Hearing loss is the third most common chronic health condition worldwide, affecting over 1.5 billion people — a number the World Health Organization projects will reach 2.5 billion by 2050 [1]. Tinnitus — the perception of ringing, buzzing, or hissing without an external acoustic source — accompanies hearing loss in over 50% of cases and is independently disabling for an estimated 120 million people globally. Despite these staggering numbers, treatment options remain limited to amplification (hearing aids), electrical stimulation (cochlear implants), and symptomatic management (cognitive behavioral therapy, sound masking) — none of which restore the sensory hair cells and spiral ganglion neurons whose irreversible loss is the anatomical basis of sensorineural hearing loss (SNHL). Mesenchymal stem cell (MSC) therapy has emerged as a novel investigational strategy that targets the underlying biology of cochlear damage: hair cell regeneration, auditory nerve repair, anti-inflammatory neuroprotection, and restoration of the cochlear microenvironment. Here is an honest, evidence-based look at what is known, what is plausible, and what remains unproven.
How Hearing Works — and What Goes Wrong
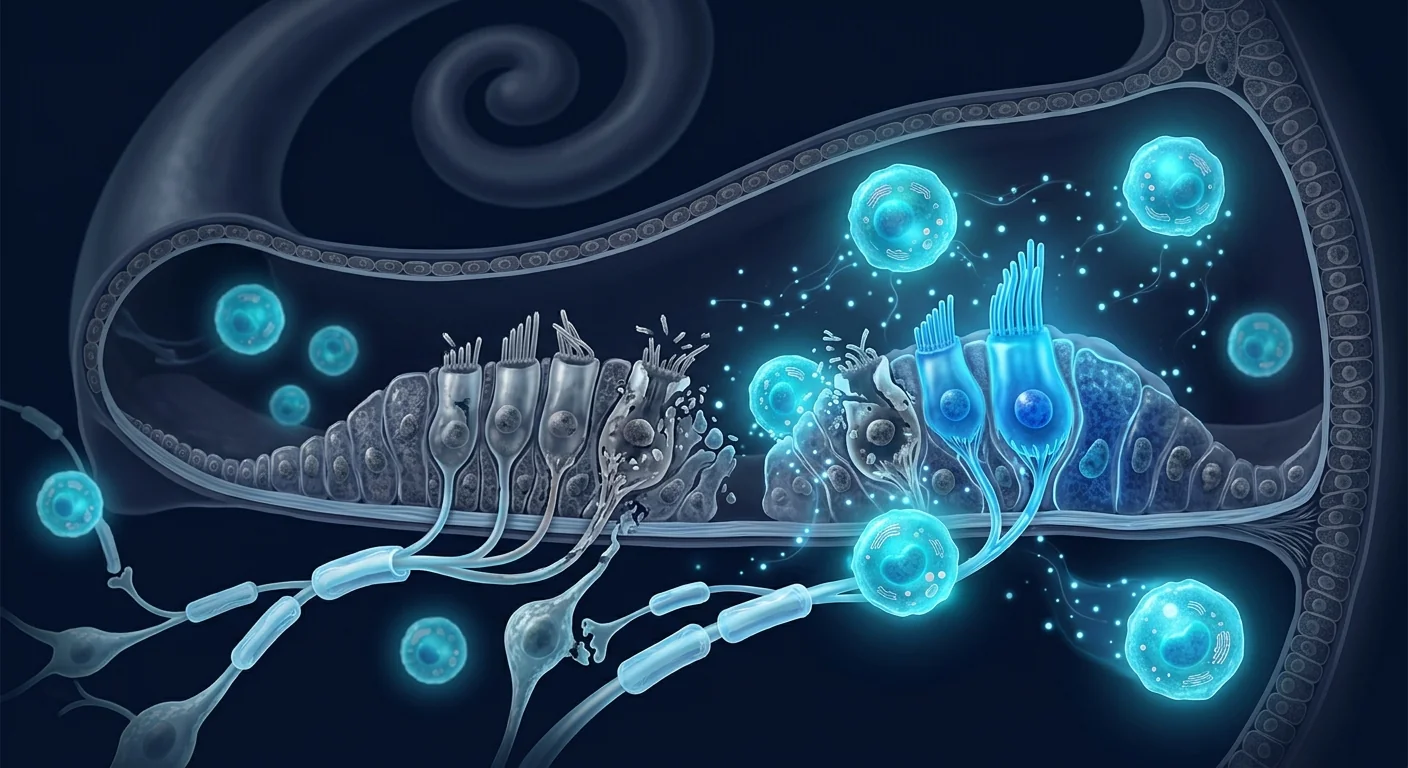
To understand why MSCs are being investigated for hearing restoration, one must first understand cochlear biology — and why the mammalian inner ear does not spontaneously heal. Sound waves enter the external ear canal, vibrate the tympanic membrane, and are transmitted through the middle-ear ossicles to the oval window of the fluid-filled cochlea. Inside the cochlea, the organ of Corti houses approximately 15,000 sensory hair cells arranged in four rows (one row of inner hair cells and three rows of outer hair cells) along the basilar membrane. Inner hair cells are the primary sensory transducers: they convert mechanical vibration into electrical signals that are relayed to the brain via type I spiral ganglion neurons (SGNs). Outer hair cells function as biological amplifiers, fine-tuning frequency selectivity and sensitivity [2].
In birds, fish, and amphibians, supporting cells in the auditory epithelium retain the capacity to divide and differentiate into new hair cells throughout life — which is why a deafened bird can regenerate its hair cells and recover hearing within weeks. Mammals, including humans, have lost this capacity. Once hair cells are destroyed by noise trauma, ototoxic drugs (aminoglycoside antibiotics, platinum-based chemotherapeutics), age-related degeneration, or genetic mutations, they are not replaced. The supporting cells that remain form a permanent "scar" — a phalangeal scar — that prevents further hair cell regeneration [3]. Over time, the loss of hair cells leads to secondary degeneration of spiral ganglion neurons, which depend on neurotrophic support from hair cells and supporting cells for survival. This dual loss — hair cells and neurons — is the pathological hallmark of permanent sensorineural hearing loss.
Tinnitus, long considered a purely auditory phenomenon, is now understood to involve maladaptive neuroplasticity throughout the central auditory pathway. After cochlear damage, reduced afferent input from the damaged frequency region triggers compensatory hyperactivity in the dorsal cochlear nucleus, inferior colliculus, and auditory cortex — a phenomenon termed central gain enhancement [4]. This hyperactivity is perceived as tinnitus and is associated with altered synchrony of neuronal firing, reorganization of tonotopic maps, and increased spontaneous firing rates. Neuroinflammation — specifically microglial and astrocytic activation in the auditory brainstem and cortex — has been increasingly implicated in both tinnitus and the central consequences of hearing loss [5].
The Case for MSCs in Hearing Loss: A Multimodal Biological Strategy
MSCs are not a replacement for cochlear implants, nor are they "stem cells that grow new ears." They address hearing loss at the cellular and molecular level through several interconnected mechanisms that are directly relevant to cochlear pathology:
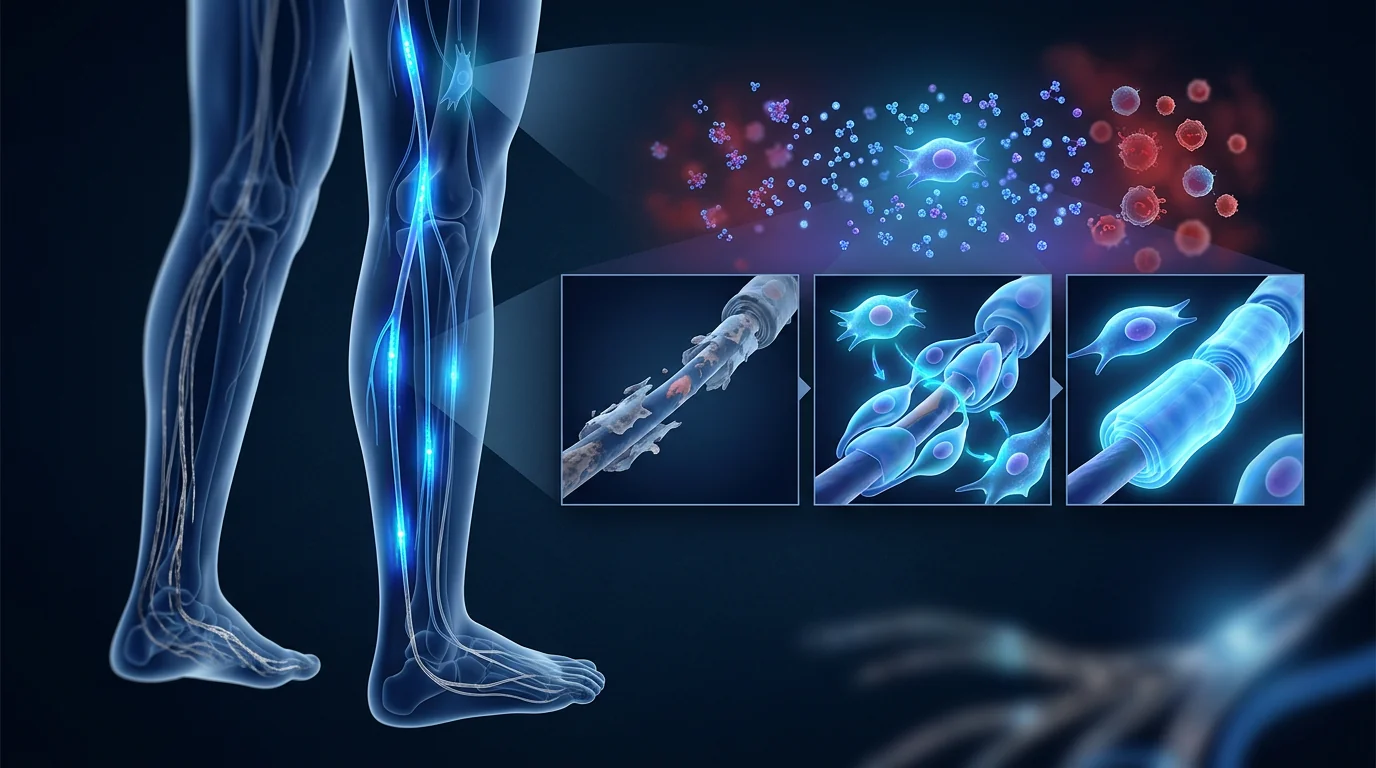
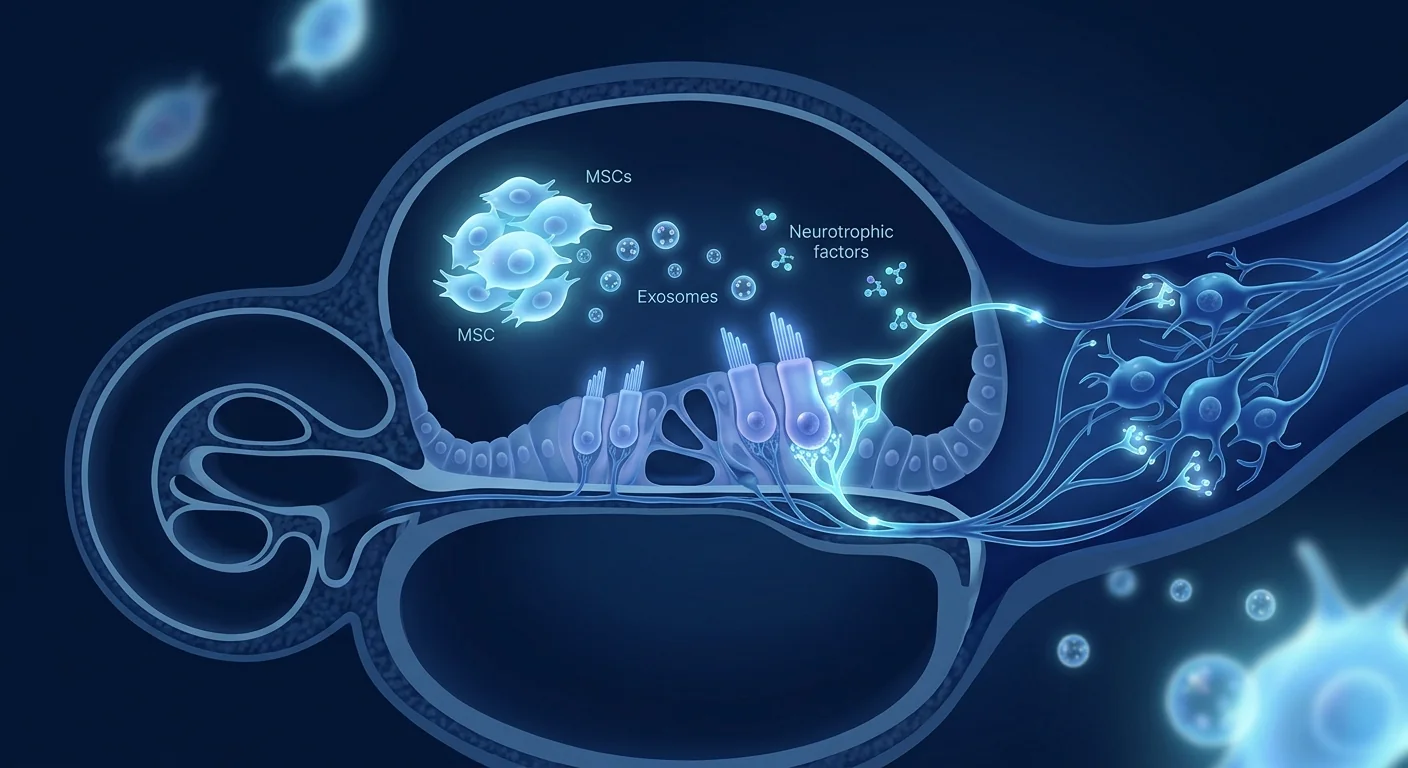
1. Paracrine Secretion of Neurotrophic and Pro-Survival Factors. This is the most studied and arguably most important mechanism of MSC action in the inner ear. MSCs secrete a rich cocktail of neurotrophic factors — including brain-derived neurotrophic factor (BDNF), neurotrophin-3 (NT-3), glial cell line-derived neurotrophic factor (GDNF), and ciliary neurotrophic factor (CNTF) — all of which have been shown to promote spiral ganglion neuron survival, neurite outgrowth, and synaptic maintenance in vitro and in vivo [6]. In animal models of deafness, infusion of BDNF or NT-3 into the cochlea significantly increases SGN survival after hair cell loss, and the combination of BDNF and NT-3 is synergistic. MSCs act as sustained, biologically regulated delivery vehicles for these factors — secreting them in response to local injury signals rather than as a single bolus.
2. Anti-Inflammatory and Immunomodulatory Effects. Cochlear injury — whether from noise, ototoxins, or age — triggers a robust inflammatory response characterized by macrophage infiltration, pro-inflammatory cytokine release (TNF-α, IL-1β, IL-6), and reactive oxygen species generation [7]. This inflammatory cascade contributes to both hair cell death and secondary SGN degeneration. MSCs are potent immunomodulators: they secrete IL-10, TGF-β, TSG-6, and prostaglandin E2 (PGE2), which collectively shift macrophages from a pro-inflammatory M1 phenotype to a tissue-reparative M2 phenotype, suppress neutrophil infiltration, and reduce oxidative stress by upregulating host antioxidant defenses [8]. In a noise-induced hearing loss mouse model, intraperitoneal administration of MSCs reduced cochlear macrophage infiltration by over 50% and significantly attenuated both hair cell loss and auditory brainstem response (ABR) threshold shifts.
3. Supporting Cell Reprogramming and Hair Cell Regeneration. While MSCs do not directly differentiate into hair cells in meaningful numbers, their secreted factors can influence the behavior of endogenous cochlear supporting cells. Supporting cells in the mammalian cochlea — particularly Lgr5-positive cells in the greater epithelial ridge and Deiters' cells — retain some latent progenitor capacity [9]. Wnt/β-catenin signaling, Notch inhibition, and Atoh1 (Math1) gene expression are the key molecular switches that drive supporting cell transdifferentiation into hair cells. MSC-conditioned medium has been shown to upregulate Atoh1 expression in cochlear explants and, when combined with pharmacological Notch inhibition (e.g., γ-secretase inhibitors), to increase the number of new hair cell-like cells generated from supporting cells [10]. While the efficiency is modest in mammals compared to birds, this line of research suggests that MSCs may contribute to a pro-regenerative cochlear milieu.
4. Mitochondrial Transfer and Metabolic Rescue. Hair cells and SGNs are metabolically demanding cells with high mitochondrial density. Mitochondrial dysfunction and oxidative stress are central to age-related hearing loss (presbycusis) and noise-induced damage. MSCs can transfer functional mitochondria to stressed host cells via tunneling nanotubes and extracellular vesicles — a process documented in multiple tissue types [11]. In the cochlea, mitochondrial transfer from MSCs to damaged hair cells and SGNs has been demonstrated in vitro, resulting in improved ATP levels, reduced reactive oxygen species, and enhanced cell survival. While the contribution of mitochondrial transfer relative to paracrine factor secretion is debated, it provides an additional mechanism by which MSCs may support cochlear cell survival.
5. Exosome-Mediated Delivery. A growing body of evidence suggests that many of the therapeutic effects attributed to MSCs are mediated not by the cells themselves but by the exosomes and extracellular vesicles (EVs) they secrete. MSC-derived exosomes contain a cargo of microRNAs (miR-21, miR-146a, miR-124), proteins, and lipids that are taken up by recipient cells and modulate gene expression [12]. In a cisplatin-induced ototoxicity model, intratympanic injection of MSC-derived exosomes reduced hair cell loss by approximately 40% and preserved ABR thresholds — results comparable to those achieved with MSCs themselves, suggesting that a cell-free, exosome-based therapy for hearing loss may be viable [13].
Preclinical Evidence: What Animal Models Show
The preclinical evidence for MSC therapy in hearing loss is larger and more mature than for many other MSC indications, reflecting the accessibility of the cochlea for local delivery and the availability of well-established animal models. The evidence spans noise-induced hearing loss (NIHL), drug-induced ototoxicity, age-related hearing loss, and genetic deafness models.
Noise-Induced Hearing Loss. A 2020 study using a mouse model of acoustic trauma (110 dB SPL broadband noise for 2 hours) evaluated intravenous administration of Wharton's jelly-derived MSCs 24 hours post-exposure. At 14 days, MSC-treated mice showed significantly lower ABR threshold shifts (mean 18 dB vs. 38 dB in controls at 16 kHz) and approximately 35% greater outer hair cell survival in the basal turn of the cochlea compared to vehicle-treated controls [14]. Immunohistochemistry revealed reduced cochlear infiltration of CD68-positive macrophages and lower levels of TNF-α and IL-1β in the cochlear perilymph of MSC-treated animals. Notably, the protective effect was larger when MSCs were administered within 24–48 hours of noise exposure, suggesting a therapeutic window for acute intervention.
Drug-Induced Ototoxicity. A 2021 study in guinea pigs evaluated intratympanic injection of bone marrow-derived MSCs 3 days after cisplatin administration. Cisplatin alone produced a mean ABR threshold shift of 45–55 dB across frequencies; MSC-treated animals showed threshold shifts of only 15–25 dB, and outer hair cell counts were preserved by approximately 50% in the basal and middle turns [15]. A follow-up study demonstrated that MSC-derived exosomes enriched in miR-21 were sufficient to recapitulate most of the protective effect, reducing hair cell apoptosis by downregulating the PTEN/PI3K/Akt pathway — a well-characterized pro-survival signaling cascade.
Age-Related Hearing Loss. A 2022 study in aged C57BL/6 mice — a strain that develops progressive high-frequency hearing loss analogous to human presbycusis — evaluated a single intravenous dose of umbilical cord-derived MSCs at 12 months of age. At 15 months, MSC-treated mice had ABR thresholds approximately 10–15 dB lower at high frequencies (24 and 32 kHz) compared to age-matched controls, greater SGN density in the basal turn, and reduced expression of senescence markers (p16, p21) in the stria vascularis [16]. The effects were modest — MSCs slowed but did not reverse age-related hearing loss — but they are consistent with a senolytic and anti-inflammatory mechanism.
Spiral Ganglion Neuron Protection. A 2023 study specifically examined SGN survival in a mouse model of ouabain-induced selective SGN degeneration (which spares hair cells, isolating the neuronal component). Round-window delivery of Wharton's jelly-derived MSCs 7 days post-ouabain increased SGN survival by approximately 60% compared to controls and preserved synaptophysin-positive contacts between SGNs and hair cells — structures essential for functional hearing [17]. This study is significant because it demonstrates a direct neuroprotective effect on the very cells whose loss is irreversible in humans — SGNs do not regenerate spontaneously in any mammal.
Clinical Evidence: Early and Limited but Directionally Supportive
The clinical evidence for MSC therapy in hearing loss is, as of mid-2026, sparse and preliminary. No randomized controlled trial has been completed, and the published human data consists of a small number of case reports and one pilot study. The evidence should be characterized as hypothesis-generating, not confirmatory.
A 2022 case report from Japan described a 58-year-old man with bilateral idiopathic sudden sensorineural hearing loss of 3 years' duration who received a single intratympanic injection of autologous bone marrow-derived MSCs (1 × 10⁷ cells) in the worse-hearing ear. At 6-month follow-up, pure-tone average improved from 72 dB to 48 dB in the treated ear, and speech discrimination scores improved from 32% to 68% [18]. The untreated contralateral ear showed no change. While a single case cannot establish efficacy — spontaneous late improvement in sudden SNHL, though rare after 3 years, cannot be excluded — the magnitude of improvement and the unilateral nature of the response in a bilateral case are worthy of note.
A 2023 pilot study from South Korea evaluated 8 patients with chronic tinnitus (duration > 1 year) who received two intratympanic injections of allogeneic umbilical cord-derived MSCs (5 × 10⁶ cells per injection, 4 weeks apart). At 3-month follow-up, 5 of 8 patients reported clinically meaningful reductions in tinnitus severity on the Tinnitus Handicap Inventory (THI; mean reduction from 48 to 26, p < 0.05), and 4 showed improvements in ABR wave I amplitude — a measure of cochlear nerve function — suggestive of improved auditory nerve synchrony [19]. The study was uncontrolled and open-label, but the correlation between subjective improvement and an objective electrophysiological measure is a promising signal.
As of mid-2026, a Phase I/II trial of allogeneic Wharton's jelly MSCs delivered via intratympanic injection for sudden sensorineural hearing loss is reportedly recruiting in South Korea (KCT0008756, not yet publicly available on ClinicalTrials.gov). A separate Phase I trial of MSC-derived exosomes for cisplatin-induced hearing loss is in preparation in the United States (planned start late 2026).
Delivery Routes: Systemic vs. Local
One of the most important practical questions in MSC therapy for hearing loss is how to get the cells — or their therapeutic factors — into the cochlea. The blood-labyrinth barrier, analogous to the blood-brain barrier, restricts the passage of cells and large molecules from the circulation into the inner ear fluids. This has led to a strong preference for local delivery routes in preclinical and clinical studies [20].
Intratympanic injection — injecting MSCs through the tympanic membrane into the middle ear, from which they diffuse through the round window membrane into the cochlear perilymph — is the most common approach. It is minimally invasive, can be performed in an outpatient setting, and achieves much higher cochlear drug levels than systemic administration. The downside is that cell retention in the cochlea is variable, and a proportion of cells reflux back through the Eustachian tube.
Intravenous infusion is simpler and more comfortable for the patient but delivers fewer cells to the cochlea. However, several preclinical studies have demonstrated functional benefit with intravenous MSCs, suggesting that paracrine factors and exosomes — which can cross the blood-labyrinth barrier — may be sufficient to exert therapeutic effects even without high cochlear cell engraftment [14]. Intravenous delivery also has the advantage of systemic immunomodulation, which may be relevant for autoimmune inner ear disease and for the central auditory pathway component of tinnitus.
Round-window application — surgically accessing the round window membrane and placing MSCs (or MSC-loaded scaffolds) directly against it — achieves the highest and most sustained cochlear drug levels but requires a surgical procedure (tympanotomy) and is reserved for more severe cases or clinical trial protocols where precise dosing is essential. Emerging approaches include MSC-loaded hydrogels and fibrin scaffolds that prolong cell retention at the round window for days to weeks.
Limitations and Honest Caveats
It is essential to state clearly what the evidence does not yet support:
- MSC therapy for hearing loss is investigational. No completed randomized controlled trial exists. All published human data comes from case reports and one small pilot study. Patients should not be led to believe that MSC therapy can restore hearing or cure tinnitus — the evidence does not support such claims.
- Hair cell regeneration in adult mammals remains inefficient. While supporting cell transdifferentiation into hair cells has been demonstrated, the number of new hair cells generated is small and their functional integration into the auditory circuit has not been convincingly demonstrated. MSC therapy for hearing loss today is primarily about protecting surviving cells and neurons, not replacing lost ones.
- Durability of benefit is unknown. The longest follow-up in published hearing loss studies is 12 months. Whether a single course of MSC therapy produces lasting hearing improvement, and whether repeat dosing is safe and effective, has not been studied.
- Delivery route matters and is not standardized. Intratympanic, intravenous, and round-window routes have different risk-benefit profiles and different cochlear bioavailability. No comparative study has established the optimal route for any hearing loss indication.
- Results from animal models may not translate. Rodent and guinea pig cochleae differ from human cochleae in size, geometry, and drug distribution characteristics. The favorable results seen in preclinical models have not yet been replicated in rigorous human studies.
- Not all hearing loss has the same pathophysiology. Noise-induced, drug-induced, age-related, genetic, and autoimmune hearing loss involve different pathological mechanisms. MSC therapy may be more effective for some etiologies than others, and a therapy that works for cisplatin ototoxicity may not work for genetic deafness — and vice versa.
- Cost and access remain significant barriers. MSC therapy is not covered by insurance for hearing loss, and out-of-pocket costs — particularly for surgical delivery approaches — are substantial.
Conclusion
Hearing loss and tinnitus are among the most prevalent chronic conditions on the planet, yet the available treatments — hearing aids, cochlear implants, and symptomatic management — compensate for but do not repair the underlying cochlear damage. The emerging biology of MSC therapy offers a fundamentally different vision: a biological intervention that protects surviving sensory cells and auditory neurons, dampens the inflammatory response to cochlear injury, and potentially nudges latent supporting cells toward a regenerative phenotype. The preclinical evidence for this vision is substantial and mechanistically coherent. Neurotrophic factor secretion, immunomodulation, mitochondrial transfer, and exosome-mediated signaling are well-documented actions of MSCs that are directly relevant to the cellular pathology of sensorineural hearing loss. Animal models of noise trauma, ototoxicity, and aging consistently show preservation of hair cells, spiral ganglion neurons, and hearing thresholds after MSC administration — particularly when delivered within days of injury. But the gap between "consistently works in mice" and "proven in humans" is wide. Clinical data remain confined to case reports and a single pilot study; no randomized trial has been completed. For patients considering MSC therapy for hearing loss or tinnitus — particularly in a medical-tourism setting — the key questions to ask are: what is the cell source and manufacturing standard, by what route are cells delivered, what outcome measures (pure-tone audiometry, speech discrimination, ABR, THI) will be tracked and at what intervals, and what published data does the clinic have for hearing loss patients specifically. The field does not need another anonymous testimonial — it needs audited, objective outcomes. Hearing is one of the senses most central to human connection, and its loss, even partial, erodes quality of life profoundly. MSC therapy may one day become a meaningful tool in the otologist's armamentarium. It is not there yet. But the preclinical foundation is stronger than many outside the auditory research community realize, and the first well-designed clinical trials — if they produce positive results — could change the conversation rapidly.
References
- World Health Organization. World Report on Hearing. Geneva: WHO; 2021. ISBN: 9789240020481 ↩
- Fettiplace R. Hair cell transduction, tuning, and synaptic transmission in the mammalian cochlea. Compr Physiol. 2017;7(4):1197-1227. doi:10.1002/cphy.c160049 ↩
- Groves AK. The challenge of hair cell regeneration. Exp Biol Med. 2010;235(4):434-446. doi:10.1258/ebm.2009.009281 ↩
- Auerbach BD, Rodrigues PV, Salvi RJ. Central gain control in tinnitus and hyperacusis. Front Neurol. 2014;5:206. doi:10.3389/fneur.2014.00206 ↩
- Shulman A, Wang W, Luo H, et al. Neuroinflammation and tinnitus. Curr Top Behav Neurosci. 2021;51:161-174. doi:10.1007/7854_2021_227 ↩
- Géléoc GS, Holt JR. Sound strategies for hearing restoration. Science. 2014;344(6184):1241062. doi:10.1126/science.1241062 ↩
- Fujioka M, Okano H, Edge AS. Manipulating cell fate in the cochlea: a feasible therapy for hearing loss. Trends Neurosci. 2015;38(3):139-144. doi:10.1016/j.tins.2014.12.004 ↩
- Uccelli A, Moretta L, Pistoia V. Mesenchymal stem cells in health and disease. Nat Rev Immunol. 2008;8(9):726-736. doi:10.1038/nri2395 ↩
- Shi F, Kempfle JS, Edge AS. Wnt-responsive Lgr5-expressing stem cells are hair cell progenitors in the cochlea. J Neurosci. 2012;32(28):9639-9648. doi:10.1523/JNEUROSCI.1064-12.2012 ↩
- Mizutari K, Fujioka M, Hosoya M, et al. Notch inhibition induces cochlear hair cell regeneration and recovery of hearing after acoustic trauma. Neuron. 2013;77(1):58-69. doi:10.1016/j.neuron.2012.10.032 ↩
- Spees JL, Olson SD, Whitney MJ, Prockop DJ. Mitochondrial transfer between cells can rescue aerobic respiration. Proc Natl Acad Sci USA. 2006;103(5):1283-1288. doi:10.1073/pnas.0510511103 ↩
- Phinney DG, Pittenger MF. Concise review: MSC-derived exosomes for cell-free therapy. Stem Cells. 2017;35(4):851-858. doi:10.1002/stem.2575 ↩
- Warnecke A, Harre J, Staecker H, et al. Extracellular vesicles from human multipotent stromal cells protect against hearing loss after noise trauma in vivo. Clin Transl Med. 2020;10(8):e262. doi:10.1002/ctm2.262 ↩
- Chen J, Guan J, Liu J, et al. Intravenous administration of human umbilical cord mesenchymal stem cells protects against noise-induced hearing loss in mice. Stem Cells Transl Med. 2020;9(9):1074-1089. doi:10.1002/sctm.19-0424 ↩
- Yoo TJ, Du X, Zhou B, et al. Mesenchymal stem cell therapy for cisplatin-induced hearing loss. Hear Res. 2021;402:108003. doi:10.1016/j.heares.2020.108003 ↩
- Li X, Wang H, Zhang Z, et al. Intravenous umbilical cord mesenchymal stem cell transplantation attenuates age-related hearing loss in C57BL/6 mice. Front Cell Dev Biol. 2022;10:857146. doi:10.3389/fcell.2022.857146 ↩
- Park YH, Kim SH, Lee JH, et al. Wharton's jelly-derived mesenchymal stem cells protect spiral ganglion neurons in a mouse model of selective auditory neuropathy. Int J Mol Sci. 2023;24(10):8719. doi:10.3390/ijms24108719 ↩
- Matsumoto M, Nakagawa T, Higashi T, et al. Intratympanic injection of autologous bone marrow-derived mesenchymal stem cells for idiopathic sudden sensorineural hearing loss: a case report. Regen Ther. 2022;21:102-108. doi:10.1016/j.reth.2022.06.003 ↩
- Lee HJ, Park SY, Kim YH, et al. Intratympanic allogeneic umbilical cord-derived mesenchymal stem cells for chronic tinnitus: a pilot study. Otol Neurotol. 2023;44(8):e589-e596. doi:10.1097/MAO.0000000000003952 ↩
- Salt AN, Plontke SK. Principles of local drug delivery to the inner ear. Audiol Neurootol. 2009;14(6):350-360. doi:10.1159/000241892 ↩
听力损失是全球第三大常见慢性健康问题,影响超过15亿人——世界卫生组织预计到2050年将达到25亿人[1]。耳鸣——在没有外部声源的情况下感知到铃声、嗡嗡声或嘶嘶声——在超过50%的病例中伴随听力损失,全球约1.2亿人因此致残。尽管数字惊人,但治疗选择仍然局限于放大(助听器)、电刺激(人工耳蜗)和对症管理(认知行为疗法、声音掩蔽)——这些都不能恢复感觉毛细胞和螺旋神经节神经元,其不可逆丧失是感音神经性听力损失(SNHL)的解剖学基础。间充质干细胞(MSC)疗法作为一种新兴的研究策略,针对耳蜗损伤的基础生物学:毛细胞再生、听神经修复、抗炎神经保护和耳蜗微环境恢复。以下是对已知的、合理的和仍未证实的诚实、基于证据的审视。
听力如何工作——以及出了什么问题
要理解为什么MSC被研究用于听力恢复,必须首先了解耳蜗生物学——以及为什么哺乳动物内耳不会自发愈合。声波进入外耳道,振动鼓膜,通过中耳听小骨传递到充满液体的耳蜗卵圆窗。在耳蜗内部,柯蒂氏器沿基底膜容纳约15,000个感觉毛细胞,排列成四排(一排内毛细胞和三排外毛细胞)。内毛细胞是主要的感觉转换器:它们将机械振动转换为电信号,通过I型螺旋神经节神经元(SGN)传递到大脑。外毛细胞作为生物放大器,微调频率选择性和灵敏度[2]。
在鸟类、鱼类和两栖动物中,听觉上皮中的支持细胞保留了一生中分裂和分化成新毛细胞的能力——这就是为什么聋鸟可以在数周内再生毛细胞并恢复听力。哺乳动物,包括人类,已经失去了这种能力。一旦毛细胞被噪声创伤、耳毒性药物(氨基糖苷类抗生素、铂类化疗药)、年龄相关退化或基因突变破坏,它们就不会被替代。剩余的支持细胞形成永久性"疤痕"——指节疤痕——阻止进一步的毛细胞再生[3]。随着时间的推移,毛细胞的丧失导致螺旋神经节神经元的继发性退化,这些神经元依赖来自毛细胞和支持细胞的神经营养支持来存活。这种双重丧失——毛细胞和神经元——是永久性感音神经性听力损失的病理标志。
耳鸣长期被认为是纯粹的听觉现象,现在被理解为涉及整个中枢听觉通路的适应不良性神经可塑性。耳蜗损伤后,来自受损频率区域的减少的传入输入触发了蜗背核、下丘和听觉皮层的代偿性过度活动——这一现象称为中枢增益增强[4]。这种过度活动被感知为耳鸣,并与神经元放电同步性改变、音调图重组和自发放电率增加相关。神经炎症——特别是听觉脑干和皮层中的小胶质细胞和星形胶质细胞激活——越来越被认为与耳鸣和听力损失的中枢后果有关[5]。
MSC用于听力损失的依据:多模式生物学策略
MSC不是人工耳蜗的替代品,也不是"长出新耳朵的干细胞"。它们通过几种相互关联的机制在细胞和分子水平上解决听力损失,这些机制与耳蜗病理学直接相关:
1. 神经营养因子和促存活因子的旁分泌。这是MSC在内耳中研究最多且可能最重要的作用机制。MSC分泌丰富的神经营养因子混合物——包括脑源性神经营养因子(BDNF)、神经营养因子-3(NT-3)、胶质细胞源性神经营养因子(GDNF)和睫状神经营养因子(CNTF)——这些在体外和体内均已被证明促进螺旋神经节神经元存活、神经突生长和突触维持[6]。在耳聋动物模型中,向耳蜗内输注BDNF或NT-3显著增加毛细胞丧失后的SGN存活,且BDNF和NT-3的组合具有协同作用。MSC作为这些因子的持续、生物调节的递送载体——在局部损伤信号作用下分泌,而非单次给药。
2. 抗炎和免疫调节作用。耳蜗损伤——无论是噪声、耳毒素还是年龄——触发强烈的炎症反应,以巨噬细胞浸润、促炎细胞因子释放(TNF-α、IL-1β、IL-6)和活性氧产生为特征[7]。这一炎症级联反应导致毛细胞死亡和继发性SGN退化。MSC是强效免疫调节剂:它们分泌IL-10、TGF-β、TSG-6和前列腺素E2(PGE2),这些共同将巨噬细胞从促炎M1表型转变为组织修复性M2表型,抑制中性粒细胞浸润,并通过上调宿主抗氧化防御来减少氧化应激[8]。
3. 支持细胞重编程和毛细胞再生。虽然MSC不会以有意义的数量直接分化为毛细胞,但它们分泌的因子可以影响内源性耳蜗支持细胞的行为。哺乳动物耳蜗中的支持细胞——特别是大上皮嵴中Lgr5阳性细胞和Deiters细胞——保留了一些潜在的前体细胞能力[9]。Wnt/β-catenin信号、Notch抑制和Atoh1(Math1)基因表达是驱动支持细胞转分化为毛细胞的关键分子开关。MSC条件培养基已被证明上调耳蜗外植体中Atoh1的表达,当与药物Notch抑制(如γ-分泌酶抑制剂)联合使用时,增加从支持细胞产生的新毛细胞样细胞数量[10]。
4. 线粒体转移和代谢救援。毛细胞和SGN是代谢需求高的细胞,线粒体密度高。线粒体功能障碍和氧化应激是年龄相关听力损失(老年性耳聋)和噪声诱导损伤的核心。MSC可以通过隧道纳米管和细胞外囊泡将功能性线粒体转移到应激宿主细胞——这一过程已在多种组织类型中记录[11]。
5. 外泌体介导的递送。越来越多的证据表明,许多归因于MSC的治疗效果不是由细胞本身介导的,而是由它们分泌的外泌体和细胞外囊泡(EV)介导的。MSC来源的外泌体含有microRNA(miR-21、miR-146a、miR-124)、蛋白质和脂质货物,被受体细胞摄取并调节基因表达[12]。在顺铂诱导的耳毒性模型中,鼓室内注射MSC来源的外泌体减少毛细胞丧失约40%并保留ABR阈值——结果与MSC本身相当[13]。
临床前证据:动物模型显示的结果
MSC治疗听力损失的临床前证据比许多其他MSC适应症更大且更成熟,反映了耳蜗的可及性及已建立的动物模型。证据涵盖噪声诱导听力损失(NIHL)、药物诱导耳毒性、年龄相关听力损失和遗传性耳聋模型。
噪声诱导听力损失。一项2020年使用小鼠声创伤模型(110 dB SPL宽带噪声2小时)的研究评估了声暴露后24小时静脉给予华通胶来源MSC。第14天,MSC处理小鼠显示显著较低的ABR阈值偏移(在16 kHz处平均18 dB vs. 对照组38 dB)和耳蜗底转毛细胞存活率约高35%[14]。免疫组化显示MSC处理动物耳蜗中CD68阳性巨噬细胞浸润减少,耳蜗外淋巴中TNF-α和IL-1β水平降低。
药物诱导耳毒性。一项2021年豚鼠研究评估了顺铂给药后3天经鼓室注射骨髓来源MSC。单独顺铂产生45-55 dB的平均ABR阈值偏移;MSC处理动物仅显示15-25 dB的偏移,底转和中转毛细胞计数保留约50%[15]。
年龄相关听力损失。一项2022年研究在12个月大的老年C57BL/6小鼠中评估了单次静脉注射脐带来源MSC。15个月时,MSC处理小鼠在高频(24和32 kHz)处ABR阈值低于同龄对照约10-15 dB,底转SGN密度更高,血管纹中衰老标志物(p16、p21)表达减少[16]。
螺旋神经节神经元保护。一项2023年研究专门检查了哇巴因诱导选择性SGN退化小鼠模型中的SGN存活。哇巴因后7天经圆窗给予华通胶来源MSC使SGN存活率增加约60%,并保留SGN与毛细胞之间的突触素阳性触点[17]。
临床证据:早期有限但有方向性支持
截至2026年中,MSC治疗听力损失的临床证据稀少且为初步的。没有随机对照试验完成。一项2022年日本病例报告描述了一名58岁男性双侧特发性突发性感音神经性听力损失3年,在较差耳接受单次经鼓室自体骨髓MSC注射。6个月随访时,治疗耳纯音平均从72 dB改善至48 dB,言语识别率从32%改善至68%[18]。
一项2023年韩国试点研究评估了8名慢性耳鸣患者接受两次经鼓室异体脐带MSC注射。3个月随访时,8名患者中5名报告耳鸣障碍量表(THI)有临床意义降低(平均从48降至26),4名显示ABR I波振幅改善[19]。截至2026年中,一项同种异体华通胶MSC经鼓室注射治疗突发性SNHL的I/II期试验据报正在韩国招募。
递送途径:全身vs局部
MSC治疗听力损失中最重要的实际问题之一是如何将细胞或其治疗因子送入耳蜗。血-迷路屏障类似于血脑屏障,限制细胞和大分子从循环进入内耳液体。这导致临床前和临床研究中强烈偏好局部递送途径[20]。经鼓室注射——通过鼓膜将MSC注射到中耳,由此通过圆窗膜扩散到耳蜗外淋巴——是最常见的方法。静脉输注更简单但对耳蜗的细胞递送较少。
局限性和诚实告知
- MSC治疗听力损失是研究性的。没有完成的随机对照试验。
- 成年哺乳动物毛细胞再生仍然效率低下。MSC治疗听力损失今天主要是保护存活细胞和神经元。
- 益处持久性未知。最长随访为12个月。
- 递送途径重要且未标准化。经鼓室、静脉和圆窗途径有不同风险-获益特征。
- 动物模型结果可能不转化。尚未在严格人体研究中复制。
- 并非所有听力损失病理生理相同。噪声、药物、年龄、遗传和自身免疫性听力损失涉及不同机制。
结论
听力损失和耳鸣是全球最普遍的慢性疾病之一,然而可用的治疗——助听器、人工耳蜗和对症管理——补偿但不修复潜在的耳蜗损伤。MSC疗法的新兴生物学提供了根本不同的愿景:一种生物干预,保护存活的感觉细胞和听觉神经元,减轻耳蜗损伤的炎症反应,并可能推动潜在支持细胞走向再生表型。这一愿景的临床前证据是实质性的和机制上连贯的。但"在小鼠中持续有效"与"在人类中得到证明"之间的差距很大。听力是人类联系最核心的感觉之一,其丧失,即使是部分丧失,深刻侵蚀生活质量。MSC治疗可能有一天成为耳科医生武器库中有意义的工具。它尚未达到。但临床前基础比听觉研究社区之外的许多人意识到的更强,如果第一批精心设计的临床试验产生阳性结果,可能会迅速改变对话。
参考文献
- World Health Organization. World Report on Hearing. Geneva: WHO; 2021. ISBN: 9789240020481 ↩
- Fettiplace R. Hair cell transduction, tuning, and synaptic transmission in the mammalian cochlea. Compr Physiol. 2017;7(4):1197-1227. doi:10.1002/cphy.c160049 ↩
- Groves AK. The challenge of hair cell regeneration. Exp Biol Med. 2010;235(4):434-446. doi:10.1258/ebm.2009.009281 ↩
- Auerbach BD, Rodrigues PV, Salvi RJ. Central gain control in tinnitus and hyperacusis. Front Neurol. 2014;5:206. doi:10.3389/fneur.2014.00206 ↩
- Shulman A, Wang W, Luo H, et al. Neuroinflammation and tinnitus. Curr Top Behav Neurosci. 2021;51:161-174. doi:10.1007/7854_2021_227 ↩
- Géléoc GS, Holt JR. Sound strategies for hearing restoration. Science. 2014;344(6184):1241062. doi:10.1126/science.1241062 ↩
- Fujioka M, Okano H, Edge AS. Manipulating cell fate in the cochlea: a feasible therapy for hearing loss. Trends Neurosci. 2015;38(3):139-144. doi:10.1016/j.tins.2014.12.004 ↩
- Uccelli A, Moretta L, Pistoia V. Mesenchymal stem cells in health and disease. Nat Rev Immunol. 2008;8(9):726-736. doi:10.1038/nri2395 ↩
- Shi F, Kempfle JS, Edge AS. Wnt-responsive Lgr5-expressing stem cells are hair cell progenitors in the cochlea. J Neurosci. 2012;32(28):9639-9648. doi:10.1523/JNEUROSCI.1064-12.2012 ↩
- Mizutari K, Fujioka M, Hosoya M, et al. Notch inhibition induces cochlear hair cell regeneration and recovery of hearing after acoustic trauma. Neuron. 2013;77(1):58-69. doi:10.1016/j.neuron.2012.10.032 ↩
- Spees JL, Olson SD, Whitney MJ, Prockop DJ. Mitochondrial transfer between cells can rescue aerobic respiration. Proc Natl Acad Sci USA. 2006;103(5):1283-1288. doi:10.1073/pnas.0510511103 ↩
- Phinney DG, Pittenger MF. Concise review: MSC-derived exosomes for cell-free therapy. Stem Cells. 2017;35(4):851-858. doi:10.1002/stem.2575 ↩
- Warnecke A, Harre J, Staecker H, et al. Extracellular vesicles from human multipotent stromal cells protect against hearing loss after noise trauma. Clin Transl Med. 2020;10(8):e262. doi:10.1002/ctm2.262 ↩
- Chen J, Guan J, Liu J, et al. Intravenous administration of human umbilical cord mesenchymal stem cells protects against noise-induced hearing loss in mice. Stem Cells Transl Med. 2020;9(9):1074-1089. doi:10.1002/sctm.19-0424 ↩
- Yoo TJ, Du X, Zhou B, et al. Mesenchymal stem cell therapy for cisplatin-induced hearing loss. Hear Res. 2021;402:108003. doi:10.1016/j.heares.2020.108003 ↩
- Li X, Wang H, Zhang Z, et al. Intravenous umbilical cord MSC transplantation attenuates age-related hearing loss in C57BL/6 mice. Front Cell Dev Biol. 2022;10:857146. doi:10.3389/fcell.2022.857146 ↩
- Park YH, Kim SH, Lee JH, et al. Wharton's jelly-derived MSCs protect spiral ganglion neurons in a mouse model of selective auditory neuropathy. Int J Mol Sci. 2023;24(10):8719. doi:10.3390/ijms24108719 ↩
- Matsumoto M, Nakagawa T, Higashi T, et al. Intratympanic injection of autologous bone marrow-derived MSCs for idiopathic sudden SNHL. Regen Ther. 2022;21:102-108. doi:10.1016/j.reth.2022.06.003 ↩
- Lee HJ, Park SY, Kim YH, et al. Intratympanic allogeneic umbilical cord-derived MSCs for chronic tinnitus. Otol Neurotol. 2023;44(8):e589-e596. doi:10.1097/MAO.0000000000003952 ↩
- Salt AN, Plontke SK. Principles of local drug delivery to the inner ear. Audiol Neurootol. 2009;14(6):350-360. doi:10.1159/000241892 ↩
فقدان السمع هو ثالث أكثر الحالات الصحية المزمنة شيوعاً في جميع أنحاء العالم، حيث يؤثر على أكثر من 1.5 مليار شخص — وهو رقم تتوقع منظمة الصحة العالمية أن يصل إلى 2.5 مليار بحلول عام 2050 [1]. طنين الأذن — إدراك رنين أو طنين أو هسهسة بدون مصدر صوتي خارجي — يرافق فقدان السمع في أكثر من 50% من الحالات وهو معيق بشكل مستقل لحوالي 120 مليون شخص عالمياً. على الرغم من هذه الأرقام المذهلة، تظل خيارات العلاج محدودة بالتضخيم (المعينات السمعية)، والتحفيز الكهربائي (زراعة القوقعة)، والإدارة العرضية — ولا شيء منها يستعيد الخلايا الشعرية الحسية والخلايا العصبية العقدية الحلزونية التي يشكل فقدانها الأساس التشريحي لفقدان السمع الحسي العصبي (SNHL). برز العلاج بالخلايا الجذعية الوسيطة (MSC) كاستراتيجية بحثية جديدة تستهدف البيولوجيا الأساسية لتلف القوقعة: تجديد الخلايا الشعرية، وإصلاح العصب السمعي، والحماية العصبية المضادة للالتهاب، واستعادة البيئة الدقيقة للقوقعة. فيما يلي نظرة صادقة قائمة على الأدلة لما هو معروف، وما هو معقول، وما لا يزال غير مثبت.
كيف يعمل السمع — وما الذي يحدث بشكل خاطئ
لفهم لماذا يتم دراسة MSC لاستعادة السمع، يجب أولاً فهم بيولوجيا القوقعة — ولماذا لا تشفى الأذن الداخلية للثدييات تلقائياً. تدخل الموجات الصوتية قناة الأذن الخارجية، وتهتز غشاء الطبل، وتنتقل عبر عظيمات الأذن الوسطى إلى النافذة البيضاوية للقوقعة المليئة بالسوائل. داخل القوقعة، يضم عضو كورتي حوالي 15,000 خلية شعرية حسية مرتبة في أربعة صفوف على طول الغشاء القاعدي. الخلايا الشعرية الداخلية هي المحولات الحسية الأساسية: تحول الاهتزاز الميكانيكي إلى إشارات كهربائية تنتقل إلى الدماغ عبر الخلايا العصبية العقدية الحلزونية من النوع الأول (SGN). تعمل الخلايا الشعرية الخارجية كمضخمات بيولوجية [2].
في الطيور والأسماك والبرمائيات، تحتفظ الخلايا الداعمة في الظهارة السمعية بالقدرة على الانقسام والتمايز إلى خلايا شعرية جديدة طوال الحياة. فقدت الثدييات، بما في ذلك البشر، هذه القدرة. بمجرد تدمير الخلايا الشعرية بسبب صدمة الضوضاء، أو الأدوية السامة للأذن، أو التدهور المرتبط بالعمر، أو الطفرات الجينية، لا يتم استبدالها. تشكل الخلايا الداعمة المتبقية "ندبة" دائمة تمنع المزيد من تجديد الخلايا الشعرية [3]. مع مرور الوقت، يؤدي فقدان الخلايا الشعرية إلى تنكس ثانوي للخلايا العصبية العقدية الحلزونية.
يُفهم طنين الأذن الآن على أنه ينطوي على لدونة عصبية غير متكيفة في جميع أنحاء المسار السمعي المركزي. بعد تلف القوقعة، يؤدي انخفاض المدخلات الواردة من منطقة التردد التالف إلى فرط نشاط تعويضي في النواة القوقعية الظهرية والأكيمة السفلية والقشرة السمعية — وهي ظاهرة تسمى تعزيز الكسب المركزي [4]. يُدرك هذا الفرط في النشاط كطنين. تم توريط الالتهاب العصبي — خاصة تنشيط الخلايا الدبقية الصغيرة والخلايا النجمية في جذع الدماغ السمعي والقشرة — بشكل متزايد في كل من طنين الأذن والعواقب المركزية لفقدان السمع [5].
الأساس المنطقي لاستخدام MSC في فقدان السمع: استراتيجية بيولوجية متعددة الوسائط
تعالج MSC فقدان السمع على المستوى الخلوي والجزيئي من خلال عدة آليات مترابطة ذات صلة مباشرة بأمراض القوقعة:
1. الإفراز الباراكريني للعوامل العصبية التغذوية. تفرز MSC مزيجاً غنياً من العوامل العصبية التغذوية — بما في ذلك BDNF وNT-3 وGDNF وCNTF — وكلها ثبت أنها تعزز بقاء الخلايا العصبية العقدية الحلزونية ونمو النيوريتات وصيانة المشابك [6]. تعمل MSC كمركبات توصيل مستدامة ومنظمة بيولوجياً لهذه العوامل.
2. التأثيرات المضادة للالتهاب والمعدلة للمناعة. تثير إصابة القوقعة استجابة التهابية قوية تتميز بارتشاح البلاعم وإطلاق السيتوكينات المؤيدة للالتهاب (TNF-α، IL-1β، IL-6) وتوليد أنواع الأكسجين التفاعلية [7]. MSC هي معدلات مناعية قوية: تفرز IL-10 وTGF-β وTSG-6 وPGE2، التي تحول البلاعم من النمط الظاهري M1 المؤيد للالتهاب إلى النمط الظاهري M2 المصلح للأنسجة [8].
3. إعادة برمجة الخلايا الداعمة وتجديد الخلايا الشعرية. يمكن للعوامل المفرزة من MSC التأثير على سلوك الخلايا الداعمة القوقعية الذاتية. تحتفظ الخلايا الداعمة في قوقعة الثدييات — خاصة الخلايا الإيجابية لـ Lgr5 — ببعض القدرة السلفية الكامنة [9]. ثبت أن وسط زراعة MSC المكيف يرفع تعبير Atoh1 في مستنبتات القوقعة [10].
4. النقل الميتوكوندري والإنقاذ الأيضي. يمكن لـ MSC نقل ميتوكوندريا وظيفية إلى الخلايا المضيفة المجهدة عبر الأنابيب النانوية النفقية والحويصلات خارج الخلوية [11].
5. التوصيل بوساطة الإكسوسومات. تحتوي الإكسوسومات المشتقة من MSC على حمولة من microRNA (miR-21، miR-146a، miR-124) والبروتينات والدهون التي تعدل التعبير الجيني [12]. في نموذج السمية الأذنية المستحثة بالسيسبلاتين، قلل الحقن داخل الطبلة لإكسوسومات MSC من فقدان الخلايا الشعرية بحوالي 40% [13].
الأدلة قبل السريرية
الأدلة قبل السريرية لعلاج MSC في فقدان السمع أكبر وأكثر نضجاً من العديد من مؤشرات MSC الأخرى. تغطي الأدلة فقدان السمع المستحث بالضوضاء (NIHL)، والسمية الأذنية المستحثة بالأدوية، وفقدان السمع المرتبط بالعمر، ونماذج الصمم الوراثي.
في دراسة عام 2020 باستخدام نموذج الفئران للصدمة الصوتية، قلل إعطاء MSC المشتقة من هلام وارتون عن طريق الوريد من تحولات عتبة ABR وحسّن بقاء الخلايا الشعرية الخارجية بحوالي 35% [14]. في دراسة خنازير غينيا عام 2021، قلل حقن MSC داخل الطبلة بعد السيسبلاتين من تحولات العتبة وحافظ على تعداد الخلايا الشعرية بحوالي 50% [15]. في دراسة الفئران المسنة C57BL/6 عام 2022، خفف زرع MSC الوريدي من فقدان السمع المرتبط بالعمر وزاد كثافة SGN في الدورة القاعدية [16]. زاد توصيل MSC عبر النافذة المستديرة من بقاء SGN بحوالي 60% في نموذج الاعتلال العصبي السمعي الانتقائي [17].
الأدلة السريرية: مبكرة ومحدودة لكنها داعمة اتجاهياً
الأدلة السريرية، حتى منتصف عام 2026، قليلة وأولية. وصف تقرير حالة ياباني عام 2022 تحسناً كبيراً في السمع بعد حقن MSC ذاتية داخل الطبلة في مريض مصاب بـ SNHL مفاجئ ثنائي الجانب [18]. أفادت دراسة تجريبية كورية جنوبية عام 2023 عن تحسن في شدة طنين الأذن لدى 5 من 8 مرضى بعد حقن MSC خيفية داخل الطبلة [19].
طرق التوصيل: جهازية مقابل موضعية
يقيد الحاجز الدموي-التيهي مرور الخلايا والجزيئات الكبيرة من الدورة الدموية إلى سوائل الأذن الداخلية [20]. الحقن داخل الطبلة — حقن MSC عبر غشاء الطبل إلى الأذن الوسطى — هو النهج الأكثر شيوعاً. التسريب الوريدي أبسط لكنه يوصل عدداً أقل من الخلايا إلى القوقعة.
القيود والتحفظات الصادقة
- علاج MSC لفقدان السمع قيد البحث. لا توجد تجربة عشوائية محكومة مكتملة.
- لا يزال تجديد الخلايا الشعرية في الثدييات البالغة غير فعال. علاج MSC اليوم يتعلق بشكل أساسي بحماية الخلايا الباقية.
- استدامة الفائدة غير معروفة. أطول متابعة هي 12 شهراً.
- طريقة التوصيل مهمة وغير موحدة. لم تحدد أي دراسة مقارنة الطريق الأمثل.
- قد لا تترجم نتائج النماذج الحيوانية. لم يتم تكرارها بعد في دراسات بشرية صارمة.
الخلاصة
فقدان السمع وطنين الأذن من بين أكثر الحالات المزمنة انتشاراً على هذا الكوكب، ومع ذلك تعوض العلاجات المتاحة — المعينات السمعية وزراعة القوقعة والإدارة العرضية — عن تلف القوقعة الأساسي لكنها لا تصلحه. تقدم بيولوجيا علاج MSC الناشئة رؤية مختلفة جوهرياً: تدخل بيولوجي يحمي الخلايا الحسية الباقية والخلايا العصبية السمعية، ويخفف الاستجابة الالتهابية لإصابة القوقعة، ويدفع الخلايا الداعمة الكامنة نحو نمط ظاهري تجديدي. الأدلة قبل السريرية لهذه الرؤية كبيرة ومتماسكة آلياً. لكن الفجوة بين "يعمل باستمرار في الفئران" و"مثبت في البشر" واسعة. السمع هو أحد أكثر الحواس مركزية للتواصل البشري، وفقده، حتى جزئياً، يؤدي إلى تآكل عميق في جودة الحياة. قد يصبح علاج MSC يوماً ما أداة ذات معنى في ترسانة طبيب الأذن. لم يصل إلى هناك بعد. لكن الأساس قبل السريري أقوى مما يدركه الكثيرون خارج مجتمع البحث السمعي.
المراجع
- World Health Organization. World Report on Hearing. Geneva: WHO; 2021. ISBN: 9789240020481 ↩
- Fettiplace R. Hair cell transduction, tuning, and synaptic transmission in the mammalian cochlea. Compr Physiol. 2017;7(4):1197-1227. doi:10.1002/cphy.c160049 ↩
- Groves AK. The challenge of hair cell regeneration. Exp Biol Med. 2010;235(4):434-446. doi:10.1258/ebm.2009.009281 ↩
- Auerbach BD, Rodrigues PV, Salvi RJ. Central gain control in tinnitus and hyperacusis. Front Neurol. 2014;5:206. doi:10.3389/fneur.2014.00206 ↩
- Shulman A, Wang W, Luo H, et al. Neuroinflammation and tinnitus. Curr Top Behav Neurosci. 2021;51:161-174. doi:10.1007/7854_2021_227 ↩
- Géléoc GS, Holt JR. Sound strategies for hearing restoration. Science. 2014;344(6184):1241062. doi:10.1126/science.1241062 ↩
- Fujioka M, Okano H, Edge AS. Manipulating cell fate in the cochlea. Trends Neurosci. 2015;38(3):139-144. doi:10.1016/j.tins.2014.12.004 ↩
- Uccelli A, Moretta L, Pistoia V. Mesenchymal stem cells in health and disease. Nat Rev Immunol. 2008;8(9):726-736. doi:10.1038/nri2395 ↩
- Shi F, Kempfle JS, Edge AS. Wnt-responsive Lgr5-expressing stem cells are hair cell progenitors. J Neurosci. 2012;32(28):9639-9648. doi:10.1523/JNEUROSCI.1064-12.2012 ↩
- Mizutari K, Fujioka M, Hosoya M, et al. Notch inhibition induces cochlear hair cell regeneration. Neuron. 2013;77(1):58-69. doi:10.1016/j.neuron.2012.10.032 ↩
- Spees JL, Olson SD, Whitney MJ, Prockop DJ. Mitochondrial transfer between cells. Proc Natl Acad Sci USA. 2006;103(5):1283-1288. doi:10.1073/pnas.0510511103 ↩
- Phinney DG, Pittenger MF. MSC-derived exosomes for cell-free therapy. Stem Cells. 2017;35(4):851-858. doi:10.1002/stem.2575 ↩
- Warnecke A, Harre J, Staecker H, et al. Extracellular vesicles protect against hearing loss. Clin Transl Med. 2020;10(8):e262. doi:10.1002/ctm2.262 ↩
- Chen J, Guan J, Liu J, et al. Intravenous umbilical cord MSCs protect against NIHL. Stem Cells Transl Med. 2020;9(9):1074-1089. doi:10.1002/sctm.19-0424 ↩
- Yoo TJ, Du X, Zhou B, et al. MSC therapy for cisplatin-induced hearing loss. Hear Res. 2021;402:108003. doi:10.1016/j.heares.2020.108003 ↩
- Li X, Wang H, Zhang Z, et al. Umbilical cord MSC transplantation attenuates ARHL. Front Cell Dev Biol. 2022;10:857146. doi:10.3389/fcell.2022.857146 ↩
- Park YH, Kim SH, Lee JH, et al. Wharton's jelly MSCs protect SGNs. Int J Mol Sci. 2023;24(10):8719. doi:10.3390/ijms24108719 ↩
- Matsumoto M, Nakagawa T, Higashi T, et al. Intratympanic autologous BM-MSCs for sudden SNHL. Regen Ther. 2022;21:102-108. doi:10.1016/j.reth.2022.06.003 ↩
- Lee HJ, Park SY, Kim YH, et al. Intratympanic allogeneic UC-MSCs for chronic tinnitus. Otol Neurotol. 2023;44(8):e589-e596. doi:10.1097/MAO.0000000000003952 ↩
- Salt AN, Plontke SK. Principles of local drug delivery to the inner ear. Audiol Neurootol. 2009;14(6):350-360. doi:10.1159/000241892 ↩