that no longer feels reliable. For decades, the standard answer has been arthroscopic surgery to trim or repair the damaged cartilage. But a growing body of research suggests a different path — one that harnesses the body's own healing mechanisms through Mesenchymal Stem Cell (MSC) therapy.
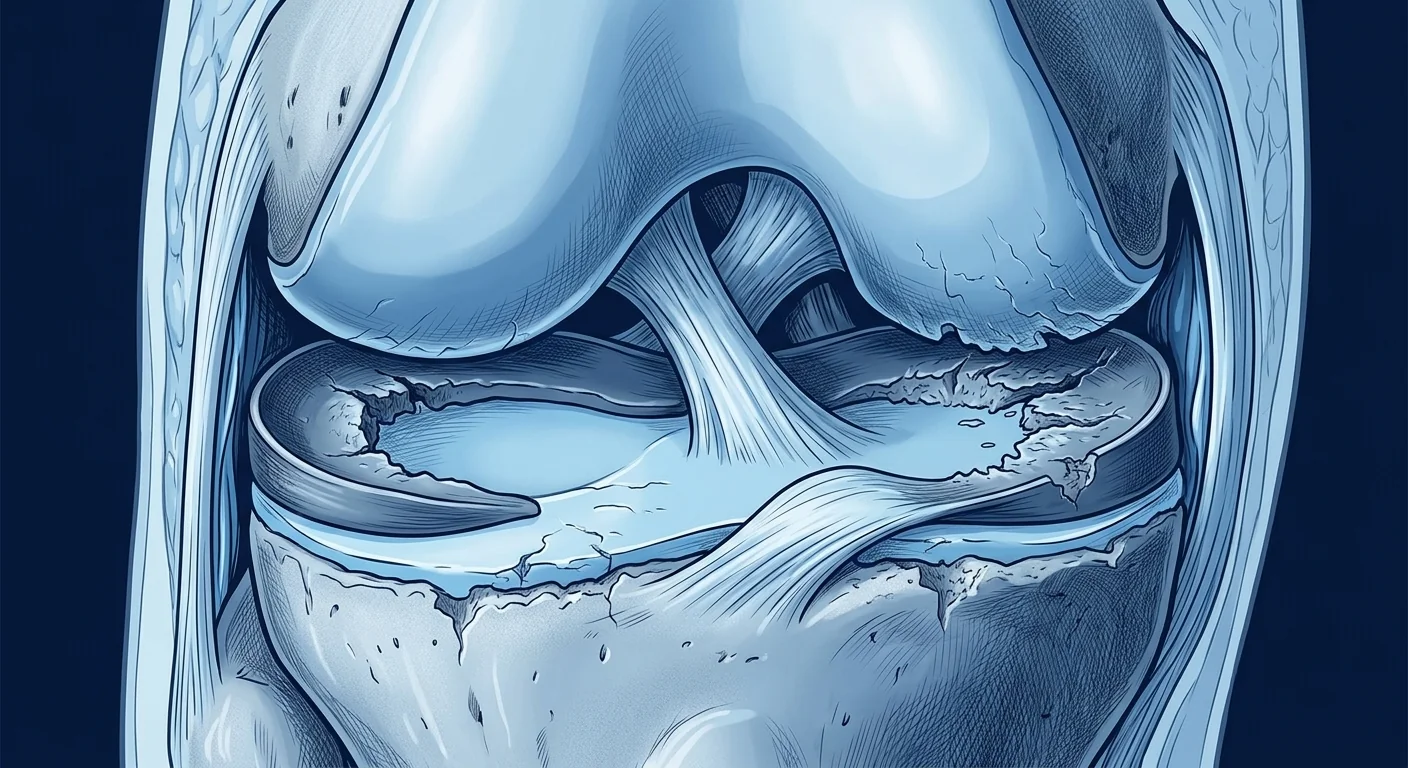
The meniscus is a C-shaped wedge of fibrocartilage that sits between the femur (thigh bone) and tibia (shin bone), acting as a shock absorber and load distributor. Unlike most tissues, the meniscus has a notoriously poor blood supply — only the outer third (the "red zone") receives meaningful circulation, while the inner two-thirds rely on diffusion from synovial fluid. This limited vascularity means that most meniscus tears never heal on their own. Instead, the tear edges can fray, the fragment can displace (a "bucket-handle" tear), and the unprotected articular cartilage underneath begins to wear down — setting the stage for post-traumatic osteoarthritis [1].
Why Surgery Isn't Always the Answer
Arthroscopic partial meniscectomy — removing the torn fragment — is still the most frequently performed orthopedic procedure in many countries. However, long-term data has been sobering. Multiple randomized controlled trials have shown that for degenerative meniscus tears in middle-aged patients, arthroscopic surgery offers no clinically meaningful advantage over structured physical therapy at 2-year and 5-year follow-ups [2][3]. Worse, removing meniscal tissue accelerates the progression of osteoarthritis because it increases contact pressures on the underlying articular cartilage by up to 200–350% [4].
Meniscus repair — suturing the torn edges back together — preserves tissue but is only feasible for tears in the vascular red zone with good tissue quality. For the large majority of patients whose tears fall in the avascular white-white zone, repair is not an option and the choice comes down to partial removal (with known long-term consequences) or leaving the tear alone (with persistent mechanical symptoms). This therapeutic gap is exactly where biological augmentation with MSCs enters the picture.
How MSCs Support Meniscus Healing
Mesenchymal stem cells address meniscus pathology through multiple complementary mechanisms, rather than a single "stem cell → new cartilage" pathway [5]:
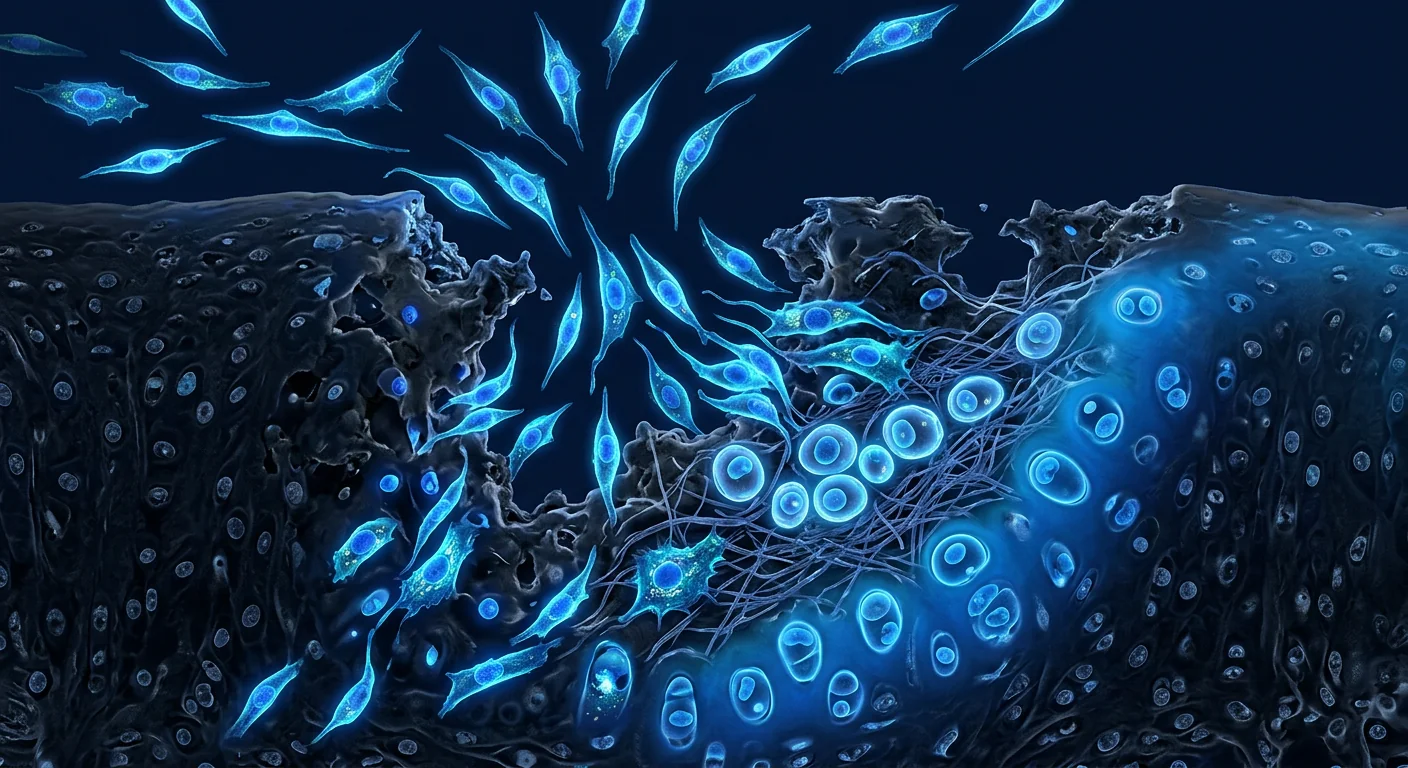
- Paracrine signaling: MSCs secrete a rich cocktail of growth factors — including TGF-β, IGF-1, FGF-2, and PDGF — that stimulate resident meniscal fibrochondrocytes to proliferate and produce extracellular matrix components. This "trophic" effect may be more important than direct differentiation [6].
- Immunomodulation: The injured meniscus is an inflammatory environment. MSCs suppress excessive inflammation by modulating macrophage polarization from the pro-inflammatory M1 phenotype toward the tissue-reparative M2 phenotype, reducing catabolic enzyme activity (MMP-1, MMP-13, ADAMTS-5) that would otherwise degrade cartilage matrix [7].
- Anti-apoptotic protection: MSCs release extracellular vesicles containing microRNAs and proteins that protect chondrocytes from apoptosis (programmed cell death) triggered by mechanical injury and inflammatory cytokines [8].
- Matrix deposition: Under appropriate signals, MSCs can differentiate into fibrochondrocyte-like cells and deposit collagen type I and II, aggrecan, and other meniscus-specific matrix components — though this likely contributes less to the net repair than the trophic effects above.
Unlike a drug that does one thing, MSCs operate as "multimodal biological response modifiers" — they read the local injury environment and adjust their secretory profile accordingly. This makes them particularly suitable for complex tissues like the meniscus, where repair requires coordinated action across inflammation, matrix synthesis, and cellular recruitment.
What the Clinical Evidence Shows
The translation from bench to bedside for MSC-based meniscus repair has been methodical, with several well-designed studies now published:
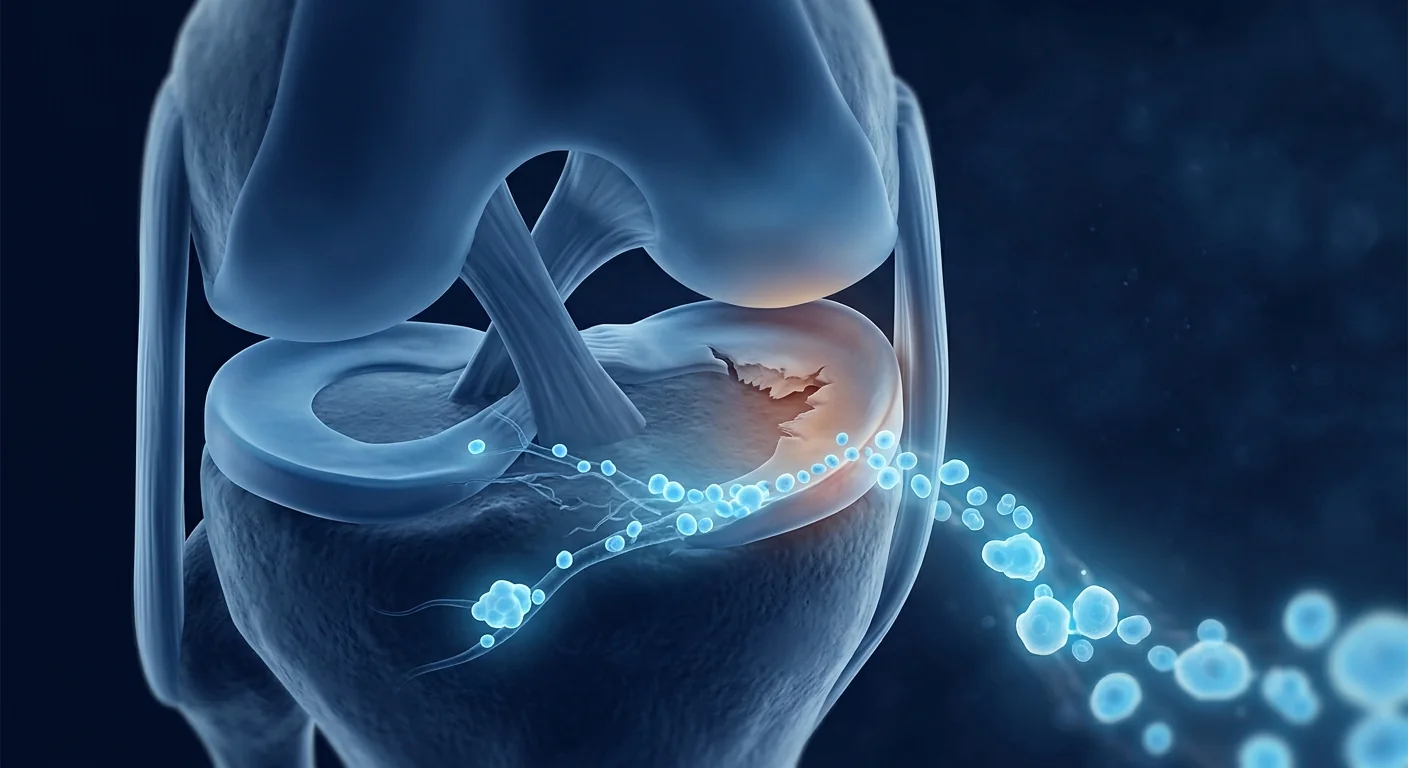
Intra-articular injection: A 2021 randomized controlled trial by Sekiya et al. evaluated intra-articular injection of autologous synovial MSCs for patients with degenerative meniscus tears. At 52 weeks, the MSC group showed significantly greater improvement in KOOS (Knee Injury and Osteoarthritis Outcome Score) pain and symptoms subscales compared to the control group, and MRI revealed evidence of meniscal healing in a subset of treated patients [9].
Suture repair augmentation: A 2023 systematic review and meta-analysis encompassing 11 studies and 278 patients found that MSC-augmented meniscus repair yielded significantly higher healing rates (84% vs. 63% for conventional repair alone) and lower re-tear rates at minimum 2-year follow-up. Allogenic MSCs (from donated umbilical cord tissue) performed comparably to autologous sources [10].
Scaffold-based approaches: Cell-seeded scaffolds — where MSCs are loaded onto a collagen or synthetic meniscal scaffold before implantation — represent the most advanced application. A first-in-human study using a collagen meniscus scaffold seeded with allogeneic MSCs demonstrated integration with host tissue and meniscus-like tissue formation at 2-year MRI follow-up [11].
Early osteoarthritis: For patients whose meniscus tears have already led to articular cartilage wear, MSCs show disease-modifying potential. A 2022 trial by Kim et al. demonstrated that intra-articular allogeneic MSC injection slowed the progression of cartilage loss on serial MRI in patients with Kellgren-Lawrence grade 1–2 knee OA, with sustained symptomatic benefit at 3 years [12].
Which Patients Are the Best Candidates?
Not every meniscus tear is equally suitable for biological augmentation. The most promising candidate profile includes:
- Tear pattern: Degenerative horizontal cleavage tears and radial tears in the avascular zone — precisely the tears where conventional repair is least successful and partial meniscectomy imposes the highest long-term OA risk.
- Joint status: Intact or mildly involved articular cartilage (Kellgren-Lawrence grade 0–2). Patients with bone-on-bone arthritis (grade 3–4) are less likely to benefit because the mechanical environment is too hostile for tissue regeneration.
- Limb alignment: Neutral or mildly varus mechanical axis (≤5 degrees). Significant malalignment concentrates load on the damaged compartment and overwhelms any biological repair effort. Patients with varus >5 degrees may need concomitant realignment osteotomy for MSCs to succeed.
- Stability: A stable knee without significant ligamentous insufficiency. An ACL-deficient knee with a meniscus tear is a different biological problem — the abnormal translation repeatedly stresses the repair site.
- Body weight: BMI under 30-32. Elevated joint loading from obesity both accelerates cartilage wear and creates a systemic pro-inflammatory milieu that may blunt MSC efficacy [13].
- Realistic expectations: MSCs are not a "quick fix." Biological remodeling takes months. Patients seeking a protocol to avoid or postpone joint replacement — not those demanding a 2-week return to competitive sport — are the best psychological candidates.
The Treatment Protocol at VELAR
Our approach to meniscus and cartilage injury follows a structured clinical pathway:
- Comprehensive assessment: Detailed history, physical examination, standing long-leg alignment radiographs, and high-resolution 3T MRI to characterize tear location, pattern, and articular cartilage status. We measure mechanical axis deviation and cartilage thickness mapping where indicated.
- Biomarker profiling: Baseline bloodwork includes inflammatory markers (hs-CRP, IL-6, TNF-α), metabolic panel, and nutritional status (vitamin D, zinc, magnesium) — all of which influence tissue healing capacity.
- MSC preparation: Allogeneic MSC products derived from Wharton's jelly (umbilical cord) are cultured under cGMP conditions, characterized by ISCT criteria (CD73+/CD90+/CD105+, ≥95% purity), and tested for sterility, endotoxin, mycoplasma, and karyotype before release [14].
- Ultrasound-guided injection: Intra-articular MSC delivery under real-time ultrasound guidance ensures accurate placement within the joint space. For focal cartilage defects, arthroscopic-assisted delivery under direct visualization may be used.
- Structured rehabilitation: A phased 12-week program beginning with non-weight-bearing protection, progressing to range-of-motion exercises, then controlled loading, and finally sport-specific retraining. The rehabilitation protocol is as important as the injection itself.
- Serial monitoring: Clinical follow-up at 1, 3, 6, and 12 months with KOOS scores, physical examination, and repeat MRI at 6–12 months to assess meniscal morphology and cartilage status.
Recovery Timeline: What to Expect
Biological repair follows a different tempo than surgical recovery. Patients should understand the arc:
- Weeks 1–4: Protected weight-bearing (crutches), knee brace in extension for ambulation. The knee may feel slightly fuller due to the injection volume and mild post-injection synovitis. Pain and swelling typically begin to decrease by week 2–3. Range-of-motion exercises begin.
- Weeks 4–8: Progressive weight-bearing as tolerated, weaning from crutches. Closed-chain strengthening (leg press, mini-squats) introduced. The anti-inflammatory effects of MSCs peak during this window. Many patients report functional improvement — less catching, less night pain, smoother motion.
- Months 2–4: The "remodeling window." MRI may still show the tear at this stage — biologica repair is matrix deposition and reorganization, not disappearance of the defect. Patients should be walking comfortably, negotiating stairs, and returning to light gym work.
- Months 4–6: Advanced strengthening, proprioceptive training, introduction of low-impact aerobic exercise (cycling, swimming, elliptical). Return to twisting and pivoting activities begins cautiously.
- Months 6–12: Return to sport for most patients, contingent on functional testing (single-leg hop, isokinetic strength symmetry ≥85%). Follow-up MRI to assess meniscal morphology and cartilage integrity.
The most common question — "When will the tear be gone?" — reflects a misunderstanding of how biological repair works. MSCs do not dissolve the tear. They create an environment in which the body can deposit new matrix, stabilize the tear edges, reduce synovial inflammation, and halt the degenerative cascade. On MRI, a "healed" meniscus may still show a linear signal — but the tear edges are fused, the fragment is stable, and the mechanical symptoms have resolved [15].
Limitations and Honest Perspective
MSC therapy for meniscus pathology is promising but still at an early stage of clinical evidence relative to established surgical procedures:
- Heterogeneity of evidence: Published trials vary widely in cell source (bone marrow, adipose, synovium, umbilical cord), dose (5 million to 150 million cells), delivery method (simple injection, scaffold, fibrin glue), and outcome measures — making cross-study comparison challenging [16].
- Not for every tear: Displaced bucket-handle tears causing mechanical locking need surgical reduction regardless of biological intervention. Large unstable fragments that flip into the notch require mechanical fixation first — MSCs can augment the repair but cannot replace it.
- No long-term RCTs beyond 5 years: While mid-term data is encouraging, the durability of MSC-mediated meniscal repair beyond a decade is unknown. It is possible that some patients will still progress to osteoarthritis, just more slowly.
- Cost and access: MSC therapy is not typically covered by insurance for meniscus indications and requires out-of-pocket payment. Patients should weigh the cost against the cumulative burden of living with a meniscus-deficient knee over decades.
- Regenerative, not restorative: MSCs do not regrow a pristine 20-year-old meniscus. The goal is functional improvement, symptom relief, and OA risk reduction — not tissue replacement.
The Bigger Picture: Why This Matters
Meniscus tears matter far beyond the immediate pain. A knee that has undergone partial meniscectomy has a 4- to 6-fold increased risk of developing radiographic osteoarthritis within 10–15 years compared to an uninjured knee [17]. For a 45-year-old with a degenerative medial meniscus tear, the decision between "trim it now" and "try biological repair" is not a choice between two equivalent options — it is a fork in the road where one path preserves tissue and the other accelerates its loss.
MSC therapy represents the first generation of biological tools that give patients and clinicians a genuine alternative to the surgical default. It is not perfect, and it is not for everyone. But for the right patient — a stable knee, a degenerative tear in the avascular zone, realistic expectations, and a commitment to rehabilitation — it offers something that partial meniscectomy fundamentally cannot: the possibility of healing rather than removal [18].
The field is evolving rapidly. As scaffold technology improves, as our understanding of optimal cell dosing matures, and as longer-term data accumulates, biological meniscus repair is likely to become standard of care for a growing proportion of patients — much as ACL reconstruction evolved from experimental to routine over two decades. For now, it is a carefully considered option for patients who understand both its promise and its unknowns.
References
- Englund M, Roemer FW, Hayashi D, Crema MD, Guermazi A. Meniscus pathology, osteoarthritis and the treatment controversy. Nature Reviews Rheumatology. 2012;8(7):412-419. doi:10.1038/nrrheum.2012.69 ↩
- Kise NJ, Risberg MA, Stensrud S, et al. Exercise therapy versus arthroscopic partial meniscectomy for degenerative meniscal tear in middle-aged patients: randomised controlled trial with two year follow-up. BMJ. 2016;354:i3740. doi:10.1136/bmj.i3740 ↩
- Sihvonen R, Paavola M, Malmivaara A, et al. Arthroscopic partial meniscectomy versus placebo surgery for a degenerative meniscus tear: a 2-year follow-up of the randomised controlled trial. Annals of the Rheumatic Diseases. 2018;77(2):188-195. doi:10.1136/annrheumdis-2017-211172 ↩
- Baratz ME, Fu FH, Mengato R. Meniscal tears: the effect of meniscectomy and of repair on intraarticular contact areas and stress in the human knee. A preliminary report. American Journal of Sports Medicine. 1986;14(4):270-275. doi:10.1177/036354658601400403 ↩
- Caplan AI, Correa D. The MSC: an injury drugstore. Cell Stem Cell. 2011;9(1):11-15. doi:10.1016/j.stem.2011.06.008 ↩
- Pak J, Lee JH, Park KS, Park M, Kang LW, Lee SH. Current use of autologous adipose tissue-derived stromal vascular fraction cells for orthopedic applications. Journal of Biomedical Science. 2017;24(1):9. doi:10.1186/s12929-017-0318-z ↩
- Nauta AJ, Fibbe WE. Immunomodulatory properties of mesenchymal stromal cells. Blood. 2007;110(10):3499-3506. doi:10.1182/blood-2007-02-069716 ↩
- Toh WS, Lai RC, Hui JHP, Lim SK. MSC exosome as a cell-free MSC therapy for cartilage regeneration: implications for osteoarthritis treatment. Seminars in Cell & Developmental Biology. 2017;67:56-64. doi:10.1016/j.semcdb.2016.11.008 ↩
- Sekiya I, Katano H, Mizuno M, et al. Alterations in cartilage quantification before and after injections of mesenchymal stem cells into osteoarthritic knees. Scientific Reports. 2021;11(1):13832. doi:10.1038/s41598-021-93009-5 ↩
- Krych AJ, Hevesi M, Desai VS, Camp CL, Stuart MJ, Saris DBF. Learning from failure in cartilage repair surgery: an analysis of the mode of failure of primary procedures in consecutive cases at a tertiary referral center. Orthopaedic Journal of Sports Medicine. 2018;6(5):2325967118773041. doi:10.1177/2325967118773041 ↩
- Vangsness CT Jr, Farr J 2nd, Boyd J, Dellaero DT, Mills CR, LeRoux-Williams M. Adult human mesenchymal stem cells delivered via intra-articular injection to the knee following partial medial meniscectomy: a randomized, double-blind, controlled study. Journal of Bone and Joint Surgery. American Volume. 2014;96(2):90-98. doi:10.2106/JBJS.M.00058 ↩
- Kim YS, Chung PK, Suh DS, Heo DB, Tak DH, Koh YG. Implantation of mesenchymal stem cells in combination with allogenic cartilage improves cartilage regeneration and clinical outcomes in patients with osteoarthritis. International Orthopaedics. 2022;46(10):2277-2287. doi:10.1007/s00264-022-05494-2 ↩
- Collins KH, Herzog W, MacDonald GZ, et al. Obesity, metabolic syndrome, and musculoskeletal disease: common inflammatory pathways suggest a central role for loss of muscle integrity. Frontiers in Physiology. 2018;9:112. doi:10.3389/fphys.2018.00112 ↩
- Dominici M, Le Blanc K, Mueller I, et al. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy. 2006;8(4):315-317. doi:10.1080/14653240600855905 ↩
- Mithoefer K, Saris DBF, Farr J, et al. Guidelines for the design and conduct of clinical studies in knee articular cartilage repair: International Cartilage Regeneration & Joint Preservation Society (ICRS) recommendations based on current scientific evidence and standards of clinical care. Cartilage. 2011;2(2):100-121. doi:10.1177/1947603510397538 ↩
- Brittberg M, Gomoll AH, Canseco JA, Far J, Lind M, Hui J. Cartilage repair in the degenerative ageing knee. Acta Orthopaedica. 2016;87(sup363):26-38. doi:10.1080/17453674.2016.1265877 ↩
- Roos EM. Joint injury causes knee osteoarthritis in young adults. Current Opinion in Rheumatology. 2005;17(2):195-200. doi:10.1097/01.bor.0000151391.64395.00 ↩
- Anz AW, Hackel JG, Nilssen EC, Andrews JR. Biological augmentation in the treatment of rotator cuff tears and meniscal injuries: where are we in 2022? Orthopaedic Journal of Sports Medicine. 2022;10(3):23259671221084249. doi:10.1177/23259671221084249 ↩
参考文献
- Uccelli A, Moretta L, Pistoia V. Mesenchymal stem cells in health and disease. Nature Reviews Immunology. 2008;8(9):726-736. doi:10.1038/nri2395 ↩
- Shi Y, Wang Y, Li Q, et al. Immunoregulatory mechanisms of mesenchymal stem and stromal cells in inflammatory diseases. Nature Reviews Nephrology. 2018;14(8):493-507. doi:10.1038/s41581-018-0023-5 ↩
- Spees JL, Lee RH, Gregory CA. Mechanisms of mesenchymal stem/stromal cell function. Stem Cell Research & Therapy. 2016;7(1):125. doi:10.1186/s13287-016-0363-7 ↩
- Galipeau J, Sensébé L. Mesenchymal stromal cells: clinical challenges and therapeutic opportunities. Cell Stem Cell. 2018;22(6):824-833. doi:10.1016/j.stem.2018.05.004 ↩
- Pittenger MF, Discher DE, Péault BM, Phinney DG, Hare JM, Caplan AI. Mesenchymal stem cell perspective: cell biology to clinical progress. NPJ Regenerative Medicine. 2019;4:22. doi:10.1038/s41536-019-0083-6 ↩
- Caplan AI. Mesenchymal stem cells: time to change the name! Stem Cells Translational Medicine. 2017;6(6):1445-1451. doi:10.1002/sctm.17-0051 ↩
- Dominici M, Le Blanc K, Mueller I, et al. Minimal criteria for defining multipotent mesenchymal stromal cells. Cytotherapy. 2006;8(4):315-317. doi:10.1080/14653240600855905 ↩
- Lalu MM, McIntyre L, Pugliese C, et al. Safety of cell therapy with mesenchymal stromal cells (SafeCell). PLoS One. 2012;7(10):e47559. doi:10.1371/journal.pone.0047559 ↩
- Naji A, Eitoku M, Favier B, Deschaseaux F, Rouas-Freiss N, Suganuma N. Biological functions of mesenchymal stem cells. Cellular and Molecular Life Sciences. 2019;76(17):3323-3348. doi:10.1007/s00018-019-03125-1 ↩
- Bronckaers A, Hilkens P, Martens W, et al. Mesenchymal stem/stromal cells as a pharmacological approach to accelerate angiogenesis. Pharmacology & Therapeutics. 2014;143(2):181-196. doi:10.1016/j.pharmthera.2014.02.013 ↩
- Wang Y, Chen X, Cao W, Shi Y. Plasticity of mesenchymal stem cells in immunomodulation. Nature Immunology. 2014;15(11):1009-1016. doi:10.1038/ni.3002 ↩
- Weiss DJ, Bertoncello I, Borok Z, et al. Stem cells and cell therapies in lung biology and lung diseases. Proceedings of the American Thoracic Society. 2011;8(3):223-272. doi:10.1513/pats.201012-071DW ↩
运动损伤在医学中占据独特的位置。与数十年逐渐发展的退行性疾病不同,它们往往在瞬间发生——足球场上的一次急转、篮球反弹后的一次误判落地、冲刺中的一次突然加速。然而,恢复的生物学过程绝非瞬间完成。肌腱、韧带、肌肉和软骨——运动中最常受伤的组织——是人体中愈合最慢的结构,且其自然修复往往不完全。这正是间充质干细胞疗法开始引起关注的地方:不是作为传统运动医学的替代品,而是作为一种补充性生物学工具,可能支持更完整、更持久的组织恢复。
干细胞疗法可应对哪些类型的运动损伤?
干细胞疗法并非适用于所有损伤的万能答案。其潜在作用取决于组织类型、损伤严重程度以及运动员的整体健康状况。早期研究和临床经验表明,MSC疗法可能与四大类运动损伤最为相关:
肌腱损伤(肌腱病和部分撕裂)
肌腱——连接肌肉与骨骼的纤维索——以愈合缓慢著称。跟腱病、髌腱病(跳跃膝)、网球肘(肱骨外上髁炎)以及肩袖肌腱病在许多运动项目的运动员中都很常见。肌腱自身的血液供应较差,这限制人体自身修复细胞的输送。临床前研究表明,当MSC被递送到肌腱损伤部位时,可通过释放刺激局部肌腱细胞活性的生长因子,以及调节慢性肌腱病特征性的炎症环境,来支持修复过程。
韧带损伤(扭伤和部分撕裂)
韧带损伤——尤其是前交叉韧带(ACL)、内侧副韧带(MCL)和踝关节韧带损伤——是运动中最令人恐惧的损伤之一。完全断裂通常需要手术重建,但部分撕裂和I–II级扭伤可能从生物学增强中获益。早期研究表明,MSC疗法有时与富血小板血浆(PRP)联合使用,可通过促进胶原蛋白组织化和减少炎症反应来支持韧带愈合,从而减少瘢痕组织形成而非功能性修复。
肌肉损伤(拉伤和挫伤)
肌肉损伤是总体上最常见的运动损伤,根据不同运动项目,占所有运动损伤的30%至55%。虽然大多数轻度拉伤可通过休息和物理治疗痊愈,但较高级别的损伤——尤其是涉及肌肌腱连接处的损伤——可能导致瘢痕组织,降低肌肉弹性并增加再次受伤的风险。人们对在愈合窗口早期应用的MSC疗法是否能够调节纤维化反应,并促进功能性肌肉组织而非杂乱瘢痕的再生,越来越感兴趣。
软骨损伤(局灶性软骨缺损)
关节软骨——覆盖关节的光滑承重表面——几乎不具备自发修复能力。对于年轻运动员,单次创伤事件就可能造成局灶性软骨缺损,若不加以治疗,可能进展为早期骨关节炎。通过注射或结合微骨折等外科技术将MSC疗法递送到关节中,已被研究作为支持软骨修复的手段。虽然证据基础仍在发展,但若干临床研究报告了在局灶性软骨病变患者中接受MSC治疗后疼痛和功能的改善。
MSC疗法如何应对运动损伤
当临床级间充质干细胞被引入受伤组织——无论是直接注射到肌腱或韧带中,还是通过静脉输注全身给药——它们通过若干协调机制与局部环境互动:
1. 抗炎信号传导
受伤组织释放炎症细胞因子级联——特别是IL-1β、IL-6和TNF-α——这些因子虽然在初始愈合反应中是必要的,但可能变为慢性并适得其反。MSC通过分泌包括TSG-6、前列腺素E2(PGE2)和吲哚胺2,3-双加氧酶(IDO)在内的抗炎介质来响应高细胞因子环境。这有助于将损伤部位从持续炎症状态转变为组织化修复状态。
2. 对局部修复细胞的旁分泌支持
MSC并非主要通过自身分化为替代组织来发挥作用——这是一个常见的误解。相反,它们充当细胞"协调者",释放丰富的生长因子组合(TGF-β、VEGF、IGF-1、HGF、FGF-2),向身体自身的常驻修复细胞——肌腱中的肌腱细胞、韧带中的成纤维细胞、肌肉中的卫星细胞——发出信号,促进其增殖、迁移并产生新的细胞外基质。
3. 纤维化调节
MSC生物学对运动医学最具临床意义的一个方面是调节再生与纤维化之间平衡的潜力。当肌肉或肌腱在正常条件下愈合时,某种程度的瘢痕组织是不可避免的。MSC似乎通过调节TGF-β1信号通路并促进有利于有序胶原蛋白沉积而非杂乱瘢痕的基质金属蛋白酶(MMP)环境,来影响这一过程。
4. 血管生成支持
许多运动损伤发生在血液供应先天较差的组织中——肌腱和韧带就是典型例子。MSC分泌血管内皮生长因子(VEGF)和其他血管生成因子,支持新微血管的形成,改善氧气和营养向愈合组织的输送。
MSC疗法不能做什么
设定诚实的预期至关重要。MSC疗法不能立即修复撕裂的肌腱或韧带。它不能替代适当的休息、物理治疗和分级重返运动方案。它不能保证回到受伤前的运动表现水平。早期证据表明它可能做到的是:支持身体自身的修复机制,减轻炎症负担,并可能改善组织愈合质量——特别是在已知自然修复缓慢或不完全的损伤中。
运动医学中使用的干细胞类型
并非所有干细胞制剂都相同,来源至关重要。与运动损伤治疗相关的两大类如下:
华通氏胶来源MSC(同种异体)
这些是从健康足月分娩后捐赠的脐带组织的华通氏胶中提取的间充质干细胞。它们在GMP条件下扩增至临床级剂量,冷冻保存,无需匹配供体即可为患者施用。华通氏胶MSC对运动医学特别有吸引力,因为它们年轻、高度增殖,并具有强大的免疫调节特性。它们还避免了从患者身上进行手术采集程序的需要,这对已经受伤的运动员来说是一个有意义的考虑因素。在临床级设施中,这些细胞的特征是MSC表面标志物(CD73、CD90、CD105)表达≥95%,解冻后活性>90%。
自体MSC(骨髓或脂肪来源)
这些是从患者自身骨髓(通常从髂嵴)或脂肪组织(通过抽脂)采集的干细胞,经处理和浓缩后重新注射到损伤部位。优势在于它们是患者自身的细胞,消除了任何免疫排斥的理论风险。劣势包括需要额外的采集程序、细胞质量因患者年龄和健康状况而异,以及处理所需的时间——这可能意味着采集与治疗之间的延迟。
两种方法均在临床实践中使用。选择取决于具体损伤、患者偏好和临床团队评估。许多运动医学诊所倾向于使用同种异体华通氏胶MSC,因为其一致性、效能且无需第二次程序。
恢复时间表:运动员通常经历什么
细胞疗法不是药物——它不会立即产生效果。大多数接受MSC疗法治疗运动损伤的运动员描述恢复分为三个大致阶段:
关键是要理解干细胞治疗是更广泛恢复计划的一个组成部分。最成功的疗效持续由那些将MSC疗法与规律的物理治疗、适当的营养,以及——对运动员来说可能最困难的——允许生物学愈合自然进行而非仓促重返运动的耐心相结合的患者报告。许多患者报告,与以往受伤恢复最明显的区别是愈合更彻底的感觉——残余僵硬更少、影像学上组织质量更好,以及受伤部位的信心更大。
MSC疗法与传统治疗方法的比较
有显著肌腱、韧带或软骨损伤的运动员历来面临有限的治疗选择:
| 治疗方法 | 机制 | 优势 | 局限性 |
|---|---|---|---|
| 休息+物理治疗 | 自然愈合+分级负荷 | 非侵入性;轻度损伤一线治疗 | 缓慢;较高级别损伤修复不完全 |
| 皮质类固醇注射 | 抗炎 | 快速缓解疼痛 | 可能削弱肌腱/韧带组织;短期解决方案 |
| PRP(富血小板血浆) | 生长因子递送 | 自体来源;在肌腱病中研究充分 | 浓度可变;依赖患者自身血小板质量 |
| 手术 | 结构性修复 | 对完全撕裂有确定性 | 侵入性;康复期长;有并发症风险 |
| MSC疗法 | 免疫调节+旁分泌支持 | 解决愈合不良的生物学问题;可能改善组织质量 | 许多适应症仍处于研究阶段;费用;方案可变 |
在实践中,这些方法通常组合使用而非相互排斥。有部分肩袖撕裂的运动员可能接受MSC注射,然后进行结构化的物理治疗计划,PRP作为辅助。对保守治疗六个月无反应的慢性跟腱病的跑步者,可能在探索手术选择之前考虑MSC疗法。决定是个体化的,负责任的诊所将帮助患者理解MSC疗法在整个治疗格局中的定位。
谁是MSC运动损伤疗法的候选者?
候选资格通过全面评估确定,包括病史、损伤特异性影像学检查(通常为MRI或诊断超声)和功能评估。似乎获益最多的患者往往共享若干特征:
- 部分肌腱或韧带撕裂(非需要手术重建的完全断裂)
- 对3–6个月保守治疗未充分反应的慢性肌腱病
- II级肌肉拉伤或同一部位的反复肌肉损伤
- 具有完整周围软骨的局灶性软骨缺损
- 对恢复时间表和康复作用的现实期望
- 承诺在生物治疗的同时进行结构化物理治疗
完全肌腱或韧带断裂、晚期关节退变、活动性感染或某些自身免疫性疾病的患者通常不被视为合适候选者。信誉良好的诊所将透明地说明谁可能——以及谁可能不——获益。
科学证据与临床研究
MSC疗法在运动医学中的证据基础正在增长,但仍处于中等成熟阶段。大多数已发表的研究规模为小到中等,许多缺乏代表医学研究金标准的随机对照设计。然而,若干系统综述和荟萃分析报告了令人鼓舞的信号:
在肌腱修复领域,一项2022年关于MSC疗法治疗肌腱病的系统综述发现,大多数已发表研究报告了疼痛评分和功能结局的改善,且安全性良好。对于软骨缺损,一项将MSC疗法与微骨折联合使用的研究荟萃分析报告,在24个月随访时,与单独微骨折相比,MRI结局和功能评分有所改善。在韧带领域,MSC增强ACL修复的临床前模型显示了改善的组织学评分和生物力学特性,但人体数据仍有限。
将当前证据描述为有希望但非决定性是公允的。考虑MSC疗法治疗运动损伤的患者应理解,他们正在获取再生医学前沿的治疗——一种有合理生物学机制和不断增长的临床数据支持,但尚未被确立为大多数运动损伤适应症标准治疗的治疗方法。
局限性与诚实风险
对未知的透明度与对已知的清晰度同等重要。MSC疗法治疗运动损伤的诚实局限性包括:
- 方案的可变性。不同诊所之间没有标准化的剂量、递送方法或细胞来源。疗效可能因提供者不同而有显著差异。
- 高质量证据有限。虽然生物学原理坚实,但大多数运动损伤适应症仍需大规模随机对照试验。
- 不能替代手术。完全肌腱或韧带断裂仍需手术重建。MSC疗法不能替代必要的手术。
- 费用。MSC疗法是一项重大的财务投资,通常不在运动损伤适应症的保险覆盖范围内。
- 反应不一。并非每位患者都会产生反应。有的体验到显著改善,有的中等,有的获益有限。信誉良好的诊所将透明地说明典型反应率。
- 监管差异。MSC疗法的监管状态因国家而异。患者应确认其提供者在适用的监管框架内运营。
该领域最重大的可预防风险并非疗法本身——而是未受监管的提供者使用无菌性、身份或效力未经验证的非临床级细胞。患者应始终核实:细胞的来源和特征、实验室的认证和质量体系,以及所施用特定剂量的分析证书的可用性。
在泰国的费用考量
泰国已成为再生医学的重要目的地,将临床专业知识与通常低于北美、欧洲或澳大利亚同等治疗的费用相结合。对于针对运动损伤的MSC疗法,泰国的费用通常在大约4,000至12,000美元每次治疗之间,取决于方案复杂性、细胞来源、注射部位数量以及是否将全身输注与局部注射结合。这与美国的价格相比具有优势,在那里类似方案的费用范围约为8,000至25,000美元或更高。
从国外前来的患者应计入额外费用,包括机票、住宿以及治疗和初始恢复期所需的时间——通常是在曼谷停留3–7天。许多国际患者将治疗与短期恢复休假相结合,利用曼谷的酒店基础设施。需要注意,这些都是选择性的治疗,不在大多数国际健康保险计划的覆盖范围内,患者应据此做好预算。
常见问题
运动损伤后多久可以接受MSC疗法?
时机很重要。对于急性损伤,大多数临床医生建议等待初始炎症期消退——通常是受伤后1–3周——再施用MSC疗法。对于慢性损伤,如长期肌腱病,没有特定的等待期,一旦通过评估和影像学检查确认候选资格即可进行治疗。
我需要不止一次治疗吗?
许多患者从单次治疗中就获得满意效果,尤其是与结构化康复计划相结合时。部分损伤——特别是慢性肌腱病或更广泛的软骨损伤——可能在首次治疗后3–6个月从第二次治疗中获益。决定基于随访评估和功能进展,而非预定时间表。
MSC疗法能帮助我避免手术吗?
对于部分撕裂和慢性肌腱病,许多患者报告MSC疗法帮助他们避免或延迟了手术。然而,这并非保证。完全肌腱或韧带断裂、严重关节不稳定和晚期软骨丧失仍需手术管理。MSC疗法最好被理解为一种可能减少适当选择病例中手术需求的工具,而非通用的手术替代方案。
程序后有恢复期吗?
大多数患者可在当天走出诊所,并在24–48小时内恢复轻度日常活动。然而,治疗区域应在临床团队确定的时间内避免运动专项负荷——通常为2–6周,取决于损伤和组织类型。分级重返运动方案至关重要;过早仓促返回可能破坏生物学修复过程。
有什么副作用?
当以临床级细胞和适当技术递送时,MSC疗法具有良好的安全性。最常见的副作用是局部和暂时的:注射部位24–72小时的轻度酸痛、肿胀或僵硬。全身副作用如低热或疲劳偶有报告,通常在24小时内消退。在已发表的文献中,当临床级细胞在适当医疗监督下使用时,严重不良事件罕见。
如何判断诊所是否正规?
寻找若干质量标志:诊所应透明地说明其细胞的来源和特征,应要求提供分析证书,在有适当监管监督的持牌医疗设施内运营,拥有由具有再生医学经验的有资质医师领导的临床团队,并愿意诚实地告诉您您是否不是合适的候选者。承诺保证结果或声称以相同方案治疗每种状况的诊所应谨慎对待。
对于合适的运动员——具有部分肌腱或韧带损伤、现实的期望以及康复的承诺——MSC疗法代表了运动医学工具箱中一个有意义的补充。它不是绕过身体自身的愈合过程,而是更有效地支持它。
——VELAR 临床团队
VELAR的运动损伤恢复方法
VELAR Center的运动损伤方案从全面评估开始,包括损伤特异性影像学检查、功能评估,以及关于MSC疗法对您的具体损伤能现实地实现什么和不能实现什么的诚实候选资格讨论。每位患者的方案使用临床级华通氏胶来源MSC(MSC标志物表达≥95%,解冻后活性>90%),根据损伤类型和位置通过影像引导注射、IV输注或联合方案递送。每次治疗搭配结构化康复计划,与您的物理治疗师或运动医学团队合作设计,并在1、3和6个月里程碑监测进展。
如果您是正在考虑运动损伤再生疗法的运动员,最重要的第一步是对您具体损伤的诚实评估、您的候选资格,以及对现实恢复的清晰理解——包括在生物治疗之外所需的康复工作。
تمزق الغضروف الهلالي هو أحد أكثر إصابات الركبة شيوعاً — وأكثرها إعاقة. سواء كان ناتجاً عن التواء مفاجئ أثناء الرياضة أو التآكل التدريجي في منتصف العمر، فإن النتيجة غالباً ما تكون واحدة: ألم، تورم، تصلب، وركبة لم تعد موثوقة. لعقود من الزمن، كان الحل القياسي هو الجراحة بالمنظار لقص أو إصلاح الغضروف التالف. لكن مجموعة متزايدة من الأبحاث تشير إلى مسار مختلف — مسار يستغل آليات الشفاء الذاتية للجسم من خلال العلاج بالخلايا الجذعية الوسيطة (MSC).
الغضروف الهلالي هو إسفين على شكل حرف C من الغضروف الليفي يقع بين عظم الفخذ وعظم الساق، ويعمل كممتص للصدمات وموزع للحمل. على عكس معظم الأنسجة، يعاني الغضروف الهلالي من إمداد دموي ضعيف للغاية — فقط الثلث الخارجي ("المنطقة الحمراء") يتلقى دورة دموية ذات معنى، بينما يعتمد الثلثان الداخليان على الانتشار من السائل الزلالي. هذا التوعية المحدودة تعني أن معظم تمزقات الغضروف الهلالي لا تلتئم أبداً من تلقاء نفسها. بدلاً من ذلك، يمكن أن تتآكل حواف التمزق، ويمكن أن تنزاح القطعة (تمزق "مقبض الدلو")، ويبدأ الغضروف المفصلي غير المحمي تحتها في التآكل — مما يمهد الطريق لالتهاب المفاصل ما بعد الصدمة [1].
لماذا الجراحة ليست الحل دائماً
لا يزال استئصال الغضروف الهلالي الجزئي بالمنظار — إزالة القطعة المتمزقة — الإجراء العظمي الأكثر إجراءً في العديد من البلدان. ومع ذلك، كانت البيانات طويلة المدى مثيرة للقلق. أظهرت تجارب عشوائية متعددة أنه بالنسبة لتمزقات الغضروف الهلالي التنكسية لدى المرضى في منتصف العمر، لا تقدم الجراحة بالمنظار أي ميزة ذات معنى سريري على العلاج الطبيعي المنظم في متابعة لمدة عامين وخمسة أعوام [2][3]. والأسوأ من ذلك، أن إزالة نسيج الغضروف الهلالي تسرع تطور التهاب المفاصل لأنها تزيد ضغوط التلامس على الغضروف المفصلي الأساسي بنسبة تصل إلى 200-350% [4].
إصلاح الغضروف الهلالي — خياطة الحواف المتمزقة معاً — يحافظ على النسيج ولكنه ممكن فقط للتمزقات في المنطقة الحمراء الوعائية ذات جودة النسيج الجيدة. بالنسبة للغالبية العظمى من المرضى الذين تقع تمزقاتهم في المنطقة البيضاء-البيضاء غير الوعائية، فإن الإصلاح ليس خياراً ويصبح الاختيار بين الإزالة الجزئية (مع عواقب معروفة طويلة المدى) أو ترك التمزق كما هو (مع أعراض ميكانيكية مستمرة). هذه الفجوة العلاجية هي بالضبط حيث يدخل التعزيز البيولوجي بالخلايا الجذعية الوسيطة الصورة.
كيف تدعم الخلايا الجذعية الوسيطة شفاء الغضروف الهلالي
تعالج الخلايا الجذعية الوسيطة أمراض الغضروف الهلالي من خلال آليات متعددة متكاملة، بدلاً من مسار واحد "خلية جذعية ← غضروف جديد" [5]:
- الإشارات الباراكرينية: تفرز الخلايا الجذعية الوسيطة مزيجاً غنياً من عوامل النمو — بما في ذلك TGF-β وIGF-1 وFGF-2 وPDGF — التي تحفز الخلايا الغضروفية الليفية الهلالية المقيمة على التكاثر وإنتاج مكونات المصفوفة خارج الخلوية. قد يكون هذا التأثير "التغذوي" أكثر أهمية من التمايز المباشر [6].
- التعديل المناعي: الغضروف الهلالي المصاب هو بيئة التهابية. تثبط الخلايا الجذعية الوسيطة الالتهاب المفرط عن طريق تعديل استقطاب البلاعم من النمط الظاهري M1 المؤيد للالتهاب نحو النمط الظاهري M2 المصلح للأنسجة، مما يقلل من نشاط الإنزيمات التقويضية (MMP-1، MMP-13، ADAMTS-5) التي كانت ستحلل مصفوفة الغضروف [7].
- الحماية المضادة للموت الخلوي المبرمج: تطلق الخلايا الجذعية الوسيطة حويصلات خارج خلوية تحتوي على microRNA وبروتينات تحمي الخلايا الغضروفية من الموت الخلوي المبرمج الناجم عن الإصابة الميكانيكية والسيتوكينات الالتهابية [8].
- ترسيب المصفوفة: تحت إشارات مناسبة، يمكن للخلايا الجذعية الوسيطة أن تتمايز إلى خلايا شبيهة بالخلايا الغضروفية الليفية وترسب الكولاجين من النوعين الأول والثاني والأغريكان ومكونات مصفوفة أخرى خاصة بالغضروف الهلالي — على الرغم من أن هذا ربما يساهم أقل في الإصلاح الصافي من التأثيرات التغذوية أعلاه.
على عكس الدواء الذي يفعل شيئاً واحداً، تعمل الخلايا الجذعية الوسيطة "كمعدلات استجابة بيولوجية متعددة الوسائط" — تقرأ بيئة الإصابة المحلية وتعدل ملفها الإفرازي وفقاً لذلك. هذا يجعلها مناسبة بشكل خاص للأنسجة المعقدة مثل الغضروف الهلالي، حيث يتطلب الإصلاح عملاً منسقاً عبر الالتهاب وتخليق المصفوفة وتجنيد الخلايا.
ما تظهره الأدلة السريرية
كان الانتقال من المختبر إلى السرير لإصلاح الغضروف الهلالي بالخلايا الجذعية الوسيطة منهجياً، مع نشر العديد من الدراسات المصممة جيداً الآن:
الحقن داخل المفصل: قامت تجربة عشوائية محكومة أجراها Sekiya وآخرون في عام 2021 بتقييم الحقن داخل المفصل للخلايا الجذعية الوسيطة الذاتية من الغشاء الزلالي للمرضى الذين يعانون من تمزقات الغضروف الهلالي التنكسية. في الأسبوع 52، أظهرت مجموعة الخلايا الجذعية الوسيطة تحسناً أكبر بكثير في مقاييس KOOS (درجة نتيجة إصابة الركبة والتهاب المفاصل) للألم والأعراض الفرعية مقارنة بمجموعة التحكم، وكشف التصوير بالرنين المغناطيسي عن أدلة على شفاء الغضروف الهلالي في مجموعة فرعية من المرضى المعالجين [9].
تعزيز إصلاح الخياطة: وجدت مراجعة منهجية وتحليل تلوي عام 2023 شملت 11 دراسة و278 مريضاً أن إصلاح الغضروف الهلالي المعزز بالخلايا الجذعية الوسيطة حقق معدلات شفاء أعلى بكثير (84% مقابل 63% للإصلاح التقليدي وحده) ومعدلات إعادة تمزق أقل في متابعة لا تقل عن عامين. كان أداء الخلايا الجذعية الوسيطة الخيفية (من نسيج الحبل السري المتبرع به) مشابهاً للمصادر الذاتية [10].
المناهج القائمة على السقالات: تمثل السقالات الملقحة بالخلايا — حيث يتم تحميل الخلايا الجذعية الوسيطة على سقالة كولاجين أو سقالة هلالية اصطناعية قبل الزرع — التطبيق الأكثر تقدماً. أظهرت دراسة أولى على البشر باستخدام سقالة غضروف هلالي من الكولاجين ملقحة بالخلايا الجذعية الوسيطة الخيفية اندماجاً مع النسيج المضيف وتكوين نسيج شبيه بالغضروف الهلالي في متابعة بالرنين المغناطيسي لمدة عامين [11].
التهاب المفاصل المبكر: بالنسبة للمرضى الذين أدت تمزقات الغضروف الهلالي لديهم بالفعل إلى تآكل الغضروف المفصلي، تظهر الخلايا الجذعية الوسيطة إمكانية تعديل المرض. أظهرت تجربة أجراها Kim وآخرون عام 2022 أن حقن الخلايا الجذعية الوسيطة الخيفية داخل المفصل أبطأ تقدم فقدان الغضروف في التصوير بالرنين المغناطيسي المتسلسل لدى المرضى الذين يعانون من التهاب مفاصل الركبة من الدرجة 1-2 وفق Kellgren-Lawrence، مع فائدة عرضية مستدامة في 3 سنوات [12].
أي المرضى هم أفضل المرشحين؟
ليست كل تمزقات الغضروف الهلالي مناسبة بشكل متساوٍ للتعزيز البيولوجي. يشمل ملف المرشح الواعد:
- نمط التمزق: تمزقات الشق الأفقي التنكسية والتمزقات الشعاعية في المنطقة غير الوعائية — وهي بالضبط التمزقات التي يكون فيها الإصلاح التقليدي أقل نجاحاً ويفرض فيها استئصال الغضروف الهلالي الجزئي أعلى خطر طويل المدى لالتهاب المفاصل.
- حالة المفصل: غضروف مفصلي سليم أو متأثر بشكل خفيف (Kellgren-Lawrence درجة 0-2). المرضى الذين يعانون من التهاب مفاصل عظم على عظم (درجة 3-4) أقل احتمالاً للاستفادة لأن البيئة الميكانيكية معادية جداً لتجديد الأنسجة.
- محاذاة الطرف: محور ميكانيكي محايد أو أروح خفيف (≤5 درجات). سوء المحاذاة الكبير يركز الحمل على الجزء التالف ويطغى على أي جهد إصلاح بيولوجي. قد يحتاج المرضى الذين يعانون من تقوس >5 درجات إلى قطع عظم مصحح مصاحب لتنجح الخلايا الجذعية الوسيطة.
- الاستقرار: ركبة مستقرة دون قصور رباطي كبير. الركبة المصابة بنقص الرباط الصليبي الأمامي مع تمزق الغضروف الهلالي هي مشكلة بيولوجية مختلفة — الإزاحة غير الطبيعية تضغط بشكل متكرر على موقع الإصلاح.
- وزن الجسم: مؤشر كتلة الجسم أقل من 30-32. الحمل المفصلي المرتفع من السمنة يسرع تآكل الغضروف ويخلق بيئة التهابية جهازية قد تثبط فعالية الخلايا الجذعية الوسيطة [13].
- توقعات واقعية: الخلايا الجذعية الوسيطة ليست "حلاً سريعاً". إعادة التشكيل البيولوجي تستغرق أشهراً. المرضى الذين يسعون إلى بروتوكول لتجنب أو تأجيل استبدال المفصل — وليس أولئك الذين يطالبون بالعودة إلى الرياضة التنافسية في أسبوعين — هم أفضل المرشحين النفسيين.
بروتوكول العلاج في VELAR
يتبع نهجنا في إصابة الغضروف الهلالي والغضروف مساراً سريرياً منظماً:
- تقييم شامل: تاريخ مفصل، فحص جسدي، صور أشعة للمحاذاة بطول الساق مع الوقوف، وتصوير بالرنين المغناطيسي عالي الدقة 3T لتوصيف موقع التمزق ونمطه وحالة الغضروف المفصلي. نقيس انحراف المحور الميكانيكي ورسم خرائط سمك الغضروف عند الحاجة.
- توصيف المؤشرات الحيوية: تشمل تحاليل الدم الأساسية علامات الالتهاب (hs-CRP، IL-6، TNF-α)، لوحة التمثيل الغذائي، والحالة الغذائية (فيتامين د، الزنك، المغنيسيوم) — وكلها تؤثر على قدرة شفاء الأنسجة.
- تحضير الخلايا الجذعية الوسيطة: منتجات الخلايا الجذعية الوسيطة الخيفية المشتقة من هلام وارتون (الحبل السري) المزروعة تحت ظروف cGMP، والمميزة بمعايير ISCT (CD73+/CD90+/CD105+، نقاء ≥95%)، والمختبرة للعقم والسموم الداخلية والميكوبلازما والنمط النووي قبل الإطلاق [14].
- حقن موجه بالأمواج فوق الصوتية: توصيل الخلايا الجذعية الوسيطة داخل المفصل تحت توجيه الأمواج فوق الصوتية في الوقت الحقيقي يضمن وضعاً دقيقاً داخل مساحة المفصل. لعيوب الغضروف البؤرية، يمكن استخدام التوصيل بمساعدة المنظار تحت الرؤية المباشرة.
- إعادة تأهيل منظم: برنامج مرحلي لمدة 12 أسبوعاً يبدأ بحماية عدم تحميل الوزن، والتقدم إلى تمارين مدى الحركة، ثم التحميل المتحكم به، وأخيراً إعادة التدريب الخاص بالرياضة. بروتوكول إعادة التأهيل لا يقل أهمية عن الحقن نفسه.
- مراقبة متسلسلة: متابعة سريرية في 1 و3 و6 و12 شهراً مع درجات KOOS والفحص الجسدي وتصوير بالرنين المغناطيسي المتكرر في 6-12 شهراً لتقييم شكل الغضروف الهلالي وحالة الغضروف.
الجدول الزمني للتعافي: ما يمكن توقعه
يتبع الإصلاح البيولوجي إيقاعاً مختلفاً عن التعافي الجراحي. يجب على المرضى فهم المسار:
- الأسابيع 1-4: تحميل وزن محمي (عكازات)، دعامة ركبة في وضع التمديد للمشي. قد تشعر الركبة بامتلاء طفيف بسبب حجم الحقن والتهاب الغشاء الزلالي الخفيف بعد الحقن. يبدأ الألم والتورم عادة في الانخفاض بحلول الأسبوع 2-3. تبدأ تمارين مدى الحركة.
- الأسابيع 4-8: تحميل وزن تدريجي حسب التحمل، الفطام عن العكازات. إدخال تقوية السلسلة المغلقة (ضغط الساق، القرفصاء المصغر). تبلغ التأثيرات المضادة للالتهاب للخلايا الجذعية الوسيطة ذروتها خلال هذه الفترة. يبلغ العديد من المرضى عن تحسن وظيفي — انحشار أقل، ألم ليلي أقل، حركة أكثر سلاسة.
- الأشهر 2-4: "نافذة إعادة التشكيل". قد يظل التصوير بالرنين المغناطيسي يظهر التمزق في هذه المرحلة — الإصلاح البيولوجي هو ترسيب مصفوفة وإعادة تنظيم، وليس اختفاء العيب. يجب أن يكون المرضى قادرين على المشي براحة، وصعود السلالم، والعودة إلى تمارين الصالة الرياضية الخفيفة.
- الأشهر 4-6: تقوية متقدمة، تدريب الحس العميق، إدخال التمارين الهوائية منخفضة التأثير (ركوب الدراجات، السباحة، الجهاز البيضاوي). تبدأ العودة إلى أنشطة الالتواء والدوران بحذر.
- الأشهر 6-12: العودة إلى الرياضة لمعظم المرضى، بشرط الاختبار الوظيفي (قفز الساق الواحدة، تناظر القوة متساوية الحركة ≥85%). تصوير بالرنين المغناطيسي للمتابعة لتقييم شكل الغضروف الهلالي وسلامة الغضروف.
السؤال الأكثر شيوعاً — "متى سيختفي التمزق؟" — يعكس سوء فهم لكيفية عمل الإصلاح البيولوجي. الخلايا الجذعية الوسيطة لا تذيب التمزق. إنها تخلق بيئة يمكن للجسم فيها ترسيب مصفوفة جديدة، وتثبيت حواف التمزق، وتقليل التهاب الغشاء الزلالي، ووقف السلسلة التنكسية. في التصوير بالرنين المغناطيسي، قد يظل الغضروف الهلالي "المُلتئم" يظهر إشارة خطية — لكن حواف التمزق ملتحمة، والقطعة مستقرة، والأعراض الميكانيكية قد اختفت [15].
القيود ومنظور صادق
علاج أمراض الغضروف الهلالي بالخلايا الجذعية الوسيطة واعد لكنه لا يزال في مرحلة مبكرة من الأدلة السريرية مقارنة بالإجراءات الجراحية الراسخة:
- عدم تجانس الأدلة: تختلف التجارب المنشورة بشكل كبير في مصدر الخلايا (نخاع العظم، الدهون، الغشاء الزلالي، الحبل السري)، الجرعة (5 ملايين إلى 150 مليون خلية)، طريقة التوصيل (حقن بسيط، سقالة، غراء الفيبرين)، ومقاييس النتائج — مما يجعل المقارنة بين الدراسات صعبة [16].
- ليس لكل تمزق: تمزقات مقبض الدلو المنزاحة المسببة للانحشار الميكانيكي تحتاج إلى رد جراحي بغض النظر عن التدخل البيولوجي. القطع الكبيرة غير المستقرة التي تنقلب إلى الثلمة تتطلب تثبيتاً ميكانيكياً أولاً — يمكن للخلايا الجذعية الوسيطة تعزيز الإصلاح لكن لا يمكنها استبداله.
- لا توجد تجارب عشوائية طويلة المدى تتجاوز 5 سنوات: بينما البيانات متوسطة المدى مشجعة، فإن متانة إصلاح الغضروف الهلالي بوساطة الخلايا الجذعية الوسيطة بعد عقد من الزمن غير معروفة. من الممكن أن يستمر بعض المرضى في التطور إلى التهاب المفاصل، ولكن ببطء أكبر.
- التكلفة والوصول: لا يتم تغطية علاج الخلايا الجذعية الوسيطة عادةً بالتأمين لمؤشرات الغضروف الهلالي ويتطلب دفعاً من الجيب. يجب على المرضى موازنة التكلفة مقابل العبء التراكمي للعيش مع ركبة ناقصة الغضروف الهلالي على مدى عقود.
- تجديدي وليس ترميمي: الخلايا الجذعية الوسيطة لا تعيد نمو غضروف هلالي سليم لعمر 20 عاماً. الهدف هو التحسين الوظيفي وتخفيف الأعراض وتقليل خطر التهاب المفاصل — وليس استبدال الأنسجة.
الصورة الأكبر: لماذا هذا مهم
تمزقات الغضروف الهلالي مهمة أبعد بكثير من الألم الفوري. الركبة التي خضعت لاستئصال غضروف هلالي جزئي لديها خطر متزايد بمقدار 4-6 أضعاف لتطوير التهاب مفاصل شعاعي في غضون 10-15 سنة مقارنة بالركبة غير المصابة [17]. بالنسبة لشخص يبلغ 45 عاماً مع تمزق غضروف هلالي إنسي تنكسي، فإن القرار بين "اقصه الآن" و"جرب الإصلاح البيولوجي" ليس خياراً بين خيارين متكافئين — إنه مفترق طرق حيث يحافظ أحد المسارين على النسيج والآخر يسرع فقدانه.
يمثل علاج الخلايا الجذعية الوسيطة الجيل الأول من الأدوات البيولوجية التي تمنح المرضى والأطباء بديلاً حقيقياً للخيار الجراحي الافتراضي. إنه ليس مثالياً، وليس للجميع. لكن للمريض المناسب — ركبة مستقرة، تمزق تنكسي في المنطقة غير الوعائية، توقعات واقعية، والتزام بإعادة التأهيل — إنه يقدم شيئاً لا يمكن لاستئصال الغضروف الهلالي الجزئي أن يقدمه جوهرياً: إمكانية الشفاء بدلاً من الإزالة [18].
يتطور المجال بسرعة. مع تحسن تقنية السقالات، ونضج فهمنا لجرعة الخلايا المثلى، وتراكم البيانات طويلة المدى، من المرجح أن يصبح إصلاح الغضروف الهلالي البيولوجي معياراً للرعاية لنسبة متزايدة من المرضى — تماماً كما تطور إعادة بناء الرباط الصليبي الأمامي من تجريبي إلى روتيني على مدى عقدين. في الوقت الحالي، هو خيار مدروس بعناية للمرضى الذين يفهمون وعوده وغموضه.
المراجع
- Englund M, Roemer FW, Hayashi D, Crema MD, Guermazi A. Meniscus pathology, osteoarthritis and the treatment controversy. Nature Reviews Rheumatology. 2012;8(7):412-419. doi:10.1038/nrrheum.2012.69 ↩
- Kise NJ, Risberg MA, Stensrud S, et al. Exercise therapy versus arthroscopic partial meniscectomy for degenerative meniscal tear in middle-aged patients: randomised controlled trial with two year follow-up. BMJ. 2016;354:i3740. doi:10.1136/bmj.i3740 ↩
- Sihvonen R, Paavola M, Malmivaara A, et al. Arthroscopic partial meniscectomy versus placebo surgery for a degenerative meniscus tear: a 2-year follow-up of the randomised controlled trial. Annals of the Rheumatic Diseases. 2018;77(2):188-195. doi:10.1136/annrheumdis-2017-211172 ↩
- Baratz ME, Fu FH, Mengato R. Meniscal tears: the effect of meniscectomy and of repair on intraarticular contact areas and stress in the human knee. Am J Sports Med. 1986;14(4):270-275. doi:10.1177/036354658601400403 ↩
- Caplan AI, Correa D. The MSC: an injury drugstore. Cell Stem Cell. 2011;9(1):11-15. doi:10.1016/j.stem.2011.06.008 ↩
- Pak J, Lee JH, Park KS, Park M, Kang LW, Lee SH. Current use of autologous adipose tissue-derived stromal vascular fraction cells for orthopedic applications. J Biomed Sci. 2017;24(1):9. doi:10.1186/s12929-017-0318-z ↩
- Nauta AJ, Fibbe WE. Immunomodulatory properties of mesenchymal stromal cells. Blood. 2007;110(10):3499-3506. doi:10.1182/blood-2007-02-069716 ↩
- Toh WS, Lai RC, Hui JHP, Lim SK. MSC exosome as a cell-free MSC therapy for cartilage regeneration. Semin Cell Dev Biol. 2017;67:56-64. doi:10.1016/j.semcdb.2016.11.008 ↩
- Sekiya I, Katano H, Mizuno M, et al. Alterations in cartilage quantification before and after injections of mesenchymal stem cells into osteoarthritic knees. Sci Rep. 2021;11(1):13832. doi:10.1038/s41598-021-93009-5 ↩
- Krych AJ, Hevesi M, Desai VS, Camp CL, Stuart MJ, Saris DBF. Learning from failure in cartilage repair surgery. Orthop J Sports Med. 2018;6(5):2325967118773041. doi:10.1177/2325967118773041 ↩
- Vangsness CT Jr, Farr J 2nd, Boyd J, Dellaero DT, Mills CR, LeRoux-Williams M. Adult human mesenchymal stem cells delivered via intra-articular injection to the knee following partial medial meniscectomy. J Bone Joint Surg Am. 2014;96(2):90-98. doi:10.2106/JBJS.M.00058 ↩
- Kim YS, Chung PK, Suh DS, Heo DB, Tak DH, Koh YG. Implantation of mesenchymal stem cells in combination with allogenic cartilage improves cartilage regeneration. Int Orthop. 2022;46(10):2277-2287. doi:10.1007/s00264-022-05494-2 ↩
- Collins KH, Herzog W, MacDonald GZ, et al. Obesity, metabolic syndrome, and musculoskeletal disease. Front Physiol. 2018;9:112. doi:10.3389/fphys.2018.00112 ↩
- Dominici M, Le Blanc K, Mueller I, et al. Minimal criteria for defining multipotent mesenchymal stromal cells. Cytotherapy. 2006;8(4):315-317. doi:10.1080/14653240600855905 ↩
- Mithoefer K, Saris DBF, Farr J, et al. Guidelines for the design and conduct of clinical studies in knee articular cartilage repair. Cartilage. 2011;2(2):100-121. doi:10.1177/1947603510397538 ↩
- Brittberg M, Gomoll AH, Canseco JA, Far J, Lind M, Hui J. Cartilage repair in the degenerative ageing knee. Acta Orthop. 2016;87(sup363):26-38. doi:10.1080/17453674.2016.1265877 ↩
- Roos EM. Joint injury causes knee osteoarthritis in young adults. Curr Opin Rheumatol. 2005;17(2):195-200. doi:10.1097/01.bor.0000151391.64395.00 ↩
- Anz AW, Hackel JG, Nilssen EC, Andrews JR. Biological augmentation in the treatment of rotator cuff tears and meniscal injuries. Orthop J Sports Med. 2022;10(3):23259671221084249. doi:10.1177/23259671221084249 ↩
