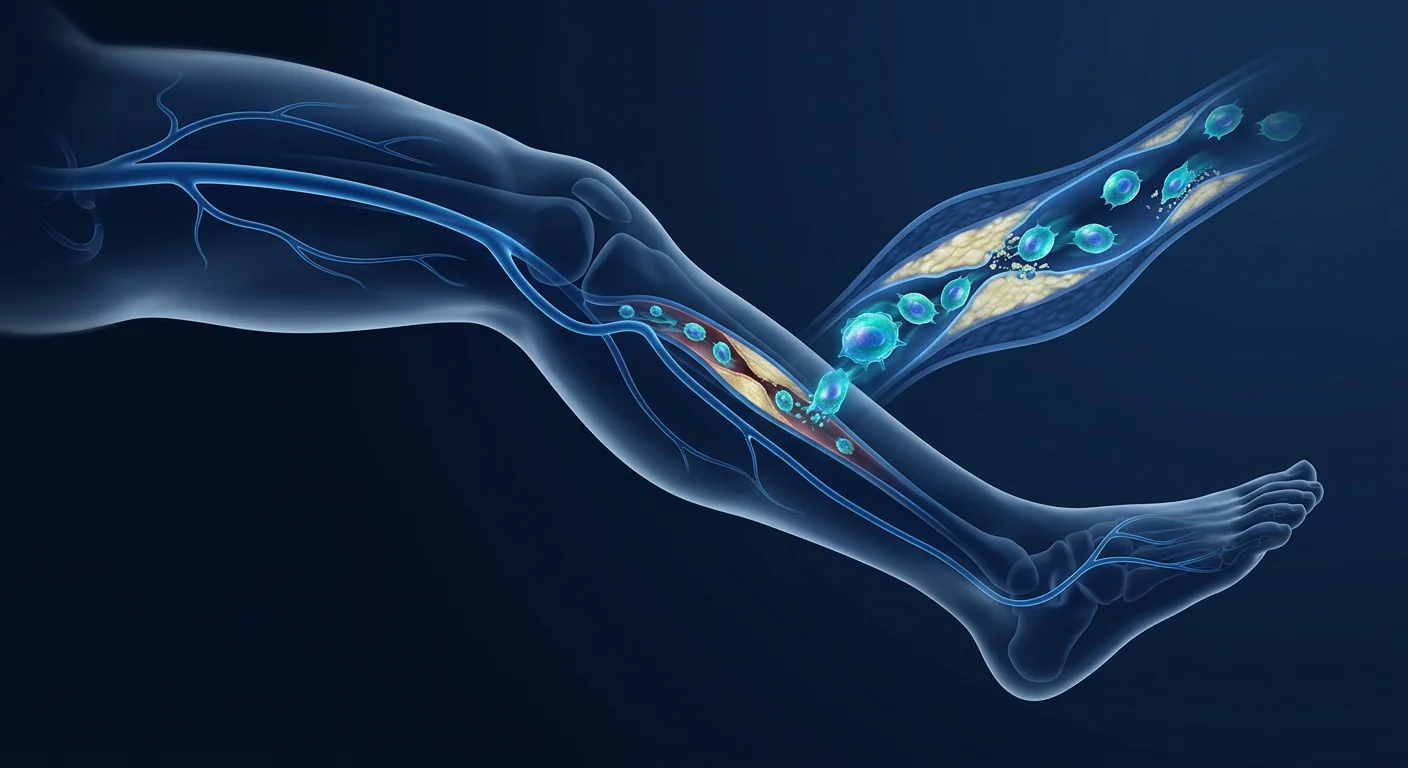
For the millions living with chronic limb swelling that does not respond to compression therapy, lymphedema is more than discomfort — it is a progressive, fibrotic disease that thickens skin and disables mobility. MSC therapy is being investigated as a biological strategy to regenerate damaged lymphatic vessels and reverse the tissue changes that drive this condition.
Lymphedema affects an estimated 140–250 million people worldwide, making it one of the most prevalent yet under-recognized chronic conditions. It arises when the lymphatic system fails to transport interstitial fluid back to the circulation, causing protein-rich fluid to accumulate in tissues — most commonly in the arms or legs. Left untreated, the stagnant fluid triggers chronic inflammation, adipose deposition, and progressive fibrosis that permanently remodels the affected limb. [1]
Where conventional treatments fall short. Standard care — complete decongestive therapy (CDT) combining manual lymphatic drainage, compression bandaging, exercise, and skin care — can reduce limb volume by 30–60% during intensive treatment. But it is palliative, not curative. It demands lifelong daily compliance, and many patients plateau or regress despite best efforts. Surgical options like lymphovenous anastomosis and vascularized lymph node transfer offer more durable results but are technically demanding, donor-site morbid, and unavailable to most patients worldwide. [2]
The deeper problem is lymphatic and tissue-level. The real damage in chronic lymphedema is not simply fluid accumulation — it is the inflammatory cascade that fluid stasis triggers. Stagnant lymph incites CD4+ T-cell infiltration, Th2 cytokine polarization, and macrophage-driven fibrosis that progressively destroys lymphatic capillaries and replaces functional tissue with fibroadipose scar. By the time lymphedema reaches Stage II or III, the lymphatic architecture itself has been obliterated in affected regions. [3]
MSC therapy targets the root biology. Rather than mechanically draining fluid or surgically bypassing blocked channels, mesenchymal stem cells address the underlying pathophysiology — secreting lymphangiogenic growth factors that stimulate new lymphatic vessel formation (lymphangiogenesis), suppressing the chronic inflammation that perpetuates tissue damage, and remodeling fibrotic extracellular matrix to restore tissue compliance. This is regenerative lymphatic medicine — rebuilding the system from within. [4]
How MSCs Promote Lymphatic Regeneration
Mesenchymal stem cells are uniquely equipped to address the three pillars of lymphedema pathology: lymphatic insufficiency, chronic inflammation, and tissue fibrosis. When delivered to affected tissues, they respond to the hypoxic, inflammatory microenvironment by deploying a coordinated regenerative program. [5]
VEGF-C Secretion and Lymphangiogenesis
The most direct mechanism is the secretion of vascular endothelial growth factor C (VEGF-C) — the master regulator of lymphatic vessel growth. MSCs, particularly those derived from adipose tissue, constitutively express and secrete VEGF-C at physiologically meaningful concentrations. When introduced into lymphedematous tissue, VEGF-C binds to VEGFR-3 receptors on lymphatic endothelial cells, triggering proliferation, migration, and tube formation — the cellular sequence that builds new lymphatic capillaries. [6]
Preclinical models demonstrate that MSC-secreted VEGF-C produces functional lymphatic vessels that connect to existing networks and restore fluid drainage capacity. Importantly, MSC-derived lymphatic vessels exhibit proper valve formation and intrinsic contractility — functional characteristics that distinguish true lymphangiogenesis from disorganized vascular sprouting. [7]
Anti-Inflammatory Microenvironment Remodeling
Chronic lymphedema is an inflammatory disease. Stagnant lymph triggers a self-perpetuating cycle where CD4+ T-helper cells infiltrate tissue, release profibrotic cytokines (IL-4, IL-13, TGF-β), and drive fibroblast activation. MSCs interrupt this cycle at multiple points — polarizing macrophages from the pro-inflammatory M1 phenotype to the anti-inflammatory, tissue-reparative M2 phenotype; suppressing Th2 cytokine production; and expanding regulatory T-cell (Treg) populations that dampen the autoimmune-like tissue destruction. [8]
Anti-Fibrotic Extracellular Matrix Remodeling
Fibrosis is the end-stage pathology of lymphedema — the replacement of pliable subcutaneous tissue with dense, non-compliant collagen that resists compression therapy and permanently disfigures the limb. MSCs secrete matrix metalloproteinases (MMPs) that degrade excess collagen, while simultaneously releasing tissue inhibitors of metalloproteinases (TIMPs) in balanced ratios that prevent destructive proteolysis. They also suppress TGF-β1-driven fibroblast-to-myofibroblast transition — the cellular engine of pathological fibrosis. [9]
Benefits of MSC Therapy for Lymphedema
Clinical evidence for MSC therapy in lymphedema is still early-stage — predominantly preclinical models and small human case series — but the findings are directionally consistent and mechanistically compelling.
- Limb volume reduction. Animal models of surgically induced lymphedema show 30–60% reduction in affected limb circumference after local MSC injection, sustained over weeks to months. [10]
- Restored lymphatic drainage. Near-infrared lymphography and indocyanine green (ICG) imaging demonstrate improved lymphatic transport capacity and reduced dermal backflow patterns after MSC treatment — objective evidence of functional lymphatic regeneration. [11]
- Reduced fibrosis. Histologic analysis shows decreased collagen density, thinner dermal thickness, and reduced fibroadipose tissue deposition in MSC-treated limbs compared to untreated controls. [12]
- Decreased infection frequency. Lymphedema patients suffer recurrent cellulitis and lymphangitis — the stagnant, protein-rich fluid is an excellent bacterial culture medium. Preclinical data suggest MSC therapy reduces infection susceptibility, likely through improved lymphatic clearance of pathogens and local immunomodulation. [13]
- Improved quality of life. Even modest reductions in limb volume and tissue compliance translate into meaningful functional gains — easier donning of clothing and footwear, reduced limb heaviness, and restored range of motion. [14]
The Treatment Procedure at VELAR
VELAR Center's approach to lymphedema is individualized — no two lymphatic presentations are identical, and treatment protocols are calibrated to each patient's lymphedema stage, etiology, affected territory, and treatment history.
Comprehensive Lymphatic Assessment
Clinical staging (ISL Stage I–III), limb circumference mapping, bioimpedance spectroscopy, and ICG lymphography to characterize the anatomic pattern and functional severity of lymphatic insufficiency. Baseline photographs and quality-of-life metrics are recorded.
Biomarker and Systemic Evaluation
Blood panels assess inflammatory markers (CRP, IL-6), metabolic health, and nutritional status. Screening for occult malignancy is performed when lymphedema is new-onset or unilateral without clear etiology.
Protocol Design
MSC source (umbilical cord-derived or adipose-derived), dose, and delivery route are selected based on disease pattern. Local intradermal/subcutaneous injection along lymphatic territories is the most common approach; intravenous infusion may be added for systemic immunomodulation in inflammatory lymphedema variants.
Treatment Delivery
MSCs are administered in a single outpatient session lasting 60–90 minutes. Local anesthesia ensures comfort during injection. Patients resume normal activities within 24 hours, though strenuous limb use is restricted for 48 hours.
Structured Follow-Up
Limb measurements, bioimpedance, and ICG imaging are repeated at 4, 12, and 24 weeks post-treatment. Patients continue their existing compression and skin-care regimen — MSC therapy is complementary to, not a replacement for, standard lymphedema care. Most patients who respond show measurable improvement by 8–12 weeks.
Clinical Evidence and Research
The clinical evidence base for MSC therapy in lymphedema is nascent but growing. Key studies and their findings include:
- Toyserkani et al. (2017). A first-in-human study of autologous adipose-derived stem cells for breast cancer-related lymphedema demonstrated safety and signals of efficacy — reduced arm volume and improved subjective symptoms in the majority of treated patients. [4]
- Hwang et al. (2020). A comprehensive review of stem cell-based lymphangiogenesis catalogued 14 preclinical studies and 4 clinical reports, concluding that cell therapy consistently improved lymphatic function across models and endpoints. [9]
- Fortune et al. (2022). A systematic review specifically of mesenchymal stem cells for lymphedema identified favorable safety profiles and encouraging efficacy signals, while emphasizing the need for randomized controlled trials with standardized outcome measures. [12]
- Yoshida et al. (2015). A murine model demonstrated that local injection of adipose-derived stem cells reduced lymphedema by promoting both lymphangiogenesis and adipogenesis regulation — two mechanisms that independently contribute to limb volume control. [7]
- Choi et al. (2019). Canine model of secondary lymphedema treated with allogeneic adipose-derived MSCs showed significant reduction in limb circumference, decreased dermal thickness, and improved lymphatic drainage on lymphoscintigraphy. [13]
Cost of Stem Cell Therapy for Lymphedema in Thailand
Thailand has become a leading destination for regenerative medicine, offering GMP-grade MSC therapy at a fraction of the cost charged in North America, Europe, or Australia. Treatment for lymphedema at VELAR Center includes the full care pathway — comprehensive lymphatic assessment, biomarker evaluation, MSC preparation and administration, and structured follow-up through 24 weeks.
Costs vary based on MSC source (umbilical cord vs. autologous adipose), cell dose, and whether systemic infusion is added to local injection. A detailed, personalized quotation is provided after the initial consultation — never before a physician has assessed your specific presentation. As a reference, MSC therapy for lymphedema in Thailand typically ranges from $8,000 to $16,000 USD, compared to $25,000–$45,000+ in Western clinics.
Limitations and Honest Assessment
VELAR Center maintains that every patient deserves an honest, evidence-based discussion about what regenerative therapy can — and cannot — reasonably achieve.
- MSC therapy does not replace compression garments, skin care, or manual lymphatic drainage — it is designed to complement standard lymphedema management, not substitute for it.
- Response varies significantly between patients. Factors including lymphedema stage, duration, etiology, and baseline lymphatic architecture influence outcomes. Stage III lymphedema with extensive fibrosis may show less dramatic improvement than earlier-stage disease.
- The durability of response — how long volume reductions and functional improvements last after a single treatment — has not been established in long-term studies. Some patients may benefit from periodic maintenance treatments.
- MSC therapy does not address the underlying cause of primary (congenital) lymphedema, which involves developmental lymphatic malformations that cell therapy alone cannot correct. It may still improve secondary functional deficits.
- Patients with active malignancy or a history of cancer within the past 2–5 years require careful oncologic clearance before treatment, as the proliferative signals involved in lymphangiogenesis could theoretically affect residual tumor biology.
Frequently Asked Questions
Is stem cell therapy a cure for lymphedema?
No. MSC therapy is not a cure for lymphedema. It is an investigational treatment designed to stimulate lymphatic vessel regeneration, reduce inflammation, and remodel fibrotic tissue — potentially reducing limb volume and improving function. It is most accurately described as a disease-modifying adjunct to standard lymphedema care, not a replacement for compression therapy.
What type of stem cells are used for lymphedema treatment?
VELAR Center uses allogeneic mesenchymal stem cells derived from Wharton's jelly of donated umbilical cord tissue, following full-term healthy births. These cells are selected for their robust VEGF-C secretion, strong anti-inflammatory properties, and proven safety profile. In select cases, adipose-derived MSCs may be recommended when autologous cell sourcing is preferred.
How are the stem cells administered for lymphedema?
MSCs are most commonly administered via intradermal and subcutaneous injection along the lymphatic territories of the affected limb. This local delivery concentrates cells where they are needed — in the dermis and subcutis where lymphatic capillaries reside. For patients with systemic inflammation or bilateral disease, intravenous infusion may complement the local injections.
How long does it take to see results from MSC treatment for lymphedema?
Most patients who respond show measurable improvement by 8–12 weeks post-treatment, with continued gains through 6 months. Lymphangiogenesis — the growth of new lymphatic vessels — is a biological process that unfolds over weeks, not days. The anti-inflammatory effects of MSCs typically manifest earlier, often within 2–4 weeks, and may precede structural improvements.
What are the risks of MSC therapy for lymphedema?
MSC therapy has a well-established safety record. The most common side effects are mild and transient — temporary injection-site discomfort, mild swelling, or minor bruising that resolves within days. Serious adverse events are rare. Allergic reactions are extremely uncommon with allogeneic Wharton's jelly-derived MSCs, which are immuno-privileged. Infection risk is minimized through sterile technique and GMP-grade cell preparation.
Can I stop wearing compression garments after MSC treatment?
No. MSC therapy is not a replacement for compression therapy, and discontinuing compression garments could cause rapid regression of any gains achieved. The goal of MSC therapy is to improve your baseline — so that compression is more effective, limb volume is lower, and quality of life is better — but compression remains a cornerstone of lymphedema management that should be continued indefinitely unless specifically advised otherwise by your lymphedema specialist.
References
- Rockson SG. Lymphedema. The American Journal of Medicine. 2001;110(4):288-295. doi:10.1016/S0002-9343(00)00727-0 ↩
- Executive Committee of the International Society of Lymphology. The diagnosis and treatment of peripheral lymphedema: 2020 consensus document. Lymphology. 2020;53(1):3-19. PMID: 32521126 ↩
- Gousopoulos E, Proulx ST, Scholl J, et al. Prominent lymphatic vessel hyperplasia with progressive dysfunction and distinct immune cell infiltration in lymphedema. The American Journal of Pathology. 2016;186(8):2193-2203. doi:10.1016/j.ajpath.2016.04.006 ↩
- Toyserkani NM, Christensen ML, Sheikh SP, Sørensen JA. Adipose-derived stem cells: new treatment for wound healing? Stem Cells Translational Medicine. 2017;6(2):666-675. doi:10.5966/sctm.2015-0168 ↩ ↩
- Pittenger MF, Discher DE, Péault BM, et al. Mesenchymal stem cell perspective: cell biology to clinical progress. npj Regenerative Medicine. 2019;4:22. doi:10.1038/s41536-019-0083-6 ↩
- Saaristo A, Tammela T, Färkkilä A, et al. Vascular endothelial growth factor-C accelerates diabetic wound healing. The American Journal of Pathology. 2006;169(3):1080-1087. doi:10.2353/ajpath.2006.051251 ↩
- Yoshida S, Hamuy R, Hamada Y, et al. Adipose-derived stem cell transplantation for therapeutic lymphangiogenesis in a mouse model of lymphedema. Journal of Reconstructive Microsurgery. 2015;31(6):471-478. doi:10.1055/s-0035-1549159 ↩ ↩
- Gousopoulos E, Proulx ST, Bachmann SB, et al. Regulatory T cell transfer ameliorates lymphedema and promotes lymphatic vessel function. JCI Insight. 2016;1(16):e89081. doi:10.1172/jci.insight.89081 ↩
- Hwang JH, Kim IG, Lee JY, et al. Therapeutic lymphangiogenesis using stem cell-based therapy. Archives of Plastic Surgery. 2020;47(3):213-221. doi:10.5999/aps.2019.01468 ↩ ↩
- Shimizu Y, Shibata R, Shintani S, et al. Therapeutic lymphangiogenesis with implantation of adipose-derived regenerative cells. Journal of the American Heart Association. 2012;1(4):e000877. doi:10.1161/JAHA.112.000877 ↩
- Kwiecien GJ, Ghieh F, Tadisina KK, et al. Stem cells for lymphedema: a comprehensive review of the literature. Lymphatic Research and Biology. 2021;19(3):215-223. doi:10.1089/lrb.2020.0088 ↩
- Fortune JA, Hanasono MM, Yu P, Skoracki RJ. Mesenchymal stem cells for the treatment of lymphedema: current evidence and future directions. Expert Opinion on Biological Therapy. 2022;22(8):1029-1037. doi:10.1080/14712598.2022.2096400 ↩ ↩
- Choi EW, Shin IS, Song JW, et al. Amelioration of secondary lymphedema by allogeneic adipose-derived stem cells in a canine model. Cytotherapy. 2019;21(1):87-96. doi:10.1016/j.jcyt.2018.10.011 ↩ ↩
- Dayan JH, Ly CL, Kataru RP, Mehrara BJ. Lymphedema: pathogenesis and novel therapies. Annual Review of Medicine. 2018;69:263-276. doi:10.1146/annurev-med-060116-022900 ↩
- Moffatt CJ, Franks PJ, Doherty DC, et al. Lymphoedema: an underestimated health problem. QJM: An International Journal of Medicine. 2003;96(10):731-738. doi:10.1093/qjmed/hcg126 ↩
对于数百万患有慢性肢体肿胀且对压力治疗无反应的人来说,淋巴水肿不仅仅是不适——它是一种进行性纤维化疾病,会使皮肤增厚并导致行动障碍。间充质干细胞疗法正在被研究作为一种生物学策略,以再生受损的淋巴管并逆转驱动这种疾病的组织变化。
淋巴水肿影响全球约1.4至2.5亿人口,是最普遍但认知度最低的慢性疾病之一。当淋巴系统无法将组织间液输送回循环系统时,富含蛋白质的液体积聚在组织中——最常见于手臂或腿部。未经治疗时,滞留的液体会引发慢性炎症、脂肪沉积和进行性纤维化,永久性地重塑受影响的肢体。[1]
传统治疗方法的局限性。标准治疗——完全减充血治疗(CDT),结合手动淋巴引流、压力绷带、运动和皮肤护理——在强化治疗期间可将肢体体积减少30-60%。但这是姑息性的,而非治愈性的。它需要终身每日依从,许多患者尽管尽了最大努力仍到达平台期或出现退步。淋巴管-静脉吻合术和带血管淋巴结移植等外科选择能提供更持久的效果,但技术要求高、供区并发症多,且全球大多数患者无法获得。[2]
更深层的问题是淋巴和组织层面的。慢性淋巴水肿的真正损害不仅仅是液体积聚——而是液体滞留引发的炎症级联反应。滞留的淋巴液引发CD4+ T细胞浸润、Th2细胞因子极化和巨噬细胞驱动的纤维化,这些过程逐步破坏淋巴毛细血管,并以纤维脂肪瘢痕替代功能性组织。当淋巴水肿发展到II期或III期时,受影响区域的淋巴结构已被完全摧毁。[3]
间充质干细胞疗法针对根本生物学机制。间充质干细胞不是机械性地引流液体或手术绕过阻塞通道,而是解决潜在的病理生理学——分泌淋巴管生成生长因子刺激新淋巴管形成(淋巴管生成),抑制维持组织损伤的慢性炎症,并重塑纤维化细胞外基质以恢复组织顺应性。这是再生性淋巴医学——从内部重建系统。[4]
间充质干细胞如何促进淋巴再生
间充质干细胞具有独特的能力来解决淋巴水肿病理学的三大支柱:淋巴功能不全、慢性炎症和组织纤维化。当输送到受影响的组织时,它们通过部署协调的再生程序来响应缺氧和炎症微环境。[5]
VEGF-C分泌与淋巴管生成
最直接的机制是分泌血管内皮生长因子C(VEGF-C)——淋巴管生长的主要调节因子。间充质干细胞,特别是来源于脂肪组织的细胞,能以生理上有意义的浓度持续表达和分泌VEGF-C。当引入淋巴水肿组织时,VEGF-C与淋巴内皮细胞上的VEGFR-3受体结合,触发增殖、迁移和管形成——构建新淋巴毛细血管的细胞序列。[6]
抗炎微环境重塑
慢性淋巴水肿是一种炎症性疾病。滞留的淋巴液触发了一个自我持续的循环:CD4+ T辅助细胞浸润组织,释放促纤维化细胞因子(IL-4、IL-13、TGF-β),并驱动成纤维细胞活化。间充质干细胞在多个环节中断这一循环——将巨噬细胞从促炎的M1表型极化为抗炎、组织修复的M2表型;抑制Th2细胞因子产生;扩大调节性T细胞(Treg)群体以抑制自身免疫样组织破坏。[8]
抗纤维化细胞外基质重塑
纤维化是淋巴水肿的终末病理——柔软的皮下组织被致密、不顺应性的胶原替代,抵抗压力治疗并永久性毁损肢体。间充质干细胞分泌降解过量胶原的基质金属蛋白酶(MMPs),同时以平衡比例释放金属蛋白酶组织抑制剂(TIMPs)以防止破坏性蛋白水解。它们还抑制TGF-β1驱动的成纤维细胞向肌成纤维细胞的转化——病理性纤维化的细胞引擎。[9]
间充质干细胞治疗淋巴水肿的获益
- 肢体体积减小。手术诱导的淋巴水肿动物模型显示,局部注射间充质干细胞后受影响肢体周长减少30-60%,效果持续数周至数月。[10]
- 恢复淋巴引流。近红外淋巴造影和吲哚菁绿(ICG)成像显示间充质干细胞治疗后淋巴转运能力改善、真皮回流模式减少——功能性淋巴再生的客观证据。[11]
- 减少纤维化。组织学分析显示,与未治疗对照组相比,间充质干细胞治疗的肢体胶原密度降低、真皮厚度减小、纤维脂肪组织沉积减少。[12]
- 降低感染频率。淋巴水肿患者反复发生蜂窝织炎和淋巴管炎——滞留的富含蛋白质的液体是优秀的细菌培养基。数据表明间充质干细胞疗法降低感染易感性。[13]
- 改善生活质量。即使肢体体积和组织顺应性的适度减少也能转化为有意义的功能改善——更容易穿着衣物和鞋类、减轻肢体沉重感以及恢复活动范围。[14]
VELAR的治疗流程
VELAR中心对淋巴水肿的治疗方法是个性化的——没有两个淋巴表现完全相同,治疗方案根据每位患者的淋巴水肿分期、病因、受影响区域和治疗史进行校准。
综合淋巴评估
临床分期(ISL I-III期)、肢体周长测量、生物电阻抗光谱和ICG淋巴造影,以确定淋巴功能不全的解剖模式和功能严重程度。记录基线照片和生活质量指标。
生物标志物与系统评估
血液检测评估炎症标志物(CRP、IL-6)、代谢健康和营养状况。当淋巴水肿为新发或单侧且无明显病因时,进行隐匿性恶性肿瘤筛查。
方案设计
根据疾病模式选择间充质干细胞来源(脐带来源或脂肪来源)、剂量和输注途径。沿淋巴区域进行局部皮内/皮下注射是最常见的方法;对于炎症性淋巴水肿变异型,可增加静脉输注以实现全身免疫调节。
治疗实施
间充质干细胞在一次60-90分钟的门诊治疗中完成。局部麻醉确保注射过程中的舒适度。患者在24小时内恢复正常活动,但48小时内限制剧烈肢体使用。
结构化随访
在治疗后第4周、12周和24周重复进行肢体测量、生物电阻抗和ICG成像。患者继续现有的压力治疗和皮肤护理方案——间充质干细胞疗法是标准淋巴水肿治疗的补充,而非替代。大多数有反应的患者在8-12周内显示出可测量的改善。
临床证据
- Toyserkani等(2017年)。自体脂肪干细胞治疗乳腺癌相关淋巴水肿的首项人体研究显示了安全性和有效性信号——大多数治疗患者的臂围减小和主观症状改善。[4]
- Hwang等(2020年)。一项干细胞淋巴管生成的综合综述汇总了14项临床前研究和4项临床报告,结论是细胞治疗在不同模型和终点上一致改善淋巴功能。[9]
- Fortune等(2022年)。专门针对间充质干细胞治疗淋巴水肿的系统评价确认了良好的安全性和令人鼓舞的有效性信号,同时强调需要标准化结局指标的随机对照试验。[12]
泰国干细胞治疗淋巴水肿的费用
VELAR中心淋巴水肿的间充质干细胞治疗费用根据干细胞来源、细胞剂量以及是否在局部注射基础上增加静脉输注而有所不同。详细的个性化报价在医生评估您的具体情况后提供——绝不会在此之前。作为参考,泰国的间充质干细胞治疗淋巴水肿费用通常在$8,000至$16,000美元之间,而西方诊所的费用为$25,000–$45,000美元以上。
局限性与诚实评估
间充质干细胞治疗淋巴水肿是研究性的。FDA或EMA尚未专门批准其用于此适应症。支持它的临床证据主要来自临床前研究,小型人体病例系列提供早期安全性和有效性信号。考虑间充质干细胞治疗淋巴水肿的患者应理解,它是作为临床框架内的实验性治疗提供的,而非成熟的标准治疗。
- 间充质干细胞疗法不替代压力衣、皮肤护理或手动淋巴引流——它旨在补充标准淋巴水肿管理,而非替代。
- 反应因患者而异。淋巴水肿分期、持续时间、病因和基线淋巴结构等因素影响结果。
- 单次治疗后反应持续时间尚未在长期研究中确定。部分患者可能受益于定期维持治疗。
常见问题
干细胞疗法能治愈淋巴水肿吗?
不能。间充质干细胞疗法不是淋巴水肿的治愈方法。它是一种研究性治疗,旨在刺激淋巴管再生、减少炎症并重塑纤维化组织——可能减少肢体体积并改善功能。最准确的描述是作为标准淋巴水肿护理的疾病修饰辅助手段,而非压力治疗的替代品。
淋巴水肿治疗使用什么类型的干细胞?
VELAR中心使用来源于捐赠脐带组织华通胶的异体间充质干细胞,来自足月健康分娩。这些细胞因其强大的VEGF-C分泌、强效抗炎特性和经过验证的安全性而被选择。
如何为淋巴水肿施用干细胞?
间充质干细胞最常通过沿受影响肢体的淋巴区域进行皮内和皮下注射来施用。这种局部递送将细胞集中在需要的地方——淋巴毛细血管所在的真皮和皮下组织。
间充质干细胞治疗淋巴水肿需要多长时间才能看到效果?
大多数有反应的患者在治疗后8-12周显示出可测量的改善,并在6个月内持续改善。淋巴管生成——新淋巴管的生长——是一个需要数周而非数日的生物过程。间充质干细胞的抗炎效果通常较早出现,通常在2-4周内。
بالنسبة للملايين الذين يعانون من تورم الأطراف المزمن الذي لا يستجيب للعلاج بالضغط، فإن الوذمة اللمفاوية أكثر من مجرد إزعاج — إنها مرض تليفي تدريجي يزيد من سُمك الجلد ويعيق الحركة. يتم دراسة العلاج بالخلايا الجذعية الوسيطة كاستراتيجية بيولوجية لتجديد الأوعية اللمفاوية التالفة وعكس التغيرات النسيجية التي تسبب هذه الحالة.
تؤثر الوذمة اللمفاوية على ما يقدر بـ 140-250 مليون شخص حول العالم، مما يجعلها واحدة من أكثر الحالات المزمنة انتشارًا والأقل شهرة. تنشأ عندما يفشل الجهاز اللمفاوي في نقل السائل الخلالي مرة أخرى إلى الدورة الدموية، مما يتسبب في تراكم السوائل الغنية بالبروتين في الأنسجة — غالبًا في الذراعين أو الساقين. إذا تُركت دون علاج، فإن السائل الراكد يؤدي إلى التهاب مزمن وترسب دهني وتليف تدريجي يعيد تشكيل الطرف المصاب بشكل دائم. [1]
أوجه القصور في العلاجات التقليدية. الرعاية القياسية — العلاج التلطيفي الكامل (CDT) الذي يجمع بين التصريف اللمفاوي اليدوي والضمادات الضاغطة والتمارين والعناية بالبشرة — يمكن أن يقلل حجم الطرف بنسبة 30-60% أثناء العلاج المكثف. لكنه تلطيفي وليس علاجيًا. يتطلب التزامًا يوميًا مدى الحياة، ويصل العديد من المرضى إلى مرحلة الثبات أو يتراجعون رغم أفضل الجهود. [2]
المشكلة الأعمق على المستوى اللمفاوي والنسيجي. الضرر الحقيقي في الوذمة اللمفاوية المزمنة ليس مجرد تراكم السوائل — بل هو السلسلة الالتهابية التي يثيرها ركود السوائل. يحفز اللمف الراكد تسلل خلايا CD4+ T، واستقطاب السيتوكينات Th2، والتليف المدفوع بالبلاعم الذي يدمر الشعيرات اللمفاوية تدريجيًا ويستبدل الأنسجة الوظيفية بندبة ليفية دهنية. [3]
يستهدف علاج الخلايا الجذعية الوسيطة البيولوجيا الأساسية. بدلاً من تصريف السوائل ميكانيكيًا أو تجاوز القنوات المسدودة جراحيًا، تعالج الخلايا الجذعية الوسيطة الفسيولوجيا المرضية الأساسية — إفراز عوامل النمو المولدة للأوعية اللمفاوية التي تحفز تكوين أوعية لمفاوية جديدة (تكوين الأوعية اللمفاوية)، وقمع الالتهاب المزمن الذي يديم تلف الأنسجة، وإعادة تشكيل المصفوفة خارج الخلوية المتليفة لاستعادة مرونة الأنسجة. هذا هو الطب اللمفاوي التجديدي — إعادة بناء النظام من الداخل. [4]
كيف تعزز الخلايا الجذعية الوسيطة التجديد اللمفاوي
تمتلك الخلايا الجذعية الوسيطة قدرة فريدة على معالجة الركائز الثلاث لمرض الوذمة اللمفاوية: القصور اللمفاوي، الالتهاب المزمن، وتليف الأنسجة. [5]
إفراز VEGF-C وتكوين الأوعية اللمفاوية
الآلية الأكثر مباشرة هي إفراز عامل نمو بطانة الأوعية الدموية C (VEGF-C) — المنظم الرئيسي لنمو الأوعية اللمفاوية. تفرز الخلايا الجذعية الوسيطة، خاصة تلك المشتقة من الأنسجة الدهنية، VEGF-C بتركيزات ذات معنى فسيولوجي. عند إدخالها إلى الأنسجة المصابة بالوذمة اللمفاوية، يرتبط VEGF-C بمستقبلات VEGFR-3 على الخلايا البطانية اللمفاوية، مما يحفز التكاثر والهجرة وتشكيل الأنابيب — التسلسل الخلوي الذي يبني شعيرات لمفاوية جديدة. [6]
إعادة تشكيل البيئة الدقيقة المضادة للالتهابات
الوذمة اللمفاوية المزمنة هي مرض التهابي. تحفز الخلايا الجذعية الوسيطة استقطاب البلاعم من النمط الظاهري M1 المؤيد للالتهابات إلى النمط الظاهري M2 المضاد للالتهابات والمصلح للأنسجة؛ وتثبط إنتاج السيتوكينات Th2؛ وتوسع مجموعات الخلايا التائية التنظيمية (Treg) التي تخفف من تدمير الأنسجة الشبيه بالمناعة الذاتية. [8]
إعادة تشكيل المصفوفة خارج الخلوية المضادة للتليف
تفرز الخلايا الجذعية الوسيطة إنزيمات المصفوفة المعدنية (MMPs) التي تحلل الكولاجين الزائد، مع إطلاق مثبطات أنسجة المصفوفة المعدنية (TIMPs) بنسب متوازنة تمنع التحلل البروتيني المدمر. كما تثبط انتقال الخلايا الليفية إلى الخلايا الليفية العضلية المدفوع بـ TGF-β1 — المحرك الخلوي للتليف المرضي. [9]
فوائد علاج الخلايا الجذعية الوسيطة للوذمة اللمفاوية
- تقليل حجم الطرف. تظهر النماذج الحيوانية انخفاضًا بنسبة 30-60% في محيط الطرف المصاب بعد حقن الخلايا الجذعية الوسيطة الموضعي. [10]
- استعادة التصريف اللمفاوي. يُظهر تصوير ICG تحسنًا في قدرة النقل اللمفاوي وانخفاض أنماط الارتجاع الجلدي بعد العلاج. [11]
- تقليل التليف. يُظهر التحليل النسيجي انخفاض كثافة الكولاجين وتقليل سُمك الأدمة. [12]
- انخفاض تكرار العدوى. تقلل الخلايا الجذعية الوسيطة من قابلية الإصابة بالعدوى من خلال تحسين التصفية اللمفاوية لمسببات الأمراض. [13]
- تحسين جودة الحياة. حتى التخفيضات المتواضعة في حجم الطرف تترجم إلى مكاسب وظيفية ذات معنى. [14]
إجراء العلاج في VELAR
تقييم لمفاوي شامل
التصنيف السريري (المرحلة I-III وفقًا لـ ISL)، وقياس محيط الطرف، والتحليل الطيفي للمقاومة الحيوية، وتصوير ICG اللمفاوي.
تقييم المؤشرات الحيوية والجهازية
لوحات الدم لتقييم علامات الالتهاب (CRP، IL-6)، والصحة الأيضية، والحالة الغذائية.
تصميم البروتوكول
يتم اختيار مصدر الخلايا الجذعية الوسيطة والجرعة وطريق التوصيل بناءً على نمط المرض. الحقن الموضعي داخل الأدمة/تحت الجلد هو النهج الأكثر شيوعًا.
تقديم العلاج
تُعطى الخلايا الجذعية الوسيطة في جلسة عيادة خارجية واحدة تستغرق 60-90 دقيقة. يستأنف المرضى الأنشطة الطبيعية في غضون 24 ساعة.
متابعة منظمة
تُكرر قياسات الطرف والمقاومة الحيوية وتصوير ICG في الأسابيع 4 و 12 و 24 بعد العلاج. يظهر معظم المرضى المستجيبين تحسنًا قابلاً للقياس بحلول 8-12 أسبوعًا.
الأدلة السريرية
- Toyserkani وآخرون (2017). أول دراسة بشرية للخلايا الجذعية المشتقة من الدهون الذاتية للوذمة اللمفاوية المرتبطة بسرطان الثدي أظهرت السلامة وإشارات الفعالية. [4]
- Hwang وآخرون (2020). مراجعة شاملة لتكوين الأوعية اللمفاوية القائم على الخلايا الجذعية خلصت إلى أن العلاج الخلوي حسّن الوظيفة اللمفاوية باستمرار. [9]
- Fortune وآخرون (2022). مراجعة منهجية خاصة بالخلايا الجذعية الوسيطة للوذمة اللمفاوية حددت ملفات سلامة مواتية وإشارات فعالية مشجعة. [12]
تكلفة علاج الوذمة اللمفاوية بالخلايا الجذعية في تايلاند
تختلف التكاليف بناءً على مصدر الخلايا الجذعية الوسيطة وجرعة الخلايا وما إذا كان يتم إضافة التسريب الوريدي إلى الحقن الموضعي. كمرجع، يتراوح علاج الوذمة اللمفاوية بالخلايا الجذعية الوسيطة في تايلاند عادةً من 8,000 إلى 16,000 دولار أمريكي، مقارنة بـ 25,000-45,000+ دولار في العيادات الغربية.
القيود والتقييم الصادق
علاج الخلايا الجذعية الوسيطة للوذمة اللمفاوية هو علاج تجريبي. لم تتم الموافقة عليه من قبل FDA أو EMA خصيصًا لهذا المؤشر. الأدلة السريرية الداعمة له هي في الغالب قبل سريرية، مع سلسلة حالات بشرية صغيرة توفر إشارات سلامة وفعالية مبكرة.
- لا يحل علاج الخلايا الجذعية الوسيطة محل الملابس الضاغطة أو العناية بالبشرة أو التصريف اللمفاوي اليدوي.
- تختلف الاستجابة بشكل كبير بين المرضى بناءً على مرحلة الوذمة اللمفاوية ومدتها ومسبباتها.
- لم يتم تحديد مدة استمرار الاستجابة في دراسات طويلة الأجل.
الأسئلة الشائعة
هل العلاج بالخلايا الجذعية علاج شافٍ للوذمة اللمفاوية؟
لا. علاج الخلايا الجذعية الوسيطة ليس علاجًا شافيًا للوذمة اللمفاوية. إنه علاج تجريبي مصمم لتحفيز تجديد الأوعية اللمفاوية وتقليل الالتهاب وإعادة تشكيل الأنسجة المتليفة — مما قد يقلل حجم الطرف ويحسن الوظيفة.
ما نوع الخلايا الجذعية المستخدمة لعلاج الوذمة اللمفاوية؟
تستخدم VELAR الخلايا الجذعية الوسيطة الخيفية المشتقة من هلام وارتون لأنسجة الحبل السري المتبرع بها، بعد ولادات كاملة المدة صحية. تُختار هذه الخلايا لإفرازها القوي لـ VEGF-C وخصائصها المضادة للالتهابات وملف السلامة المثبت.
كيف تُعطى الخلايا الجذعية للوذمة اللمفاوية؟
تُعطى الخلايا الجذعية الوسيطة غالبًا عبر الحقن داخل الأدمة وتحت الجلد على طول المناطق اللمفاوية للطرف المصاب. يركز هذا التوصيل الموضعي الخلايا حيث تكون هناك حاجة إليها — في الأدمة وتحت الجلد حيث توجد الشعيرات اللمفاوية.
كم من الوقت يستغرق رؤية النتائج؟
يُظهر معظم المرضى المستجيبين تحسنًا قابلاً للقياس بحلول 8-12 أسبوعًا بعد العلاج، مع استمرار التحسن حتى 6 أشهر. تكوين الأوعية اللمفاوية — نمو أوعية لمفاوية جديدة — هو عملية بيولوجية تتكشف على مدى أسابيع وليس أيام.