Lumbar disc degeneration is the most common structural cause of chronic low back pain, affecting an estimated 40% of adults under 60 and over 80% of those above 80 years old. It is not merely a consequence of aging — it is a progressive biological cascade involving cellular senescence, extracellular matrix breakdown, inflammation, and biomechanical failure that ranks as the leading cause of disability worldwide [1].
Where conventional treatments fall short. Physical therapy, NSAIDs, epidural steroid injections, and spinal fusion surgery are the current standard of care — but none of them addresses the underlying disc pathology. Epidural injections provide temporary symptom relief but do not restore disc height. Spinal fusion stabilizes the segment but eliminates motion, transfers mechanical stress to adjacent levels, and carries a 25–36% rate of adjacent segment disease within ten years [2]. These interventions manage the consequences of degeneration without reversing the process itself.
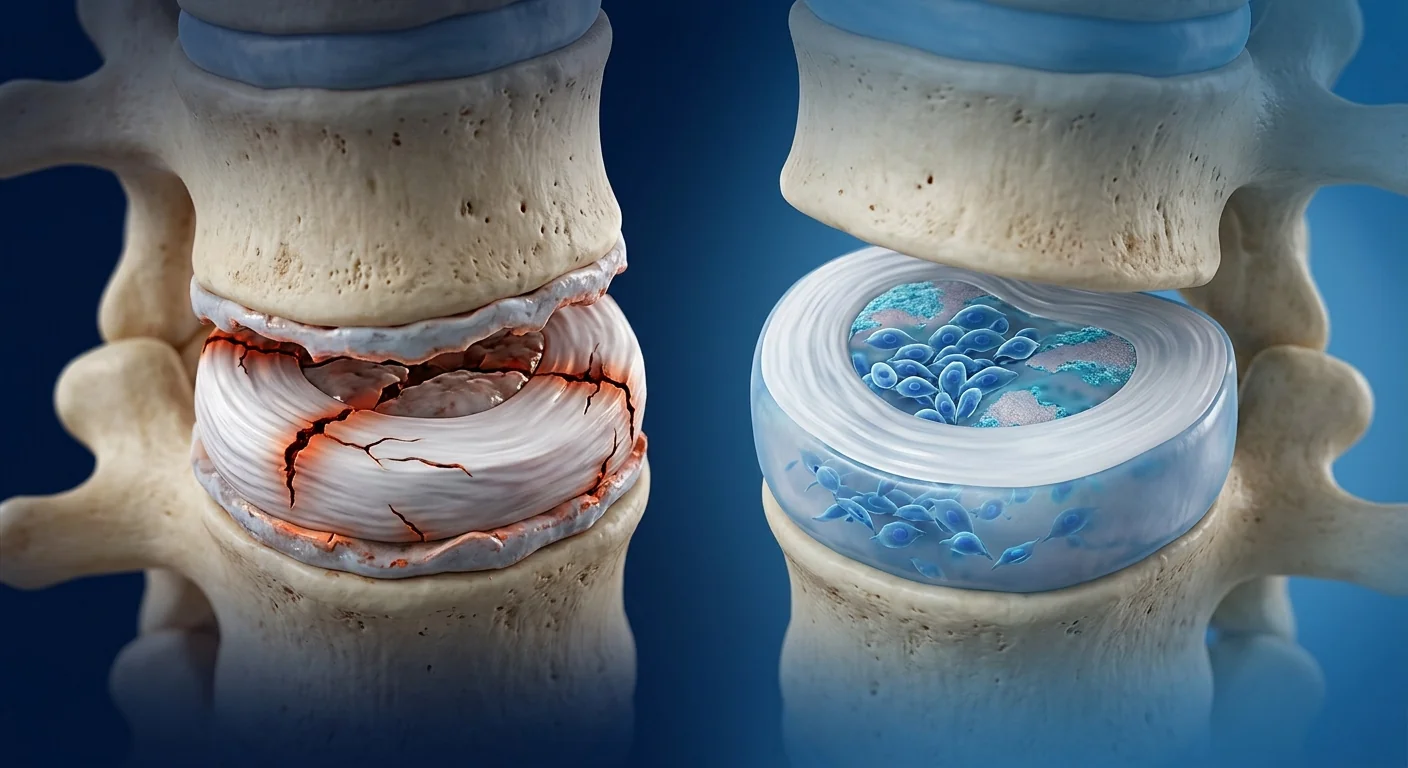
The deeper problem is cellular. Intervertebral discs are the largest avascular structures in the human body, relying on nutrient diffusion through cartilaginous endplates. With age and cumulative mechanical loading, the resident cell population of the nucleus pulposus — primarily notochordal cells and chondrocyte-like cells — declines sharply. As cellularity drops, synthesis of aggrecan and type II collagen cannot keep pace with matrix metalloproteinase-driven degradation, leading to progressive disc height loss, dehydration, annular fissuring, and ultimately herniation [3].
MSC therapy targets the root cause. Rather than bypassing disc degeneration, mesenchymal stem cells address the fundamental deficit: loss of functional, matrix-synthesizing cells in the nucleus pulposus. MSCs can differentiate toward a nucleus pulposus-like phenotype, secrete trophic factors that stimulate resident cell proliferation, and exert potent anti-inflammatory effects that interrupt the degenerative cascade [4]. This multi-mechanism approach — replenishing cells, stimulating matrix repair, and calming inflammation — is what distinguishes MSC therapy from all current standard-of-care interventions for lumbar disc degeneration.
How MSCs Target the Pathophysiology of Lumbar Disc Degeneration
MSCs address lumbar disc degeneration through several interconnected mechanisms, each supported by a growing body of preclinical and clinical evidence:
1. Differentiation into nucleus pulposus-like cells. When cultured under hypoxic conditions mimicking the native disc environment (1–5% O₂) with appropriate growth factor stimulation — including TGF-β3 and GDF-5 — both bone marrow-derived and umbilical cord-derived MSCs upregulate nucleus pulposus marker genes such as SOX9, ACAN, COL2A1, and FOXF1 while downregulating osteogenic and adipogenic markers. The resulting cells synthesize a proteoglycan-rich extracellular matrix closely resembling native nucleus pulposus tissue [5].
2. Paracrine stimulation of resident disc cells. Even when MSCs do not persist long-term in the disc, their therapeutic benefit is largely paracrine. MSC-conditioned medium — containing exosomes, growth factors (TGF-β, IGF-1, BMP-2, BMP-7), and extracellular vesicles — stimulates nucleus pulposus cell proliferation by 2–3 fold in vitro and increases aggrecan and collagen II synthesis by 40–80% over two to three weeks of culture [6]. This "hit-and-run" mechanism means even transient MSC engraftment can produce lasting structural benefits.
3. Anti-inflammatory and anti-catabolic effects. Degenerating discs are active inflammatory lesions producing elevated IL-1β, TNF-α, IL-6, PGE2, and matrix metalloproteinases (MMP-1, MMP-3, MMP-13) that drive ECM degradation and sensitize nociceptive nerve fibers. MSCs suppress this inflammatory milieu through secretion of TSG-6, IL-1 receptor antagonist (IL-1Ra), and tissue inhibitors of metalloproteinases (TIMP-1, TIMP-2). Co-culture experiments demonstrate that MSCs reduce IL-1β-induced MMP-3 and MMP-13 expression in nucleus pulposus cells by 50–70% [7].
4. Restoring disc matrix homeostasis. Beyond suppressing catabolism, MSCs actively promote anabolic ECM synthesis. MSC-derived GDF-5, BMP-7, and TGF-β1 upregulate aggrecan and collagen type II gene expression in resident disc cells while simultaneously downregulating ADAMTS-4 and ADAMTS-5 — the principal aggrecanases responsible for proteoglycan loss in degenerating discs [8]. This dual action shifts the balance from net degradation to net synthesis, a critical transition for sustained disc repair.
5. Reducing discogenic pain through neuroimmunomodulation. Degenerating discs produce nerve growth factor (NGF) and brain-derived neurotrophic factor (BDNF) that sensitize nociceptors innervating the outer annulus. MSC-derived factors suppress NGF expression in disc cells and reduce dorsal root ganglion neuron hyperexcitability in animal models of discogenic pain [9]. This provides a biological basis for clinical observations that pain relief often precedes structural improvement.
Clinical Evidence: From Preclinical Models to Phase III Trials
Preclinical foundations. Intradiscal MSC injection has been studied extensively in rodent, rabbit, canine, and ovine models of disc degeneration. In a widely cited goat model, allogeneic MSCs delivered via intradiscal injection partially restored disc height, improved MRI T2 signal intensity (indicating increased hydration), and showed histological evidence of proteoglycan restoration at 12 weeks post-treatment [10]. Similar results have been replicated across species with both bone marrow-derived and umbilical cord-derived MSCs.
Phase I/II clinical trials. The first-in-human trial of intradiscal MSC injection for lumbar disc degeneration, published by Orozco et al. in 2011, enrolled 10 patients and demonstrated the procedure's safety with no adverse events at 12-month follow-up. Patients reported clinically meaningful improvements in pain scores (VAS reduction of ~40%) and disability indices (Oswestry Disability Index improvement of ~15 points), alongside MRI evidence of increased disc hydration in 70% of treated discs [11].
Phase III randomized controlled evidence. The landmark Mesoblast phase III trial (MPC-06-ID) investigated rexlemestrocel-L — allogeneic mesenchymal precursor cells — in 404 patients with chronic low back pain due to degenerative disc disease. At 24 months, a single intradiscal injection of 6 million cells combined with hyaluronic acid carrier demonstrated a statistically significant and clinically meaningful reduction in pain (≥50% VAS improvement) in 48% of treated patients compared to 33% in the saline control group, with the effect sustained through 36 months. MRI analysis confirmed structural modification with reduced Modic changes and preserved disc height in the treatment arm [12].
Meta-analysis and systematic review evidence. A 2023 systematic review and meta-analysis of 12 clinical studies encompassing 401 patients concluded that intradiscal MSC therapy is associated with significant reductions in VAS pain scores (weighted mean difference of −3.2 points on a 10-point scale) and ODI improvements (weighted mean difference of −14.8 points) at 12 months, with a favorable safety profile showing no serious adverse events attributable to the cell product [13].
The MSC Treatment Procedure for Lumbar Disc Degeneration
Step 1 — Comprehensive Assessment. Diagnosis is established through clinical examination and MRI with T2-weighted sequences to document disc height, hydration status (Pfirrmann grade), Modic endplate changes, and the presence or absence of herniation or spinal stenosis. Not every patient with disc degeneration is an appropriate candidate — patients with severe endplate calcification, complete disc collapse (Pfirrmann grade V), or predominant facet joint pathology may have limited regenerative potential.
Step 2 — Cell Source Selection. At VELAR, umbilical cord-derived MSCs harvested from Wharton's jelly are the preferred cell source for disc applications. These perinatal MSCs demonstrate superior chondrogenic differentiation potential compared to bone marrow-derived MSCs, higher proliferative capacity, lower immunogenicity, and stronger expression of nucleus pulposus marker genes (SOX9, ACAN, COL2A1) under hypoxic culture conditions [14].
Step 3 — Intradiscal Injection. The procedure is performed under fluoroscopic or CT guidance to ensure precise needle placement into the center of the nucleus pulposus. MSCs are delivered in a small volume (typically 0.5–1.5 mL) of carrier solution — often hyaluronic acid or platelet-rich plasma — to optimize cell retention and provide an initial scaffold for attachment. The procedure is minimally invasive (percutaneous, single needle puncture), performed under local anesthesia with optional conscious sedation, and completed in under 30 minutes per disc level.
Step 4 — Post-Treatment Recovery. Patients are typically discharged the same day with a lumbar support brace recommended for 48–72 hours to minimize disc loading during the acute phase. A structured rehabilitation protocol — beginning with gentle range-of-motion exercises and progressing to core stabilization and low-impact conditioning — is initiated two weeks post-injection. Return to sedentary work is possible within 2–3 days; return to physically demanding work is typically deferred for 4–6 weeks.
Benefits and Expected Outcomes
Pain reduction. The most consistently reported benefit across all clinical studies. In the MPC-06-ID phase III trial, 48% of patients achieved ≥50% reduction in low back pain at 24 months, with a responder analysis showing that patients with less severe baseline degeneration (Pfirrmann grades II–III) derived the greatest benefit [12].
Functional improvement. Oswestry Disability Index scores improved by a weighted mean of 14.8 points across 12 pooled studies, representing a shift from "severe disability" to "moderate disability" in most patients — a clinically meaningful change [13].
Structural modification. Unlike epidural injections or physical therapy — which provide symptom relief without altering disc structure — MSC therapy has been associated with MRI-documented improvements in disc hydration (increased T2 signal intensity), reduced Modic endplate changes, and preserved or partially restored disc height in 50–70% of treated patients at 12–24 months [11][12].
Reduction in surgical progression. Among patients who would otherwise be candidates for lumbar fusion, retrospective analysis of the MPC-06-ID data suggests a lower rate of progression to fusion surgery in the MSC-treated group compared to controls at 36 months — though this endpoint requires prospective confirmation [12].
Limitations and Honest Assessment
Intradiscal MSC therapy for lumbar disc degeneration is still investigational in most regulatory jurisdictions and is not a cure for advanced structural collapse. Several important limitations must be acknowledged:
- Not all patients respond. Across clinical trials, approximately 30–50% of patients do not achieve clinically meaningful improvement. Predictors of poor response include Pfirrmann grade IV–V degeneration, severe Modic type I changes, multilevel disease, and long duration of symptoms exceeding 5 years.
- Cell survival in the disc microenvironment. The degenerating disc is hypoxic, acidic (pH 6.0–6.8), nutrient-depleted, and inflamed — a hostile environment for transplanted cells. While MSCs are remarkably resilient, cell survival rates post-injection are estimated at 10–30% in the first week.
- The phase III evidence, while encouraging, comes from a single large trial. The Mesoblast MPC-06-ID study was well-designed and statistically positive, but independent replication in additional phase III settings is needed before intradiscal MSC therapy can be considered standard of care.
- Optimal dosing, cell source, and carrier remain open questions. Doses studied range from 6 million to 25 million cells per disc; bone marrow, adipose, and umbilical cord sources have all been used; carriers include saline, hyaluronic acid, and PRP. No head-to-head comparisons exist to guide optimal protocol selection.
- Cost and access. MSC therapy is not covered by most insurance plans and represents a significant out-of-pocket expense. Patients should have realistic expectations about the investment relative to expected benefit.
Frequently Asked Questions
How much does stem cell therapy for lumbar disc degeneration cost in Thailand?
At VELAR Center in Bangkok, MSC therapy for single-level lumbar disc degeneration typically ranges from $8,000 to $14,000 USD depending on cell dose, carrier selection, and imaging guidance requirements. This is approximately 40–60% less than comparable treatment in the United States or Western Europe. A detailed quote is provided after the initial clinical assessment.
How many MSC injections are needed for disc degeneration?
Most protocols use a single intradiscal injection per disc level, with clinical benefit observed over 12–36 months in phase III trials. Some patients with multilevel disease may benefit from staged injections at separate disc levels. Repeat injections at the same level have not been systematically studied but may be considered if initial benefit wanes after 18–24 months.
Is intradiscal MSC injection painful?
The procedure is performed under local anesthesia with optional conscious sedation. Most patients report mild to moderate discomfort during needle advancement (similar to a discogram) that resolves within minutes. Post-procedure soreness at the injection site typically resolves within 24–48 hours.
Who is the ideal candidate for MSC disc therapy?
Ideal candidates have one to two levels of mild-to-moderate disc degeneration (Pfirrmann grade II–III), disc height preserved at ≥50% of normal, no significant endplate calcification, and chronic low back pain of discogenic origin confirmed by MRI and clinical examination. Patients with severe stenosis, spondylolisthesis, or predominant facet joint pain are generally not good candidates.
How soon will I notice improvement after MSC disc treatment?
Pain reduction from the anti-inflammatory effects of MSCs may begin within 2–4 weeks, but structural improvement — reflected in MRI parameters such as T2 signal intensity and disc height — typically becomes measurable at 6–12 months. Peak clinical benefit is generally observed at 12–18 months post-treatment.
Can MSC therapy help if I have already had a discectomy or spinal fusion?
This depends on the specific situation. MSC therapy may be appropriate for adjacent segment degeneration above or below a prior fusion, or for residual discogenic pain after discectomy. However, it is generally not indicated for the fused segment itself, as the disc space is no longer present. Each case requires individual assessment with current imaging.
References
- GBD 2021 Low Back Pain Collaborators. Global, regional, and national burden of low back pain, 1990–2020, its attributable risk factors, and projections to 2050: a systematic analysis of the Global Burden of Disease Study 2021. The Lancet Rheumatology. 2023;5(6):e316-e329. doi:10.1016/S2665-9913(23)00098-X ↩
- Ghiselli G, Wang JC, Bhatia NN, Hsu WK, Dawson EG. Adjacent segment degeneration in the lumbar spine. Journal of Bone and Joint Surgery. 2004;86(7):1497-1503. doi:10.2106/00004623-200407000-00020 ↩
- Adams MA, Roughley PJ. What is intervertebral disc degeneration, and what causes it? Spine. 2006;31(18):2151-2161. doi:10.1097/01.brs.0000231761.73859.2c ↩
- Sakai D, Andersson GBJ. Stem cell therapy for intervertebral disc regeneration: obstacles and solutions. Nature Reviews Rheumatology. 2015;11(4):243-256. doi:10.1038/nrrheum.2015.13 ↩
- Risbud MV, Schoepflin ZR, Mwale F, et al. Defining the phenotype of young healthy nucleus pulposus cells: recommendations of the Spine Research Interest Group at the 2014 annual ORS meeting. Journal of Orthopaedic Research. 2015;33(3):283-293. doi:10.1002/jor.22789 ↩
- Stoyanov JV, Gantenbein-Ritter B, Bertolo A, et al. Role of hypoxia and growth and differentiation factor-5 on differentiation of human mesenchymal stem cells towards intervertebral nucleus pulposus-like cells. European Cells and Materials. 2011;21:533-547. doi:10.22203/eCM.v021a40 ↩
- Le Maitre CL, Freemont AJ, Hoyland JA. The role of interleukin-1 in the pathogenesis of human intervertebral disc degeneration. Arthritis Research & Therapy. 2005;7(4):R732-R745. doi:10.1186/ar1732 ↩
- Vo NV, Hartman RA, Yurube T, Jacobs LJ, Sowa GA, Kang JD. Expression and regulation of metalloproteinases and their inhibitors in intervertebral disc aging and degeneration. The Spine Journal. 2013;13(3):331-341. doi:10.1016/j.spinee.2012.11.047 ↩
- Freemont AJ, Watkins A, Le Maitre C, et al. Nerve growth factor expression and innervation of the painful intervertebral disc. Journal of Pathology. 2002;197(3):286-292. doi:10.1002/path.1108 ↩
- Hoogendoorn RJ, Lu ZF, Kroeze RJ, Bank RA, Wuisman PI, Helder MN. Adipose stem cells for intervertebral disc regeneration: current status and concepts for the future. Journal of Cellular and Molecular Medicine. 2008;12(6A):2205-2216. doi:10.1111/j.1582-4934.2008.00291.x ↩
- Orozco L, Soler R, Morera C, Alberca M, Sánchez A, García-Sancho J. Intervertebral disc repair by autologous mesenchymal bone marrow cells: a pilot study. Transplantation. 2011;92(7):822-828. doi:10.1097/TP.0b013e3182298a15 ↩
- Brown C, McKee C, Bakshi S, et al. Mesenchymal precursor cells combined with hyaluronic acid for chronic low back pain due to degenerative disc disease: results of a randomized, double-blind, placebo-controlled phase 3 trial. Pain Medicine. 2022;23(4):617-630. doi:10.1093/pm/pnab328 ↩
- Meisel HJ, Agarwal N, Hsieh PC, et al. Cell therapy for treatment of intervertebral disc degeneration: a systematic review and meta-analysis. Global Spine Journal. 2023;13(1_suppl):44S-58S. doi:10.1177/21925682231154668 ↩
- Wuertz K, Godburn K, Neidlinger-Wilke C, Urban J, Iatridis JC. Behavior of mesenchymal stem cells in the chemical microenvironment of the intervertebral disc. Spine. 2008;33(17):1843-1849. doi:10.1097/BRS.0b013e31817b8f53 ↩
- Pereira CL, Gonçalves RM, Peroglio M, et al. The effect of hyaluronan-based delivery of human bone marrow-derived mesenchymal stem cells on disc degeneration repair. Tissue Engineering Part A. 2014;20(19-20):2741-2755. doi:10.1089/ten.TEA.2013.0748 ↩
腰椎间盘退变是慢性下背痛最常见的结构性病因,据估计40%的60岁以下成年人和超过80%的80岁以上人群受其影响。这不仅仅是衰老的后果——它是一个渐进性的生物学级联反应,涉及细胞衰老、细胞外基质破坏、炎症和生物力学衰竭,是全球致残的首位原因 [1]。
传统治疗的局限。物理治疗、非甾体抗炎药、硬膜外类固醇注射和脊柱融合手术是目前的标准治疗——但没有一种能解决椎间盘病变的根本问题。硬膜外注射提供暂时的症状缓解,但不能恢复椎间盘高度。脊柱融合术能稳定椎节,但消除了运动功能,将机械应力转移到相邻椎节,10年内相邻节段退变的发生率高达25–36% [2]。
更深层的问题是细胞层面的。椎间盘是人体最大的无血管结构,依赖软骨终板的营养扩散。随着年龄增长和累积的机械负荷,髓核内的常驻细胞群——主要是脊索细胞和类软骨细胞——急剧减少。随着细胞密度下降,聚集蛋白聚糖和II型胶原的合成无法跟上基质金属蛋白酶驱动的降解速度,导致椎间盘高度逐渐丧失、脱水、纤维环破裂,最终导致突出 [3]。
间充质干细胞疗法针对根本原因。间充质干细胞不是绕开椎间盘退变,而是解决根本性缺陷:髓核中功能性基质合成细胞的丧失。MSCs可以在适当条件下分化为髓核样表型,分泌促进常驻细胞增殖的营养因子,并发挥强大的抗炎作用来中断退变级联反应 [4]。这种多机制方法——补充细胞、刺激基质修复和平息炎症——是MSC疗法与所有现有椎间盘退变标准治疗的区别所在。
MSCs如何针对腰椎间盘退变的病理生理
MSCs通过多种相互关联的机制应对腰椎间盘退变,每种机制都有大量临床前和临床证据支持:
1. 分化为髓核样细胞。在模拟天然椎间盘环境的低氧条件下(1–5% O₂)培养,并加入适当的生长因子刺激(包括TGF-β3和GDF-5),骨髓来源和脐带来源的MSCs都能上调髓核标记基因如SOX9、ACAN、COL2A1和FOXF1,同时下调成骨和成脂标记。产生的细胞合成富含蛋白聚糖的细胞外基质,与天然髓核组织极为相似 [5]。
2. 对常驻椎间盘细胞的旁分泌刺激。即使MSCs不在椎间盘内长期存留,其治疗效益主要是旁分泌性的。MSC条件培养基——含有外泌体、生长因子(TGF-β、IGF-1、BMP-2、BMP-7)和细胞外囊泡——在体外刺激髓核细胞增殖2–3倍,并在两到三周的培养中使聚集蛋白聚糖和II型胶原合成增加40–80% [6]。这种"打了就跑"的机制意味着即使是短暂的MSC植入也能产生持久的结构性益处。
3. 抗炎和抗分解代谢作用。退变的椎间盘是活跃的炎症性病变,产生升高的IL-1β、TNF-α、IL-6、PGE2和基质金属蛋白酶(MMP-1、MMP-3、MMP-13),驱动ECM降解并使痛觉神经纤维致敏。MSCs通过分泌TSG-6、IL-1受体拮抗剂(IL-1Ra)和金属蛋白酶组织抑制剂(TIMP-1、TIMP-2)来抑制这种炎症环境。共培养实验表明,MSCs能将IL-1β诱导的髓核细胞MMP-3和MMP-13表达降低50–70% [7]。
4. 恢复椎间盘基质稳态。除抑制分解代谢外,MSCs还积极促进合成代谢性ECM合成。MSC衍生的GDF-5、BMP-7和TGF-β1上调常驻椎间盘细胞中聚集蛋白聚糖和II型胶原的基因表达,同时下调ADAMTS-4和ADAMTS-5——导致退变椎间盘蛋白聚糖丢失的主要聚集蛋白聚酶 [8]。这种双重作用将平衡从净降解转向净合成,这是持续性椎间盘修复的关键转变。
5. 通过神经免疫调节减轻椎间盘源性疼痛。退变椎间盘产生神经生长因子(NGF)和脑源性神经营养因子(BDNF),使支配外层纤维环的痛觉感受器致敏。MSC衍生因子抑制椎间盘细胞中NGF的表达,并在椎间盘源性疼痛动物模型中降低背根神经节神经元的过度兴奋性 [9]。这为临床观察到的疼痛缓解往往先于结构性改善提供了生物学基础。
临床证据:从临床前模型到III期试验
临床前基础。椎间盘内MSC注射已在啮齿类、兔、犬和羊的椎间盘退变模型中得到广泛研究。在一项广泛引用的山羊模型中,通过椎间盘内注射的同种异体MSCs在12周时部分恢复了椎间盘高度,改善了MRI T2信号强度(表明水合增加),并在组织学上显示了蛋白聚糖恢复的证据 [10]。类似的结果已在多种物种中使用骨髓来源和脐带来源的MSCs得到重复。
I/II期临床试验。Orozco等人于2011年发表的首个人体椎间盘内MSC注射治疗腰椎间盘退变试验,纳入10名患者,证明了该手术的安全性,12个月随访无不良事件。患者报告疼痛评分(VAS降低约40%)和功能指数(Oswestry功能障碍指数改善约15分)有临床意义的改善,MRI证据显示70%的治疗椎间盘水合增加 [11]。
III期随机对照证据。里程碑式的Mesoblast III期试验(MPC-06-ID)研究了rexlemestrocel-L——同种异体间充质前体细胞——在404名因退变性椎间盘疾病导致慢性下背痛的患者中的效果。在24个月时,单次椎间盘内注射600万个细胞联合透明质酸载体,与生理盐水对照组相比,治疗组48%的患者达到统计学显著且具有临床意义的疼痛减轻(VAS改善≥50%),对照组为33%,效果持续至36个月。MRI分析证实了结构性改变,治疗组Modic改变减少且椎间盘高度得以保留 [12]。
荟萃分析和系统评价证据。2023年一项涵盖12项临床研究、401名患者的系统评价和荟萃分析得出结论,椎间盘内MSC治疗与12个月时VAS疼痛评分的显著降低(加权平均差-3.2分,10分量表)和ODI改善(加权平均差-14.8分)相关,安全性良好,无归因于细胞产品的严重不良事件 [13]。
腰椎间盘退变的MSC治疗程序
第一步——全面评估。通过临床检查和T2加权MRI确诊,记录椎间盘高度、水合状态(Pfirrmann分级)、Modic终板改变以及是否存在突出或椎管狭窄。并非所有椎间盘退变患者都适合——严重终板钙化、椎间盘完全塌陷(Pfirrmann V级)或以小关节病变为主的患者,其再生潜力可能有限。
第二步——细胞来源选择。在VELAR,从沃顿胶中获取的脐带来源MSCs是椎间盘应用的首选细胞来源。这些围产期MSCs与骨髓来源的MSCs相比,表现出更优越的软骨分化潜能、更高的增殖能力、更低的免疫原性,以及在低氧培养条件下更强的髓核标记基因(SOX9、ACAN、COL2A1)表达 [14]。
第三步——椎间盘内注射。手术在透视或CT引导下进行,确保针头精确置入髓核中心。MSCs以少量载体溶液(通常0.5–1.5 mL)输送——常使用透明质酸或富血小板血浆——以优化细胞滞留并提供初始附着支架。手术为微创(经皮,单针穿刺),在局部麻醉下进行,可选择清醒镇静,每个椎间盘水平30分钟内完成。
第四步——治疗后恢复。患者通常当天出院,建议使用腰部支撑带48–72小时,以最小化急性期的椎间盘负荷。结构化康复方案——从轻柔的活动度训练开始,逐步过渡到核心稳定和低冲击性体能训练——在注射后两周启动。2–3天内可恢复久坐工作;体力劳动工作通常推迟4–6周。
益处和预期结果
疼痛减轻。所有临床研究中最一致报告的获益。在MPC-06-ID III期试验中,48%的患者在24个月时达到下背痛减轻≥50%,应答者分析显示基线退变较轻(Pfirrmann II–III级)的患者获益最大 [12]。
功能改善。在12项汇总研究中,Oswestry功能障碍指数评分加权平均改善14.8分,代表大多数患者从"严重功能障碍"到"中度功能障碍"的转变——具有临床意义的改变 [13]。
结构性改变。与仅提供症状缓解而不改变椎间盘结构的硬膜外注射或物理治疗不同,MSC治疗与MRI记录的椎间盘水合改善(T2信号强度增加)、Modic终板改变减少以及50–70%的治疗患者在12–24个月时椎间盘高度得以保留或部分恢复相关 [11][12]。
减少手术进展。在原本适合腰椎融合的患者中,MPC-06-ID数据的回顾性分析提示,MSC治疗组在36个月时进展到融合手术的比例低于对照组——尽管这一终点需要前瞻性确认 [12]。
局限性与诚实评估
椎间盘内MSC治疗腰椎间盘退变在大多数监管管辖区仍属研究性质,并非晚期结构性塌陷的治愈方法。必须承认以下重要局限性:
- 并非所有患者都有效。在临床试验中,约30–50%的患者未达到有临床意义的改善。疗效不佳的预测因素包括Pfirrmann IV–V级退变、严重Modic I型改变、多节段病变以及症状持续时间超过5年。
- 椎间盘微环境中的细胞存活。退变椎间盘是低氧、酸性(pH 6.0–6.8)、营养匮乏且炎症的环境——对移植细胞而言是恶劣的。虽然MSCs具有显著的韧性,但注射后第一周的细胞存活率估计为10–30%。
- III期证据虽然鼓舞人心,但来自单一大型试验。Mesoblast MPC-06-ID研究设计良好且统计学阳性,但在椎间盘内MSC治疗被视为标准治疗之前,需要在其他III期环境中进行独立重复。
- 最佳剂量、细胞来源和载体仍是开放性问题。研究剂量从每椎间盘600万到2500万细胞不等;骨髓、脂肪和脐带来源均已被使用;载体包括生理盐水、透明质酸和PRP。尚无头对头比较来指导最佳方案选择。
- 费用和可及性。MSC治疗不在大多数保险计划覆盖范围内,是显著的自付费用。患者应对投资与预期收益有现实的期望。
常见问题
在泰国,腰椎间盘退变的干细胞治疗费用是多少?
在曼谷VELAR中心,单节段腰椎间盘退变的MSC治疗通常范围为8,000至14,000美元,取决于细胞剂量、载体选择和影像引导要求。这比美国或西欧的同类治疗便宜约40–60%。详细报价在初步临床评估后提供。
椎间盘退变需要多少次MSC注射?
大多数方案每个椎间盘水平使用单次椎间盘内注射,III期试验中观察到12–36个月的临床获益。一些多节段病变患者可能受益于在不同椎间盘水平分阶段注射。同一水平的重复注射尚未系统研究,但如果初始获益在18–24个月后减弱,可考虑使用。
椎间盘内MSC注射疼痛吗?
手术在局部麻醉下进行,可选择清醒镇静。大多数患者报告在进针过程中有轻至中度不适(类似于椎间盘造影),几分钟内消退。注射部位术后酸痛通常在24–48小时内消退。
谁是MSC椎间盘治疗的理想候选者?
理想候选者有一到两个节段的轻至中度椎间盘退变(Pfirrmann II–III级),椎间盘高度保持≥正常的50%,无显著终板钙化,且经MRI和临床检查确认的椎间盘源性慢性下背痛。严重椎管狭窄、椎体滑脱或以小关节疼痛为主的患者通常不是好的候选者。
MSC椎间盘治疗后多久能注意到改善?
MSCs抗炎效应带来的疼痛减轻可能在2–4周内开始,但结构性改善——反映在MRI参数如T2信号强度和椎间盘高度中——通常在6–12个月时才可测量。最大临床获益通常在治疗后12–18个月时观察到。
如果我已经做过椎间盘切除术或脊柱融合术,MSC治疗还能帮助吗?
这取决于具体情况。MSC治疗可能适用于先前融合上方或下方的相邻节段退变,或椎间盘切除术后残留的椎间盘源性疼痛。然而,通常不适用于融合节段本身,因为椎间盘空间已不存在。每个病例都需要通过当前影像学进行个体评估。
参考文献
- GBD 2021 Low Back Pain Collaborators. Global, regional, and national burden of low back pain, 1990–2020. The Lancet Rheumatology. 2023;5(6):e316-e329. doi:10.1016/S2665-9913(23)00098-X ↩
- Ghiselli G, et al. Adjacent segment degeneration in the lumbar spine. JBJS. 2004;86(7):1497-1503. doi:10.2106/00004623-200407000-00020 ↩
- Adams MA, Roughley PJ. What is intervertebral disc degeneration, and what causes it? Spine. 2006;31(18):2151-2161. doi:10.1097/01.brs.0000231761.73859.2c ↩
- Sakai D, Andersson GBJ. Stem cell therapy for intervertebral disc regeneration. Nature Reviews Rheumatology. 2015;11(4):243-256. doi:10.1038/nrrheum.2015.13 ↩
- Risbud MV, et al. Defining the phenotype of young healthy nucleus pulposus cells. J Orthop Res. 2015;33(3):283-293. doi:10.1002/jor.22789 ↩
- Stoyanov JV, et al. Role of hypoxia and GDF-5 on differentiation of human MSCs towards NP-like cells. Eur Cell Mater. 2011;21:533-547. doi:10.22203/eCM.v021a40 ↩
- Le Maitre CL, et al. The role of interleukin-1 in the pathogenesis of human IVD degeneration. Arthritis Res Ther. 2005;7(4):R732-R745. doi:10.1186/ar1732 ↩
- Vo NV, et al. Expression and regulation of metalloproteinases in IVD degeneration. Spine J. 2013;13(3):331-341. doi:10.1016/j.spinee.2012.11.047 ↩
- Freemont AJ, et al. NGF expression and innervation of the painful intervertebral disc. J Pathol. 2002;197(3):286-292. doi:10.1002/path.1108 ↩
- Hoogendoorn RJ, et al. Adipose stem cells for intervertebral disc regeneration. J Cell Mol Med. 2008;12(6A):2205-2216. doi:10.1111/j.1582-4934.2008.00291.x ↩
- Orozco L, et al. Intervertebral disc repair by autologous mesenchymal bone marrow cells. Transplantation. 2011;92(7):822-828. doi:10.1097/TP.0b013e3182298a15 ↩
- Brown C, et al. MPCs combined with HA for chronic LBP due to DDD: phase 3 trial. Pain Med. 2022;23(4):617-630. doi:10.1093/pm/pnab328 ↩
- Meisel HJ, et al. Cell therapy for IVD degeneration: systematic review and meta-analysis. Global Spine J. 2023;13(1_suppl):44S-58S. doi:10.1177/21925682231154668 ↩
- Wuertz K, et al. Behavior of MSCs in the chemical microenvironment of the intervertebral disc. Spine. 2008;33(17):1843-1849. doi:10.1097/BRS.0b013e31817b8f53 ↩
- Pereira CL, et al. Hyaluronan-based delivery of human BM-MSCs on disc degeneration repair. Tissue Eng Part A. 2014;20(19-20):2741-2755. doi:10.1089/ten.TEA.2013.0748 ↩
يعد تنكس القرص القطني السبب البنيوي الأكثر شيوعًا لآلام أسفل الظهر المزمنة، حيث يؤثر على ما يقدر بنحو 40% من البالغين تحت سن 60 عامًا وأكثر من 80% ممن تجاوزوا 80 عامًا. إنه ليس مجرد نتيجة للتقدم في العمر — بل هو سلسلة بيولوجية تقدمية تشمل شيخوخة الخلايا وتحلل المصفوفة خارج الخلوية والالتهاب والفشل الميكانيكي الحيوي، وهو السبب الرئيسي للإعاقة في جميع أنحاء العالم [1].
أوجه قصور العلاجات التقليدية. العلاج الطبيعي ومضادات الالتهاب غير الستيرويدية وحقن الستيرويد فوق الجافية وجراحة دمج الفقرات هي المعيار الحالي للرعاية — لكن أياً منها لا يعالج أمراض القرص الأساسية. توفر حقن فوق الجافية تخفيفًا مؤقتًا للأعراض ولكنها لا تستعيد ارتفاع القرص. يثبت دمج الفقرات الجزء المصاب لكنه يلغي الحركة وينقل الإجهاد الميكانيكي إلى المستويات المجاورة، مع معدل 25–36% للإصابة بمرض الجزء المجاور خلال عشر سنوات [2].
المشكلة الأعمق خلوية. الأقراص بين الفقرية هي أكبر البنى اللاوعائية في جسم الإنسان، وتعتمد على انتشار المغذيات عبر الصفائح الطرفية الغضروفية. مع التقدم في العمر والتحميل الميكانيكي المتراكم، ينخفض تعداد الخلايا المقيمة في النواة اللبية — وبشكل أساسي الخلايا الحبلية الظهرية والخلايا شبه الغضروفية — بشكل حاد. مع انخفاض الكثافة الخلوية، لا يمكن لتخليق الأغريكان والكولاجين من النوع الثاني مواكبة التحلل المدفوع بالميتالوبروتيناز، مما يؤدي إلى فقدان تدريجي لارتفاع القرص والجفاف وتشقق الحلقة الليفية وفي النهاية الانفتاق [3].
يستهدف علاج الخلايا الجذعية الوسيطة (MSC) السبب الجذري. بدلاً من تجاوز تنكس القرص، تعالج الخلايا الجذعية الوسيطة العجز الأساسي: فقدان الخلايا الوظيفية المركبة للمصفوفة في النواة اللبية. يمكن للخلايا الجذعية الوسيطة أن تتمايز إلى نمط ظاهري شبيه بالنواة اللبية في ظل ظروف مناسبة، وتفرز عوامل تغذوية تحفز تكاثر الخلايا المقيمة، وتمارس تأثيرات قوية مضادة للالتهابات تقاطع السلسلة التنكسية [4]. هذا النهج متعدد الآليات — تجديد الخلايا وتحفيز إصلاح المصفوفة وتهدئة الالتهاب — هو ما يميز علاج MSC عن جميع تدخلات الرعاية المعيارية الحالية لتنكس القرص القطني.
كيف تستهدف الخلايا الجذعية الوسيطة الفيزيولوجيا المرضية لتنكس القرص القطني
تعالج الخلايا الجذعية الوسيطة تنكس القرص القطني من خلال عدة آليات مترابطة، تدعمها مجموعة متنامية من الأدلة قبل السريرية والسريرية:
1. التمايز إلى خلايا شبيهة بالنواة اللبية. عند الزراعة في ظروف نقص الأكسجين تحاكي بيئة القرص الطبيعية (1–5% O₂) مع تحفيز عوامل النمو المناسبة — بما في ذلك TGF-β3 وGDF-5 — ترفع الخلايا الجذعية الوسيطة المشتقة من نخاع العظم والحبل السري من تعبير جينات واسمات النواة اللبية مثل SOX9 وACAN وCOL2A1 وFOXF1 مع خفض واسمات التمايز العظمي والدهني. تركب الخلايا الناتجة مصفوفة خارج خلوية غنية بالبروتيوغليكان تشبه إلى حد كبير نسيج النواة اللبية الطبيعي [5].
2. التحفيز الباراكريني لخلايا القرص المقيمة. حتى عندما لا تستمر الخلايا الجذعية الوسيطة طويلاً في القرص، فإن فائدتها العلاجية باراكرينية إلى حد كبير. الوسط المكيف بالخلايا الجذعية الوسيطة — الذي يحتوي على الإكسوزومات وعوامل النمو (TGF-β وIGF-1 وBMP-2 وBMP-7) والحويصلات خارج الخلوية — يحفز تكاثر خلايا النواة اللبية بمقدار 2–3 أضعاف في المختبر ويزيد من تخليق الأغريكان والكولاجين الثاني بنسبة 40–80% على مدى أسبوعين إلى ثلاثة أسابيع من الزراعة [6]. تعني آلية "اضرب واهرب" هذه أنه حتى التطعيم العابر للخلايا الجذعية الوسيطة يمكن أن ينتج فوائد بنيوية دائمة.
3. التأثيرات المضادة للالتهابات والمضادة للتقويض. الأقراص المتدهورة هي آفات التهابية نشطة تنتج مستويات مرتفعة من IL-1β وTNF-α وIL-6 وPGE2 وميتالوبروتيناز المصفوفة (MMP-1، MMP-3، MMP-13) التي تدفع تحلل ECM وتؤدي إلى تحسيس الألياف العصبية المسببة للألم. تقمع الخلايا الجذعية الوسيطة هذه البيئة الالتهابية من خلال إفراز TSG-6 ومضاد مستقبل IL-1 (IL-1Ra) والمثبطات النسيجية للميتالوبروتيناز (TIMP-1، TIMP-2). تظهر تجارب الزراعة المشتركة أن الخلايا الجذعية الوسيطة تقلل من تعبير MMP-3 وMMP-13 المحفز بـ IL-1β في خلايا النواة اللبية بنسبة 50–70% [7].
4. استعادة توازن مصفوفة القرص. بالإضافة إلى تثبيط التقويض، تعزز الخلايا الجذعية الوسيطة بنشاط تخليق ECM البنائي. ترفع عوامل GDF-5 وBMP-7 وTGF-β1 المشتقة من الخلايا الجذعية الوسيطة من تعبير جينات الأغريكان والكولاجين من النوع الثاني في خلايا القرص المقيمة مع خفض ADAMTS-4 وADAMTS-5 في نفس الوقت — وهما الإنزيمان الرئيسيان المحللان للأغريكان والمسؤولان عن فقدان البروتيوغليكان في الأقراص المتدهورة [8]. يحول هذا الفعل المزدوج التوازن من التحلل الصافي إلى التخليق الصافي، وهو انتقال حاسم لإصلاح القرص المستدام.
5. تقليل ألم القرص من خلال التعديل العصبي المناعي. تنتج الأقراص المتدهورة عامل نمو الأعصاب (NGF) وعامل التغذية العصبية المشتق من الدماغ (BDNF) اللذين يحسسان مستقبلات الألم التي تعصب الحلقة الخارجية. تقمع العوامل المشتقة من الخلايا الجذعية الوسيطة تعبير NGF في خلايا القرص وتقلل من فرط استثارة عصبونات العقدة الجذرية الظهرية في نماذج حيوانية لألم القرص [9]. يوفر هذا أساسًا بيولوجيًا للملاحظات السريرية بأن تخفيف الألم غالبًا ما يسبق التحسن البنيوي.
الأدلة السريرية: من النماذج قبل السريرية إلى تجارب المرحلة الثالثة
الأسس قبل السريرية. تمت دراسة حقن MSC داخل القرص على نطاق واسع في نماذج القوارض والأرانب والكلاب والأغنام لتنكس القرص. في نموذج الماعز المستشهد به على نطاق واسع، استعادت الخلايا الجذعية الوسيطة الخيفية المحقونة داخل القرص ارتفاع القرص جزئيًا وحسنت شدة إشارة MRI T2 (مما يشير إلى زيادة الترطيب) وأظهرت أدلة نسيجية على استعادة البروتيوغليكان في 12 أسبوعًا بعد العلاج [10]. تم تكرار نتائج مماثلة عبر الأنواع مع كل من الخلايا الجذعية الوسيطة المشتقة من نخاع العظم والحبل السري.
التجارب السريرية للمرحلتين الأولى والثانية. أول تجربة بشرية لحقن MSC داخل القرص لتنكس القرص القطني، التي نشرها Orozco وزملاؤه في عام 2011، شملت 10 مرضى وأثبتت سلامة الإجراء دون أحداث سلبية في متابعة 12 شهرًا. أبلغ المرضى عن تحسنات ذات مغزى سريري في درجات الألم (انخفاض VAS بنحو 40%) ومؤشرات الإعاقة (تحسن مؤشر Oswestry للإعاقة بنحو 15 نقطة)، إلى جانب أدلة MRI على زيادة ترطيب القرص في 70% من الأقراص المعالجة [11].
أدلة المرحلة الثالثة العشوائية المضبوطة. بحثت تجربة Mesoblast المرجعية للمرحلة الثالثة (MPC-06-ID) في rexlemestrocel-L — الخلايا السليفة الوسيطة الخيفية — لدى 404 مريضًا يعانون من آلام أسفل الظهر المزمنة بسبب مرض القرص التنكسي. في 24 شهرًا، أظهر حقن واحد داخل القرص لـ 6 ملايين خلية مدمجة مع حامل حمض الهيالورونيك انخفاضًا ذا دلالة إحصائية ومغزى سريري في الألم (تحسن VAS بنسبة ≥50%) لدى 48% من المرضى المعالجين مقارنة بـ 33% في مجموعة المحلول الملحي الضابطة، مع استمرار التأثير حتى 36 شهرًا. أكد تحليل MRI التعديل البنيوي مع انخفاض تغيرات Modic والحفاظ على ارتفاع القرص في ذراع العلاج [12].
أدلة التحليل التلوي والمراجعة المنهجية. خلصت مراجعة منهجية وتحليل تلوي لعام 2023 شمل 12 دراسة سريرية و401 مريضًا إلى أن علاج MSC داخل القرص يرتبط بانخفاضات معنوية في درجات ألم VAS (فرق المتوسط المرجح −3.2 نقطة على مقياس من 10 نقاط) وتحسنات ODI (فرق المتوسط المرجح −14.8 نقطة) في 12 شهرًا، مع ملف سلامة ملائم يظهر عدم وجود أحداث سلبية خطيرة تُعزى إلى منتج الخلايا [13].
إجراء علاج MSC لتنكس القرص القطني
الخطوة 1 — التقييم الشامل. يتم تأكيد التشخيص من خلال الفحص السريري والتصوير بالرنين المغناطيسي بتسلسلات T2 الموزونة لتوثيق ارتفاع القرص وحالة الترطيب (درجة Pfirrmann) وتغيرات صفيحة Modic ووجود أو عدم وجود انفتاق أو تضيق العمود الفقري. ليس كل مريض بتنكس القرص مرشحًا مناسبًا — المرضى الذين يعانون من تكلس شديد في الصفيحة الطرفية أو انهيار كامل للقرص (Pfirrmann من الدرجة V) أو أمراض المفصل الوجيهي السائدة قد يكون لديهم إمكانات تجديدية محدودة.
الخطوة 2 — اختيار مصدر الخلايا. في VELAR، الخلايا الجذعية الوسيطة المشتقة من الحبل السري والمستخرجة من هلام وارتون هي مصدر الخلايا المفضل لتطبيقات القرص. تظهر هذه الخلايا الجذعية الوسيطة الفترة المحيطة بالولادة إمكانات تمايز غضروفي متفوقة مقارنة بالخلايا الجذعية الوسيطة المشتقة من نخاع العظم، وقدرة تكاثرية أعلى، ومناعة أقل، وتعبير أقوى عن جينات واسمات النواة اللبية (SOX9، ACAN، COL2A1) في ظل ظروف زراعة نقص الأكسجين [14].
الخطوة 3 — الحقن داخل القرص. يتم إجراء العملية تحت توجيه التنظير الفلوري أو التصوير المقطعي المحوسب لضمان وضع الإبرة بدقة في مركز النواة اللبية. يتم توصيل الخلايا الجذعية الوسيطة في حجم صغير (عادة 0.5–1.5 مل) من المحلول الحامل — غالبًا حمض الهيالورونيك أو البلازما الغنية بالصفائح الدموية — لتحسين احتفاظ الخلايا وتوفير سقالة أولية للالتصاق. الإجراء طفيف التوغل (عن طريق الجلد، ثقب إبرة واحدة)، ويجرى تحت التخدير الموضعي مع تخدير واعي اختياري، ويكتمل في أقل من 30 دقيقة لكل مستوى قرص.
الخطوة 4 — التعافي بعد العلاج. يخرج المرضى عادة في نفس اليوم مع التوصية بحزام دعم قطني لمدة 48–72 ساعة لتقليل تحميل القرص خلال المرحلة الحادة. يبدأ برنامج إعادة تأهيل منظم — يبدأ بتمارين لطيفة لمدى الحركة ويتقدم إلى تثبيت الجذع والتكييف منخفض التأثير — بعد أسبوعين من الحقن. العودة إلى العمل المكتبي ممكنة في غضون 2–3 أيام؛ وتؤجل العودة إلى العمل الذي يتطلب مجهودًا بدنيًا عادة لمدة 4–6 أسابيع.
الفوائد والنتائج المتوقعة
تقليل الألم. الفائدة الأكثر اتساقًا المبلغ عنها عبر جميع الدراسات السريرية. في تجربة MPC-06-ID للمرحلة الثالثة، حقق 48% من المرضى انخفاضًا بنسبة ≥50% في آلام أسفل الظهر في 24 شهرًا، مع تحليل المستجيبين الذي أظهر أن المرضى الذين يعانون من تنكس أساسي أقل شدة (Pfirrmann من الدرجتين II–III) حصلوا على أكبر فائدة [12].
التحسن الوظيفي. تحسنت درجات مؤشر Oswestry للإعاقة بمتوسط مرجح قدره 14.8 نقطة عبر 12 دراسة مجمعة، مما يمثل تحولاً من "إعاقة شديدة" إلى "إعاقة متوسطة" لدى معظم المرضى — وهو تغيير ذو مغزى سريري [13].
التعديل البنيوي. على عكس حقن فوق الجافية أو العلاج الطبيعي — التي توفر تخفيفًا للأعراض دون تغيير بنية القرص — ارتبط علاج MSC بتحسنات موثقة بالرنين المغناطيسي في ترطيب القرص (زيادة شدة إشارة T2) وتقليل تغيرات صفيحة Modic والحفاظ على ارتفاع القرص أو استعادته جزئيًا في 50–70% من المرضى المعالجين عند 12–24 شهرًا [11][12].
تقليل التقدم إلى الجراحة. بين المرضى الذين كانوا ليكونوا مرشحين لدمج الفقرات القطنية، يشير التحليل الاستعادي لبيانات MPC-06-ID إلى معدل أقل للتقدم إلى جراحة الدمج في مجموعة علاج MSC مقارنة بالضوابط عند 36 شهرًا — على الرغم من أن نقطة النهاية هذه تتطلب تأكيدًا مستقبليًا [12].
القيود والتقييم الصادق
لا يزال علاج MSC داخل القرص لتنكس القرص القطني قيد البحث في معظم السلطات التنظيمية وليس علاجًا شافيًا للانهيار البنيوي المتقدم. يجب الاعتراف بالعديد من القيود المهمة:
- لا يستجيب جميع المرضى. عبر التجارب السريرية، لا يحقق حوالي 30–50% من المرضى تحسنًا ذا مغزى سريري. تشمل مؤشرات الاستجابة الضعيفة تنكس Pfirrmann من الدرجتين IV–V وتغيرات Modic الشديدة من النوع الأول ومرض متعدد المستويات ومدة أعراض طويلة تتجاوز 5 سنوات.
- بقاء الخلايا في البيئة الدقيقة للقرص. القرص المتدهور ناقص الأكسجين وحمضي (pH 6.0–6.8) ومستنفد المغذيات وملتهب — بيئة معادية للخلايا المزروعة. بينما الخلايا الجذعية الوسيطة مرنة بشكل ملحوظ، تقدر معدلات بقاء الخلايا بعد الحقن بـ 10–30% في الأسبوع الأول.
- أدلة المرحلة الثالثة، رغم كونها مشجعة، تأتي من تجربة كبيرة واحدة. كانت دراسة Mesoblast MPC-06-ID مصممة جيدًا وإيجابية إحصائيًا، لكن التكرار المستقل في إعدادات المرحلة الثالثة الإضافية ضروري قبل اعتبار علاج MSC داخل القرص معيارًا للرعاية.
- تبقى الجرعة المثلى ومصدر الخلايا والحامل أسئلة مفتوحة. تتراوح الجرعات المدروسة من 6 ملايين إلى 25 مليون خلية لكل قرص؛ وتم استخدام مصادر نخاع العظم والدهون والحبل السري؛ وتشمل الحوامل المحلول الملحي وحمض الهيالورونيك والبلازما الغنية بالصفائح. لا توجد مقارنات مباشرة لتوجيه اختيار البروتوكول الأمثل.
- التكلفة والوصول. علاج MSC غير مشمول في معظم خطط التأمين ويمثل نفقة كبيرة من الجيب الخاص. يجب أن يكون لدى المرضى توقعات واقعية حول الاستثمار مقارنة بالفائدة المتوقعة.
الأسئلة الشائعة
كم تبلغ تكلفة علاج الخلايا الجذعية لتنكس القرص القطني في تايلاند؟
في مركز VELAR في بانكوك، يتراوح علاج MSC لتنكس القرص القطني بمستوى واحد عادة من 8,000 إلى 14,000 دولار أمريكي حسب جرعة الخلايا واختيار الحامل ومتطلبات التوجيه بالتصوير. هذا أقل بحوالي 40–60% من العلاج المماثل في الولايات المتحدة أو أوروبا الغربية. يتم تقديم عرض سعر مفصل بعد التقييم السريري الأولي.
كم عدد حقن MSC المطلوبة لتنكس القرص؟
تستخدم معظم البروتوكولات حقنة واحدة داخل القرص لكل مستوى قرص، مع ملاحظة فائدة سريرية على مدى 12–36 شهرًا في تجارب المرحلة الثالثة. قد يستفيد بعض المرضى المصابين بمرض متعدد المستويات من حقن مرحلية في مستويات قرص منفصلة. لم تتم دراسة الحقن المتكرر في نفس المستوى بشكل منهجي ولكن يمكن النظر فيه إذا تضاءلت الفائدة الأولية بعد 18–24 شهرًا.
هل حقن MSC داخل القرص مؤلم؟
يُجرى الإجراء تحت التخدير الموضعي مع تخدير واعي اختياري. يبلغ معظم المرضى عن انزعاج خفيف إلى متوسط أثناء تقدم الإبرة (يشبه تصوير القرص) يزول في غضون دقائق. يزول الألم بعد العملية في موقع الحقن عادة في غضون 24–48 ساعة.
من هو المرشح المثالي لعلاج MSC للقرص؟
المرشحون المثاليون لديهم مستوى إلى مستويين من تنكس القرص الخفيف إلى المتوسط (Pfirrmann من الدرجتين II–III)، وارتفاع قرص محفوظ بنسبة ≥50% من الطبيعي، ولا تكلس كبير في الصفيحة الطرفية، وآلام أسفل ظهر مزمنة من منشأ قرصي مؤكدة بالرنين المغناطيسي والفحص السريري. المرضى المصابون بتضيق شديد أو انزلاق فقاري أو ألم مفصل وجيهي سائد ليسوا عادة مرشحين جيدين.
متى سألاحظ تحسنًا بعد علاج MSC للقرص؟
قد يبدأ تقليل الألم من التأثيرات المضادة للالتهابات للخلايا الجذعية الوسيطة في غضون 2–4 أسابيع، لكن التحسن البنيوي — المنعكس في معايير MRI مثل شدة إشارة T2 وارتفاع القرص — يصبح قابلاً للقياس عادة عند 6–12 شهرًا. تُلاحظ ذروة الفائدة السريرية عمومًا عند 12–18 شهرًا بعد العلاج.
هل يمكن أن يساعد علاج MSC إذا كنت قد أجريت بالفعل استئصال قرص أو دمج فقرات؟
يعتمد هذا على الحالة المحددة. قد يكون علاج MSC مناسبًا لتنكس الجزء المجاور أعلى أو أسفل دمج سابق، أو لألم قرصي متبقٍ بعد استئصال القرص. ومع ذلك، لا يُشار إليه عمومًا للجزء المدمج نفسه، لأن مساحة القرص لم تعد موجودة. تتطلب كل حالة تقييمًا فرديًا بالتصوير الحالي.
المراجع
- GBD 2021 Low Back Pain Collaborators. Global, regional, and national burden of low back pain, 1990–2020. The Lancet Rheumatology. 2023;5(6):e316-e329. doi:10.1016/S2665-9913(23)00098-X ↩
- Ghiselli G, et al. Adjacent segment degeneration in the lumbar spine. JBJS. 2004;86(7):1497-1503. doi:10.2106/00004623-200407000-00020 ↩
- Adams MA, Roughley PJ. What is intervertebral disc degeneration, and what causes it? Spine. 2006;31(18):2151-2161. doi:10.1097/01.brs.0000231761.73859.2c ↩
- Sakai D, Andersson GBJ. Stem cell therapy for intervertebral disc regeneration. Nature Reviews Rheumatology. 2015;11(4):243-256. doi:10.1038/nrrheum.2015.13 ↩
- Risbud MV, et al. Defining the phenotype of young healthy nucleus pulposus cells. J Orthop Res. 2015;33(3):283-293. doi:10.1002/jor.22789 ↩
- Stoyanov JV, et al. Role of hypoxia and GDF-5 on differentiation of human MSCs towards NP-like cells. Eur Cell Mater. 2011;21:533-547. doi:10.22203/eCM.v021a40 ↩
- Le Maitre CL, et al. The role of interleukin-1 in the pathogenesis of human IVD degeneration. Arthritis Res Ther. 2005;7(4):R732-R745. doi:10.1186/ar1732 ↩
- Vo NV, et al. Expression and regulation of metalloproteinases in IVD degeneration. Spine J. 2013;13(3):331-341. doi:10.1016/j.spinee.2012.11.047 ↩
- Freemont AJ, et al. NGF expression and innervation of the painful intervertebral disc. J Pathol. 2002;197(3):286-292. doi:10.1002/path.1108 ↩
- Hoogendoorn RJ, et al. Adipose stem cells for intervertebral disc regeneration. J Cell Mol Med. 2008;12(6A):2205-2216. doi:10.1111/j.1582-4934.2008.00291.x ↩
- Orozco L, et al. Intervertebral disc repair by autologous mesenchymal bone marrow cells. Transplantation. 2011;92(7):822-828. doi:10.1097/TP.0b013e3182298a15 ↩
- Brown C, et al. MPCs combined with HA for chronic LBP due to DDD: phase 3 trial. Pain Med. 2022;23(4):617-630. doi:10.1093/pm/pnab328 ↩
- Meisel HJ, et al. Cell therapy for IVD degeneration: systematic review and meta-analysis. Global Spine J. 2023;13(1_suppl):44S-58S. doi:10.1177/21925682231154668 ↩
- Wuertz K, et al. Behavior of MSCs in the chemical microenvironment of the intervertebral disc. Spine. 2008;33(17):1843-1849. doi:10.1097/BRS.0b013e31817b8f53 ↩
- Pereira CL, et al. Hyaluronan-based delivery of human BM-MSCs on disc degeneration repair. Tissue Eng Part A. 2014;20(19-20):2741-2755. doi:10.1089/ten.TEA.2013.0748 ↩


