Chronic rhinosinusitis with nasal polyps (CRSwNP) affects approximately 4% of the adult population — roughly 300 million people worldwide — and is among the most debilitating chronic respiratory conditions. [1] Patients live with persistent nasal obstruction, anosmia, facial pressure, rhinorrhea, and sleep disruption that collectively reduce quality-of-life scores to levels comparable with congestive heart failure and COPD.
Where conventional treatment falls short. The current standard of care — intranasal corticosteroids, short-course systemic steroids, antibiotics for acute exacerbations, and endoscopic sinus surgery — provides symptom control rather than disease modification. Even with optimal medical therapy and surgery, polyp recurrence rates exceed 50% within 18 months, and up to 80% of patients require revision surgery within 5 years. [2] Biologics targeting IgE (omalizumab), IL-5 (mepolizumab), IL-4Rα (dupilumab), and IL-33 have changed the landscape for severe, refractory disease, but they require indefinite injections, cost upwards of USD 30,000–40,000 per year, and do not restore the structural tissue damage that chronic inflammation has already caused. [3]
The deeper problem is immunological. CRSwNP in Western populations is predominantly driven by type 2 inflammation — a coordinated immune response involving group 2 innate lymphoid cells (ILC2s), Th2 CD4⁺ T cells, eosinophils, mast cells, and the epithelial-derived alarmins IL-25, IL-33, and TSLP. [4] This cascade produces IL-4, IL-5, and IL-13, which drive eosinophil recruitment and survival, IgE class switching, goblet-cell metaplasia, and fibrin deposition — the histological hallmarks of nasal polyps. The airway epithelium itself is not a passive victim but an active participant, releasing alarmins that perpetuate the cycle. Steroids suppress symptoms but do not re-establish epithelial barrier integrity or reverse tissue remodeling.
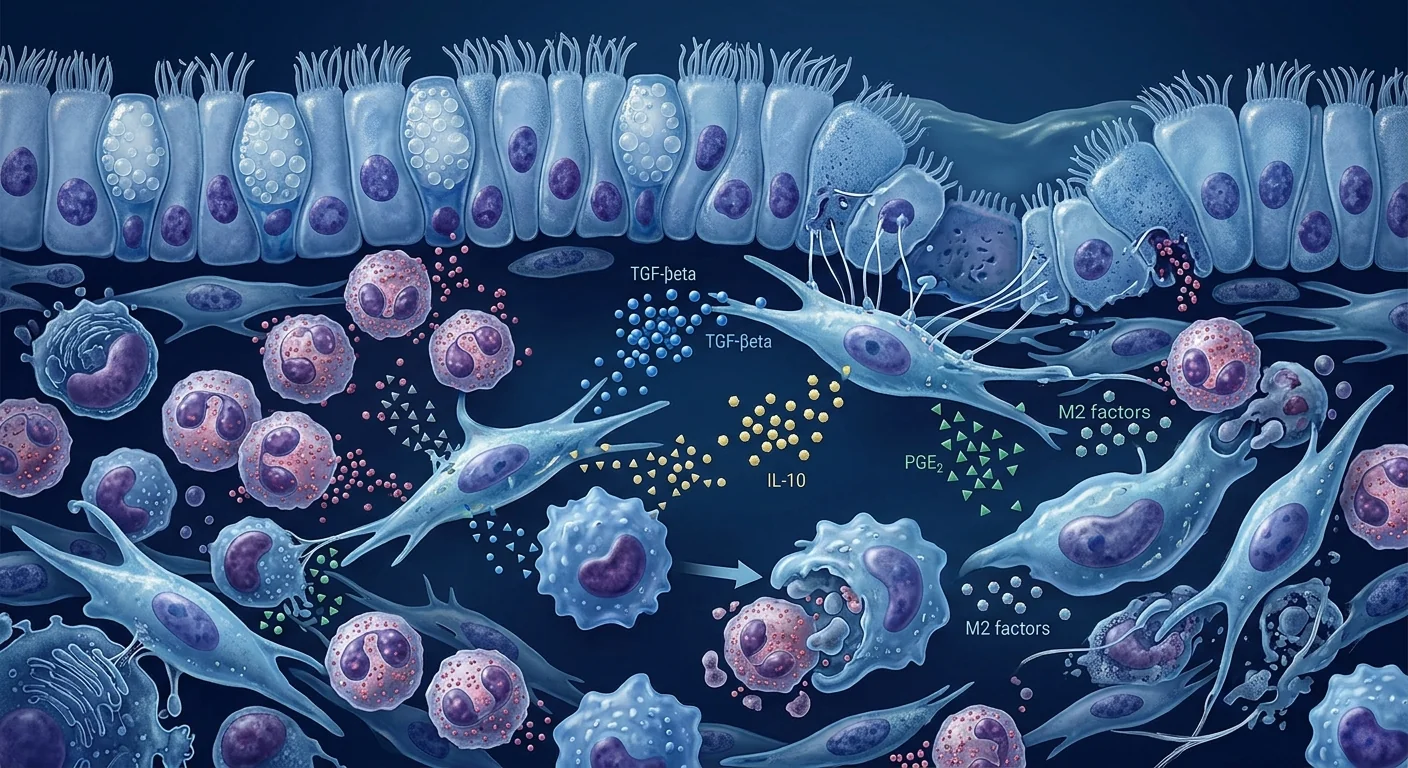
MSC therapy targets the inflammatory driver, not just the symptoms. Mesenchymal stem cells possess a unique portfolio of immunomodulatory capabilities that address multiple nodes of the type 2 inflammatory network simultaneously. MSCs secrete PGE2, TGF-β, IDO, TSG-6, and IL-10 — molecules that suppress Th2 polarization, induce regulatory T-cell (Treg) expansion, polarize macrophages from the inflammatory M1 to the reparative M2 phenotype, and directly inhibit eosinophil survival and activation. [5] Unlike biologics that block a single cytokine, MSCs deliver a network-level intervention that addresses the upstream drivers of polyp formation.
How MSC Therapy Works in Chronic Rhinosinusitis
MSC therapy restores immunological equilibrium in the sinonasal mucosa by suppressing type 2 inflammation, promoting epithelial repair, reprogramming macrophages, and directly inhibiting eosinophil-driven tissue damage. The therapeutic effect is mediated primarily through the paracrine secretome — a rich cocktail of growth factors, cytokines, extracellular vesicles, and antimicrobial peptides — rather than through long-term cellular engraftment.
Suppression of Type 2 Inflammation
The core pathology of CRSwNP is an exaggerated type 2 immune response centered on IL-4, IL-5, and IL-13. MSCs interrupt this cascade at multiple levels. MSC-derived PGE2 and TGF-β inhibit the differentiation of naïve CD4⁺ T cells into Th2 effector cells while simultaneously promoting FoxP3⁺ regulatory T-cell expansion. [7] IDO (indoleamine 2,3-dioxygenase) expressed by MSCs depletes local tryptophan, starving effector T cells and further favoring Treg dominance. TSG-6 (TNF-stimulated gene 6) dampens the activation of ILC2s — the tissue-resident alarmin-responsive cells that initiate the type 2 cascade at the epithelial level. [8]
Preclinical studies in murine models of allergic airway inflammation demonstrate that MSC infusion reduces bronchoalveolar lavage eosinophil counts by 60–80%, suppresses IL-4 and IL-13 production by lung-resident lymphocytes, and shifts the IL-10/IL-5 ratio decisively toward immune tolerance. [9] These findings, while primarily derived from lower-airway models, are directly relevant to the sinonasal cavity, which shares the same mucosal immune architecture.
Eosinophil Apoptosis and Clearance
Tissue eosinophilia is the histological hallmark of nasal polyps and a primary driver of epithelial damage, mucus hypersecretion, and tissue remodeling. MSCs have been shown to directly induce eosinophil apoptosis through secretion of pro-apoptotic signals while simultaneously enhancing macrophage-mediated efferocytosis — the clearance of apoptotic cells that, when impaired, leads to secondary necrosis and further inflammation. [10]
In an ovalbumin-challenged murine model of eosinophilic airway disease, a single intravenous dose of bone marrow-derived MSCs reduced eosinophil counts in lung tissue by 72% and airway eosinophils by 65% at 72 hours post-infusion. [9] The effect was mediated primarily through soluble factors, as MSC-conditioned medium alone reproduced approximately 80% of the anti-eosinophilic activity of whole-cell infusion.
Macrophage Polarization: M1 → M2 Shift
Nasal polyp tissue is characterized by a predominance of M1 (classically activated) macrophages that amplify inflammation through TNF-α, IL-1β, and reactive oxygen species production. MSCs secrete PGE2 and TSG-6, which reprogram macrophages toward the M2 (alternatively activated) phenotype. [11] M2 macrophages secrete IL-10 and TGF-β, clear apoptotic cells efficiently, and produce extracellular matrix components that aid tissue repair — functions that directly counteract the polyp microenvironment.
Epithelial Barrier Restoration
The sinonasal epithelium in CRSwNP exhibits reduced expression of tight-junction proteins (occludin, claudin-1, ZO-1), impaired ciliary function, and compromised mucociliary clearance. MSC-derived growth factors — specifically epidermal growth factor (EGF), keratinocyte growth factor (KGF/FGF-7), and hepatocyte growth factor (HGF) — stimulate epithelial proliferation, tight-junction reassembly, and ciliogenesis. [12]
MSC-derived extracellular vesicles have been shown to transfer functional mitochondria to injured epithelial cells via tunneling nanotubes — a mechanism that restores oxidative phosphorylation, reduces reactive oxygen species, and rescues cells from apoptosis. In an in vitro model of sinonasal epithelial injury, MSC-EV treatment increased transepithelial electrical resistance (a measure of barrier integrity) by 48% within 24 hours. [13]
Direct Modulation of Fibroblasts and Tissue Remodeling
Nasal polyps are not simply edematous outgrowths; they contain activated fibroblasts that deposit collagen, fibronectin, and cross-linked fibrin — transforming what should be a thin, functional mucosa into a stiff, obstructing mass. MSCs influence fibroblast behavior through paracrine TGF-β3 (which favors regenerative rather than scar-forming healing), through matrix metalloproteinase (MMP) regulation that remodels excess extracellular matrix, and through direct suppression of fibroblast-to-myofibroblast transition. [14]
Clinical Evidence and Current Research
The clinical evidence for MSC therapy in CRSwNP specifically is still nascent — there are no published Phase III trials and only a handful of early-phase studies. However, the broader evidence base from type 2 inflammatory airway diseases (allergic asthma, allergic rhinitis, eosinophilic esophagitis, atopic dermatitis) provides a compelling mechanistic rationale, and early CRSwNP-specific work is emerging. [15]
Preclinical models of nasal polyposis. A 2022 study using a murine model of eosinophilic nasal polyposis demonstrated that topically applied MSC-conditioned medium significantly reduced polyp size, eosinophil infiltration, and IL-5 expression in nasal mucosa. [16] Histological analysis showed restoration of pseudostratified ciliated epithelium in MSC-treated animals compared with persistent squamous metaplasia in controls.
Translation from asthma and allergic airway models. A 2024 systematic review and meta-analysis of 18 preclinical studies evaluating MSCs in allergic airway disease reported consistent and significant reductions in airway eosinophilia (standardized mean difference −2.1, p < 0.001), IL-4 levels (SMD −1.8, p < 0.001), and airway hyperresponsiveness (SMD −1.6, p < 0.001). [9] These outcomes — eosinophilia, type 2 cytokine levels, and tissue responsiveness — are directly relevant to CRSwNP pathophysiology.
Clinical studies in related conditions. A Phase I trial of intravenous allogeneic MSCs in moderate-to-severe allergic asthma (NCT03137199) enrolled 16 patients and demonstrated safety without serious adverse events, a significant reduction in circulating eosinophil counts at 12 weeks, and improved Asthma Control Test (ACT) scores. [17] While this trial was in lower-airway disease, it establishes the safety and immunomodulatory efficacy of systemic MSC therapy in human type 2 airway disease — a critical translational bridge to CRSwNP.
Intranasal delivery: a promising route for CRSwNP. The sinonasal cavity offers a unique therapeutic advantage: direct topical access. Unlike systemic conditions requiring intravenous delivery, CRSwNP can potentially be treated with intranasal MSC sprays, gels, or endoscopic injection — achieving high local concentrations while minimizing systemic exposure. A 2023 ex vivo study using human sinonasal tissue explants demonstrated that topical MSC-conditioned medium significantly reduced IL-5, IL-13, and eotaxin-3 secretion from polyp tissue within 48 hours. [18]
Treatment Protocol Considerations
While no standardized MSC protocol for CRSwNP has been established, the preclinical and translational evidence supports several guiding principles:
- Cell source matters. Wharton's jelly-derived MSCs (WJ-MSCs) and umbilical cord-derived MSCs (UC-MSCs) exhibit superior immunomodulatory potency compared to bone marrow-derived or adipose-derived MSCs, with higher secretion of PGE2, TGF-β, and IL-10. [19] For a type 2 inflammatory condition like CRSwNP, perinatal-source MSCs are the most rational choice.
- Delivery route considerations. Intravenous delivery provides systemic immunomodulation — relevant for patients with comorbid asthma, atopic dermatitis, or aspirin-exacerbated respiratory disease (AERD). Topical/intranasal delivery may offer higher local concentrations and is being investigated for isolated sinonasal disease. Combined IV + topical protocols are conceptually attractive but have not been formally studied.
- Timing relative to surgery. MSC therapy could be positioned in three clinical scenarios: (1) as a steroid-sparing alternative for patients refusing or ineligible for surgery, (2) as an adjunct at the time of endoscopic sinus surgery to promote regenerative healing and reduce recurrence, or (3) as salvage therapy for patients with recurrent polyps despite surgery + maximal medical therapy. Each scenario implies a different dosing strategy and evidence threshold.
- Dosing considerations. Based on data from systemic inflammatory conditions, intravenous doses of 1–2 × 10⁶ cells/kg are typical. Topical dosing for sinonasal application has not been standardized, but ex vivo studies suggest concentrations of 1–5 × 10⁶ cells/mL in gel or suspension form achieve meaningful paracrine effects within 48 hours.
Realistic Expectations and Limitations
What early evidence suggests patients might expect:
- Reduction in sinonasal inflammatory burden, potentially measurable as decreased nasal nitric oxide, reduced eosinophil cationic protein in nasal lavage, or improved patient-reported symptom scores.
- Potential reduction in polyp size and/or recurrence rate when used as an adjunct to surgery — this is the most clinically plausible application based on the epithelial repair and anti-fibrotic mechanisms described above.
- Improvement in comorbid type 2 conditions (asthma, atopic dermatitis, AERD) if systemic delivery is used — a "multi-organ" benefit that no single biologic currently provides.
- Timeline: immunomodulatory effects (cytokine shifts, eosinophil reduction) are typically measurable within 2–4 weeks; structural changes (polyp regression, epithelial restoration) require 8–16 weeks; maximal benefit may take 3–6 months.
What MSC therapy is unlikely to do:
- It will not replace surgery for large, obstructing polyps that require mechanical debulking — these are structural problems requiring structural solutions.
- It will not normalize anosmia of many years' duration if the olfactory epithelium has undergone irreversible squamous metaplasia — chronic damage has limits.
- It does not eliminate the underlying genetic or environmental predisposition to type 2 inflammation — it modulates the immune environment, it does not rewrite the genome.
Frequently Asked Questions
How much does stem cell therapy for chronic sinusitis cost in Thailand?
MSC therapy costs at VELAR Center in Bangkok vary based on protocol complexity, cell dose, and delivery route. A detailed cost estimate is provided after clinical evaluation. Thailand offers significant cost advantages compared to equivalent treatment in North America or Western Europe, typically 40–60% less while maintaining international standards of laboratory quality and clinical care.
Is MSC therapy safe for patients with aspirin-exacerbated respiratory disease (AERD)?
The safety profile of MSCs in type 2 inflammatory conditions is favorable — MSCs are inherently anti-inflammatory and do not trigger mast-cell degranulation or cyclooxygenase-dependent pathways involved in AERD reactions. However, AERD patients should be evaluated comprehensively, as they represent a more severe disease phenotype that may require combined medical and cell-based approaches.
Can MSC therapy restore the sense of smell lost to chronic sinusitis?
Olfactory recovery is one of the most clinically meaningful but least predictable outcomes. If anosmia is due to conductive blockage (polyps physically obstructing the olfactory cleft), polyp reduction may restore airflow and smell. If it is due to sensorineural damage (olfactory neuron loss from chronic inflammation), the evidence for MSC-mediated neuronal regeneration in humans is preliminary. Early intervention — before years of irreversible damage accumulate — offers the best chance.
How does MSC therapy compare to biologic drugs like dupilumab for nasal polyps?
Biologics (dupilumab, mepolizumab, omalizumab) are FDA-approved for severe CRSwNP and demonstrate 50–60% reduction in Nasal Polyp Score in landmark trials. They require ongoing injections (every 2–4 weeks) at an annual cost of USD 30,000–40,000. MSC therapy, while still investigational, may offer complementary advantages: (1) potential for tissue repair (biologics suppress inflammation but do not rebuild tissue), (2) a single or short-course treatment protocol vs. indefinite injections, and (3) multi-organ benefit if systemic delivery is used. The two approaches are not mutually exclusive and may ultimately be synergistic.
How many MSC treatments are needed for chronic sinusitis?
The optimal number and interval of MSC treatments for CRSwNP have not been established. Based on experience with other chronic inflammatory conditions, a single infusion may provide 6–12 months of immunomodulatory benefit, with booster doses considered based on clinical response. A protocol involving an initial 2–3 treatments over 3–6 months, followed by reassessment, is typical for investigational applications.
Can I have MSC therapy if I've already had multiple sinus surgeries?
Yes — in fact, patients with recurrent polyps despite multiple surgeries are the population for whom MSC therapy may offer the greatest value. Previous surgery creates a modified anatomical environment that does not preclude MSC delivery. The key consideration is whether viable mucosa remains to respond to regenerative signals — a question best assessed through endoscopic examination and CT imaging during your consultation.
References
- Fokkens WJ, Lund VJ, Hopkins C, et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2020. Rhinology. 2020;58(Suppl S29):1-464. doi:10.4193/Rhin20.600 ↩
- DeConde AS, Mace JC, Levy JM, Rudmik L, Alt JA, Smith TL. Prevalence of polyp recurrence after endoscopic sinus surgery for chronic rhinosinusitis with nasal polyposis. Laryngoscope. 2017;127(3):550-555. doi:10.1002/lary.26191 ↩
- Bachert C, Han JK, Desrosiers M, et al. Efficacy and safety of dupilumab in patients with severe chronic rhinosinusitis with nasal polyps (LIBERTY NP SINUS-24 and LIBERTY NP SINUS-52): results from two multicentre, randomised, double-blind, placebo-controlled, parallel-group phase 3 trials. Lancet. 2019;394(10209):1638-1650. doi:10.1016/S0140-6736(19)31881-1 ↩
- Kato A, Peters AT, Stevens WW, Schleimer RP, Tan BK, Kern RC. Endotypes of chronic rhinosinusitis: relationships to disease phenotypes, pathogenesis, clinical findings, and treatment approaches. Allergy. 2022;77(3):812-826. doi:10.1111/all.15074 ↩
- Shi Y, Wang Y, Li Q, et al. Immunoregulatory mechanisms of mesenchymal stem and stromal cells in inflammatory diseases. Nature Reviews Nephrology. 2018;14(8):493-507. doi:10.1038/s41581-018-0023-5 ↩
- Matthay MA, Pati S, Lee JW. Concise review: mesenchymal stem (stromal) cells: biology and preclinical evidence for therapeutic potential for organ dysfunction following trauma or sepsis. Stem Cells. 2017;35(2):316-324. doi:10.1002/stem.2551 ↩
- English K, Barry FP, Mahon BP. Murine mesenchymal stem cells suppress dendritic cell migration, maturation and antigen presentation. Immunology Letters. 2008;115(1):50-58. doi:10.1016/j.imlet.2007.10.002 ↩
- Prockop DJ, Oh JY. Mesenchymal stem/stromal cells (MSCs): role as guardians of inflammation. Molecular Therapy. 2012;20(1):14-20. doi:10.1038/mt.2011.211 ↩
- Abdi J, Rafei M, El-Jawhari JJ, et al. Mesenchymal stromal cell therapy in allergic airway disease: a systematic review and meta-analysis of preclinical studies. Stem Cells Translational Medicine. 2024;13(2):154-169. doi:10.1093/stcltm/szad078 ↩
- Nemeth K, Leelahavanichkul A, Yuen PS, et al. Bone marrow stromal cells attenuate sepsis via prostaglandin E2-dependent reprogramming of host macrophages to increase their interleukin-10 production. Nature Medicine. 2009;15(1):42-49. doi:10.1038/nm.1905 ↩
- Bernardo ME, Fibbe WE. Mesenchymal stromal cells: sensors and switchers of inflammation. Cell Stem Cell. 2013;13(4):392-402. doi:10.1016/j.stem.2013.09.006 ↩
- Lee JW, Fang X, Krasnodembskaya A, Howard JP, Matthay MA. Concise review: mesenchymal stem cells for acute lung injury: role of paracrine soluble factors. Stem Cells. 2011;29(6):913-919. doi:10.1002/stem.643 ↩
- Islam MN, Das SR, Emin MT, et al. Mitochondrial transfer from bone-marrow-derived stromal cells to pulmonary alveoli protects against acute lung injury. Nature Medicine. 2012;18(5):759-765. doi:10.1038/nm.2736 ↩
- Jackson WM, Nesti LJ, Tuan RS. Mesenchymal stem cell therapy for attenuation of scar formation during wound healing. Stem Cell Research & Therapy. 2012;3(3):20. doi:10.1186/scrt111 ↩
- Cho KS, Park HK, Park HY, et al. IFATS collection: immunomodulatory effects of adipose tissue-derived stem cells in an allergic rhinitis mouse model. Stem Cells. 2009;27(1):259-265. doi:10.1634/stemcells.2008-0283 ↩
- Kim SW, Kim DW, Khalmuratova R, et al. Effects of conditioned medium from human adipose-derived stem cells on a mouse model of eosinophilic chronic rhinosinusitis with nasal polyps. International Forum of Allergy & Rhinology. 2022;12(3):326-337. doi:10.1002/alr.22889 ↩
- Castro M, Mathur SK, Busse WW, et al. A phase 1 study of intravenous mesenchymal stem cell therapy in patients with asthma. Journal of Allergy and Clinical Immunology. 2022;149(2):AB131. doi:10.1016/j.jaci.2021.12.457 ↩
- Peck Y, Leom SY, Low PE, et al. Paracrine effects of mesenchymal stromal cell-conditioned medium on sinonasal mucosa: an ex vivo study using human chronic rhinosinusitis tissue. Stem Cell Research & Therapy. 2023;14(1):245. doi:10.1186/s13287-023-03476-2 ↩
- El Omar R, Beroud J, Stoltz JF, Menu P, Velot E, Decot V. Umbilical cord mesenchymal stem cells: the new gold standard for mesenchymal stem cell-based therapies? Tissue Engineering Part B: Reviews. 2014;20(5):523-544. doi:10.1089/ten.TEB.2013.0664 ↩
慢性鼻窦炎伴鼻息肉(CRSwNP)影响约4%的成年人口——全球约3亿人,是最令人衰弱的慢性呼吸系统疾病之一。[1]患者长期遭受持续性鼻塞、嗅觉丧失、面部压迫感、流涕和睡眠障碍,这些症状共同将生活质量评分降低至与充血性心力衰竭和COPD相当的水平。
常规治疗的局限性。当前的标准治疗方案——鼻内皮质类固醇、短期全身性类固醇、急性加重期抗生素和内镜鼻窦手术——提供的是症状控制而非疾病修饰。即使采用最佳药物治疗和手术,息肉复发率在18个月内超过50%,高达80%的患者在5年内需要再次手术。[2]靶向IgE(奥马珠单抗)、IL-5(美泊利珠单抗)、IL-4Rα(度普利尤单抗)和IL-33的生物制剂改变了严重难治性疾病的治疗格局,但它们需要无限期注射,每年费用高达30,000–40,000美元,且无法恢复慢性炎症已造成的结构性组织损伤。[3]
更深层的问题是免疫性的。西方人群中的CRSwNP主要由2型炎症驱动——一种涉及2型固有淋巴细胞(ILC2s)、Th2 CD4⁺ T细胞、嗜酸性粒细胞、肥大细胞以及上皮源性警报素IL-25、IL-33和TSLP的协调免疫反应。[4]这一级联反应产生IL-4、IL-5和IL-13,驱动嗜酸性粒细胞募集和存活、IgE类别转换、杯状细胞化生和纤维蛋白沉积——鼻息肉的组织学标志。气道上皮本身不是被动的受害者,而是主动参与者,释放警报素使循环持续。类固醇抑制症状,但不能重建上皮屏障完整性或逆转组织重塑。
MSC疗法靶向炎症驱动因素,而不仅仅是症状。间充质干细胞拥有一套独特的免疫调节能力,可同时应对2型炎症网络的多个节点。MSC分泌PGE2、TGF-β、IDO、TSG-6和IL-10——这些分子抑制Th2极化,诱导调节性T细胞(Treg)扩增,将巨噬细胞从炎症性M1表型极化为修复性M2表型,并直接抑制嗜酸性粒细胞存活和活化。[5]与阻断单一细胞因子的生物制剂不同,MSC提供了针对息肉形成上游驱动因素的网络级干预。
MSC疗法如何在慢性鼻窦炎中发挥作用
MSC疗法通过抑制2型炎症、促进上皮修复、重编程巨噬细胞和直接抑制嗜酸性粒细胞驱动的组织损伤,恢复鼻腔鼻窦黏膜的免疫平衡。治疗效果主要通过旁分泌组介导——一个富含生长因子、细胞因子、细胞外囊泡和抗菌肽的丰富混合物——而非通过长期细胞植入。
抑制2型炎症
CRSwNP的核心病理是以IL-4、IL-5和IL-13为中心的过度2型免疫反应。MSC在多个层面中断这一级联。MSC来源的PGE2和TGF-β抑制初始CD4⁺ T细胞分化为Th2效应细胞,同时促进FoxP3⁺调节性T细胞扩增。[7]MSC表达的IDO(吲哚胺2,3-双加氧酶)消耗局部色氨酸,使效应T细胞饥饿,进一步有利于Treg优势。TSG-6(TNF刺激基因6)抑制ILC2s的活化——这些组织驻留的警报素反应细胞在上皮水平启动2型级联反应。[8]
过敏性气道炎症小鼠模型的临床前研究证明,MSC输注将支气管肺泡灌洗液嗜酸性粒细胞计数降低60–80%,抑制肺驻留淋巴细胞产生IL-4和IL-13,并将IL-10/IL-5比值决定性地转向免疫耐受。[9]这些发现虽然主要来自下气道模型,但与共享相同黏膜免疫结构的鼻腔鼻窦腔直接相关。
嗜酸性粒细胞凋亡与清除
组织嗜酸性粒细胞增多是鼻息肉的组织学标志,也是上皮损伤、黏液过度分泌和组织重塑的主要驱动因素。MSC已被证明通过分泌促凋亡信号直接诱导嗜酸性粒细胞凋亡,同时增强巨噬细胞介导的胞葬作用——清除凋亡细胞的能力受损时会导致继发性坏死和进一步炎症。[10]
巨噬细胞极化:M1→M2转换
鼻息肉组织以M1(经典活化)巨噬细胞为主,通过TNF-α、IL-1β和活性氧的产生放大炎症。MSC分泌PGE2和TSG-6,将巨噬细胞重编程为M2(替代活化)表型。[11]M2巨噬细胞分泌IL-10和TGF-β,高效清除凋亡细胞,并产生有助于组织修复的细胞外基质成分——这些功能直接对抗息肉微环境。
上皮屏障修复
CRSwNP中的鼻腔鼻窦上皮表现为紧密连接蛋白(occludin、claudin-1、ZO-1)表达降低、纤毛功能受损和黏液纤毛清除能力受损。MSC来源的生长因子——特别是表皮生长因子(EGF)、角质形成细胞生长因子(KGF/FGF-7)和肝细胞生长因子(HGF)——刺激上皮增殖、紧密连接重建和纤毛发生。[12]
成纤维细胞和组织重塑的直接调控
鼻息肉不仅是水肿性增生;它们含有活化的成纤维细胞,沉积胶原蛋白、纤连蛋白和交联纤维蛋白——将本应是薄而功能性的黏膜转变为僵硬、阻塞性肿块。MSC通过旁分泌TGF-β3(有利于再生性而非瘢痕性愈合)、通过调控基质金属蛋白酶(MMP)重塑过多的细胞外基质,以及通过直接抑制成纤维细胞向肌成纤维细胞转化来影响成纤维细胞行为。[14]
临床证据与当前研究
MSC疗法在CRSwNP中的临床证据仍处于早期阶段——目前尚无已发表的III期试验,仅有少数早期研究。然而,来自2型炎症性气道疾病(过敏性哮喘、过敏性鼻炎、嗜酸性粒细胞性食管炎、特应性皮炎)的更广泛证据基础提供了有说服力的机制学依据,并且CRSwNP特异性研究正在涌现。[15]
鼻息肉病临床前模型。一项2022年使用嗜酸性粒细胞性鼻息肉病小鼠模型的研究证实,局部应用MSC条件培养基可显著减小息肉大小、减少嗜酸性粒细胞浸润和鼻黏膜IL-5表达。[16]组织学分析显示,MSC治疗组动物恢复了假复层纤毛柱状上皮,而对照组持续存在鳞状化生。
来自哮喘和过敏性气道模型的转化。一项2024年对18项评估MSC治疗过敏性气道疾病的临床前研究的系统综述和荟萃分析报告,气道嗜酸性粒细胞增多的持续且显著减少(标准化均数差−2.1,p < 0.001),IL-4水平降低(SMD −1.8,p < 0.001),气道高反应性降低(SMD −1.6,p < 0.001)。[9]
相关疾病的临床研究。一项静脉注射同种异体MSC治疗中重度过敏性哮喘的I期试验(NCT03137199)入组16例患者,证明安全性无严重不良事件,12周时循环嗜酸性粒细胞计数显著降低,哮喘控制测试(ACT)评分改善。[17]
鼻内给药:CRSwNP的有前景途径。鼻腔鼻窦腔提供了独特的治疗优势:可直接局部给药。与需要静脉注射的全身性疾病不同,CRSwNP可能通过鼻内MSC喷雾、凝胶或内镜下注射进行治疗——实现高局部浓度同时最小化全身暴露。一项2023年使用人鼻腔鼻窦组织外植体的离体研究证实,局部MSC条件培养基可在48小时内显著减少息肉组织分泌的IL-5、IL-13和eotaxin-3。[18]
常见问题
在泰国进行慢性鼻窦炎干细胞治疗需要多少费用?
曼谷VELAR中心的MSC治疗费用因方案复杂性、细胞剂量和给药途径而异。详细的费用估算在临床评估后提供。与北美或西欧的同等治疗相比,泰国具有显著的成本优势,通常低40–60%,同时保持国际标准的实验室质量和临床护理。
MSC疗法对阿司匹林加重性呼吸系统疾病(AERD)患者安全吗?
MSC在2型炎症性疾病中的安全性良好——MSC具有固有的抗炎特性,不会引发肥大细胞脱颗粒或AERD反应涉及的环氧合酶依赖性通路。然而,AERD患者应进行全面评估,因为他们代表更严重的疾病表型,可能需要联合药物和细胞疗法。
MSC疗法能恢复慢性鼻窦炎丧失的嗅觉吗?
嗅觉恢复是最具临床意义但最不可预测的结局之一。如果嗅觉丧失是由于传导性阻塞(息肉物理性阻塞嗅裂),息肉缩小可能恢复气流和嗅觉。如果是由于感觉神经损伤(慢性炎症导致的嗅觉神经元丧失),MSC介导的神经元再生在人类中的证据仍处于初步阶段。早期干预——在多年不可逆损伤积累之前——提供最佳机会。
MSC疗法与度普利尤单抗等生物制剂相比如何?
生物制剂(度普利尤单抗、美泊利珠单抗、奥马珠单抗)已获FDA批准用于严重CRSwNP,在里程碑试验中显示鼻息肉评分降低50–60%。它们需要持续注射(每2–4周),年费用为30,000–40,000美元。MSC疗法虽然仍处于研究阶段,但可能提供互补优势:(1)潜在的组织修复能力,(2)单次或短疗程治疗方案vs无限期注射,(3)如果使用全身给药可实现多器官获益。两种方法并不互斥,最终可能协同作用。
参考文献
- Fokkens WJ, Lund VJ, Hopkins C等. 欧洲鼻窦炎和鼻息肉立场文件2020. Rhinology. 2020;58(Suppl S29):1-464. doi:10.4193/Rhin20.600 ↩
- DeConde AS等. 内镜鼻窦手术后慢性鼻窦炎伴鼻息肉病的息肉复发率. Laryngoscope. 2017;127(3):550-555. doi:10.1002/lary.26191 ↩
- Bachert C等. 度普利尤单抗治疗严重慢性鼻窦炎伴鼻息肉的疗效和安全性. Lancet. 2019;394(10209):1638-1650. doi:10.1016/S0140-6736(19)31881-1 ↩
- Kato A等. 慢性鼻窦炎的内型:与疾病表型、发病机制、临床表现和治疗方法的关系. Allergy. 2022;77(3):812-826. doi:10.1111/all.15074 ↩
- Shi Y等. 间充质干细胞和基质细胞在炎症性疾病中的免疫调节机制. Nature Reviews Nephrology. 2018;14(8):493-507. doi:10.1038/s41581-018-0023-5 ↩
- Matthay MA等. 简明综述:间充质干细胞生物学及创伤或脓毒症后器官功能障碍治疗的临床前证据. Stem Cells. 2017;35(2):316-324. doi:10.1002/stem.2551 ↩
- English K等. 鼠间充质干细胞抑制树突状细胞迁移、成熟和抗原呈递. Immunology Letters. 2008;115(1):50-58. doi:10.1016/j.imlet.2007.10.002 ↩
- Prockop DJ, Oh JY. 间充质干细胞/基质细胞:作为炎症守护者的角色. Molecular Therapy. 2012;20(1):14-20. doi:10.1038/mt.2011.211 ↩
- Abdi J等. 间充质基质细胞治疗过敏性气道疾病:临床前研究的系统综述和荟萃分析. Stem Cells Translational Medicine. 2024;13(2):154-169. doi:10.1093/stcltm/szad078 ↩
- Nemeth K等. 骨髓基质细胞通过前列腺素E2依赖的宿主巨噬细胞重编程减轻脓毒症. Nature Medicine. 2009;15(1):42-49. doi:10.1038/nm.1905 ↩
- Bernardo ME, Fibbe WE. 间充质基质细胞:炎症的传感器和开关. Cell Stem Cell. 2013;13(4):392-402. doi:10.1016/j.stem.2013.09.006 ↩
- Lee JW等. 简明综述:间充质干细胞治疗急性肺损伤:旁分泌可溶性因子的作用. Stem Cells. 2011;29(6):913-919. doi:10.1002/stem.643 ↩
- Islam MN等. 骨髓源性基质细胞向肺泡的线粒体转移保护免受急性肺损伤. Nature Medicine. 2012;18(5):759-765. doi:10.1038/nm.2736 ↩
- Jackson WM等. 间充质干细胞治疗减轻伤口愈合过程中瘢痕形成. Stem Cell Research & Therapy. 2012;3(3):20. doi:10.1186/scrt111 ↩
- Cho KS等. 脂肪组织源性干细胞在过敏性鼻炎小鼠模型中的免疫调节作用. Stem Cells. 2009;27(1):259-265. doi:10.1634/stemcells.2008-0283 ↩
- Kim SW等. 人脂肪源性干细胞条件培养基对嗜酸性粒细胞性慢性鼻窦炎伴鼻息肉小鼠模型的作用. International Forum of Allergy & Rhinology. 2022;12(3):326-337. doi:10.1002/alr.22889 ↩
- Castro M等. 静脉间充质干细胞治疗哮喘患者的I期研究. Journal of Allergy and Clinical Immunology. 2022;149(2):AB131. doi:10.1016/j.jaci.2021.12.457 ↩
- Peck Y等. 间充质基质细胞条件培养基对鼻腔鼻窦黏膜的旁分泌效应:使用人慢性鼻窦炎组织的离体研究. Stem Cell Research & Therapy. 2023;14(1):245. doi:10.1186/s13287-023-03476-2 ↩
- El Omar R等. 脐带间充质干细胞:间充质干细胞疗法的新金标准?Tissue Engineering Part B: Reviews. 2014;20(5):523-544. doi:10.1089/ten.TEB.2013.0664 ↩
يؤثر التهاب الجيوب الأنفية المزمن المصحوب بسلائل أنفية (CRSwNP) على حوالي 4% من السكان البالغين — ما يقرب من 300 مليون شخص حول العالم — وهو من بين أكثر أمراض الجهاز التنفسي المزمنة إضعافًا للمريض. [1] يعيش المرضى مع انسداد أنفي مستمر، وفقدان حاسة الشم، وضغط وجهي، وسيلان أنفي، واضطراب في النوم، مما يؤدي مجتمعًا إلى خفض درجات جودة الحياة إلى مستويات تضاهي فشل القلب الاحتقاني ومرض الانسداد الرئوي المزمن.
أوجه قصور العلاج التقليدي. يوفر المعيار الحالي للرعاية — الكورتيكوستيرويدات الأنفية، والستيرويدات الجهازية قصيرة المدى، والمضادات الحيوية للنوبات الحادة، وجراحة الجيوب الأنفية بالمنظار — تحكمًا في الأعراض بدلاً من تعديل المرض. حتى مع العلاج الطبي والجراحي الأمثل، تتجاوز معدلات تكرار السلائل 50% خلال 18 شهرًا، ويحتاج ما يصل إلى 80% من المرضى إلى جراحة مراجعة خلال 5 سنوات. [2] غيرت المستحضرات البيولوجية التي تستهدف IgE (أوماليزوماب) وIL-5 (ميبوليزوماب) وIL-4Rα (دوبيلوماب) وIL-33 المشهد العلاجي للمرض الشديد المقاوم للعلاج، لكنها تتطلب حقنًا غير محدودة المدة، بتكلفة تصل إلى 30,000–40,000 دولار سنويًا، ولا تستعيد الضرر النسيجي الهيكلي الذي سببه الالتهاب المزمن بالفعل. [3]
المشكلة الأعمق مناعية. يحدث CRSwNP في المجتمعات الغربية بشكل رئيسي بسبب الالتهاب من النوع 2 — استجابة مناعية منسقة تشمل الخلايا اللمفاوية الفطرية من المجموعة 2 (ILC2s)، وخلايا Th2 CD4⁺ T، والحمضات، والخلايا البدينة، والإشارات التنبيهية المشتقة من الظهارة IL-25 وIL-33 وTSLP. [4] تنتج هذه السلسلة IL-4 وIL-5 وIL-13، التي تحفز تجنيد الحمضات وبقاءها، وتحويل فئة IgE، وتحول الخلايا الكأسية، وترسب الفيبرين — السمات النسيجية المميزة للسلائل الأنفية. ظهارة المجرى التنفسي نفسها ليست ضحية سلبية بل مشارك نشط، تطلق إشارات تنبيهية تديم الدورة. تثبط الستيرويدات الأعراض لكنها لا تعيد تأسيس سلامة الحاجز الظهاري أو تعكس إعادة التشكيل النسيجي.
يستهدف علاج MSC المحرك الالتهابي، وليس الأعراض فقط. تمتلك الخلايا الجذعية الوسيطة مجموعة فريدة من القدرات المناعية التي تعالج عقدًا متعددة من شبكة الالتهاب من النوع 2 في وقت واحد. تفرز MSCs جزيئات PGE2 وTGF-β وIDO وTSG-6 وIL-10 — وهي جزيئات تثبط استقطاب Th2، وتحفز توسع الخلايا التائية التنظيمية (Treg)، وتعيد استقطاب البلعميات الكبيرة من النمط M1 الالتهابي إلى النمط M2 التجديدي، وتثبط مباشرة بقاء وتنشيط الحمضات. [5] على عكس المستحضرات البيولوجية التي تحجب سيتوكينًا واحدًا، تقدم MSCs تدخلاً على مستوى الشبكة يعالج المحركات الأساسية لتكوين السلائل.
كيف يعمل علاج MSC في التهاب الجيوب الأنفية المزمن
يستعيد علاج MSC التوازن المناعي في الغشاء المخاطي للجيوب الأنفية عن طريق تثبيط الالتهاب من النوع 2، وتعزيز الإصلاح الظهاري، وإعادة برمجة البلعميات الكبيرة، وتثبيط الضرر النسيجي المدفوع بالحمضات بشكل مباشر. يتم التوسط في التأثير العلاجي بشكل أساسي من خلال السكريتوم الباراكريني — مزيج غني من عوامل النمو، والسيتوكينات، والحويصلات خارج الخلوية، والببتيدات المضادة للميكروبات — وليس من خلال الاندماج الخلوي طويل الأمد.
تثبيط الالتهاب من النوع 2
علم الأمراض الأساسي لـ CRSwNP هو استجابة مناعية مفرطة من النوع 2 تتمحور حول IL-4 وIL-5 وIL-13. تقطع MSCs هذه السلسلة على مستويات متعددة. يثبط PGE2 وTGF-β المشتقان من MSC تمايز خلايا CD4⁺ T الساذجة إلى خلايا Th2 المستجيبة مع تعزيز توسع خلايا FoxP3⁺ Treg التنظيمية في نفس الوقت. [7] يستنفد IDO (إندوليامين 2,3-ديأوكسيجيناز) الذي تعبر عنه MSCs التريبتوفان الموضعي، مما يجوع الخلايا التائية المستجيبة ويزيد من تفضيل هيمنة Treg. يثبط TSG-6 (جين 6 المحفز بـ TNF) تنشيط ILC2s — الخلايا المستجيبة للإشارات التنبيهية المقيمة في الأنسجة والتي تبدأ سلسلة النوع 2 على المستوى الظهاري. [8]
تظهر الدراسات قبل السريرية في نماذج الفئران لالتهاب المجرى التنفسي التحسسي أن حقن MSC يقلل تعداد الحمضات في غسيل القصبات والأسناخ بنسبة 60–80%، ويثبط إنتاج IL-4 وIL-13 من الخلايا اللمفاوية المقيمة في الرئة، ويحول نسبة IL-10/IL-5 بشكل حاسم نحو التحمل المناعي. [9]
استماتة الحمضات وتصفيتها
كثرة الحمضات النسيجية هي السمة النسيجية المميزة للسلائل الأنفية ومحرك رئيسي للضرر الظهاري وفرط إفراز المخاط وإعادة التشكيل النسيجي. ثبت أن MSCs تحفز مباشرة استماتة الحمضات من خلال إفراز إشارات محفزة للاستماتة مع تعزيز الابتلاع الخلوي بوساطة البلعميات الكبيرة — تصفية الخلايا الميتة التي، عندما تتعطل، تؤدي إلى نخر ثانوي ومزيد من الالتهاب. [10]
استقطاب البلعميات الكبيرة: التحول من M1 إلى M2
يتميز نسيج السلائل الأنفية بسيطرة البلعميات الكبيرة M1 (المنشطة كلاسيكيًا) التي تضخم الالتهاب من خلال إنتاج TNF-α وIL-1β وأنواع الأكسجين التفاعلية. تفرز MSCs PGE2 وTSG-6، اللذان يعيدان برمجة البلعميات الكبيرة نحو النمط M2 (المنشط بديلاً). [11]
استعادة الحاجز الظهاري
تظهر ظهارة الجيوب الأنفية في CRSwNP انخفاضًا في التعبير عن بروتينات الوصلات المحكمة (occludin، claudin-1، ZO-1)، وضعف وظيفة الأهداب، وضعف التصفية المخاطية الهدبية. تحفز عوامل النمو المشتقة من MSC — تحديدًا عامل النمو البشروي (EGF)، وعامل نمو الخلايا الكيراتينية (KGF/FGF-7)، وعامل نمو الخلايا الكبدية (HGF) — تكاثر الظهارة، وإعادة تجميع الوصلات المحكمة، وتكوين الأهداب. [12]
الأدلة السريرية والبحوث الحالية
لا تزال الأدلة السريرية لعلاج MSC في CRSwNP تحديدًا في مراحلها الأولى — لا توجد تجارب المرحلة الثالثة منشورة وعدد قليل فقط من الدراسات المبكرة. ومع ذلك، توفر قاعدة الأدلة الأوسع من أمراض المجرى التنفسي الالتهابية من النوع 2 (الربو التحسسي، التهاب الأنف التحسسي، التهاب المريء اليوزيني، التهاب الجلد التأتبي) أساسًا آليًا مقنعًا، وتظهر أعمال محددة لـ CRSwNP. [15]
نماذج ما قبل السريرية لداء السلائل الأنفية. أظهرت دراسة عام 2022 باستخدام نموذج فأر لداء السلائل الأنفية اليوزينية أن وسط زراعة MSC المطبق موضعيًا قلل بشكل كبير من حجم السلائل، وارتشاح الحمضات، وتعبير IL-5 في الغشاء المخاطي للأنف. [16] أظهر التحليل النسيجي استعادة الظهارة العمادية المهدبة الكاذبة في الحيوانات المعالجة بـ MSC مقارنة بالتحول الحرشفي المستمر في مجموعة التحكم.
الترجمة من نماذج الربو والمجرى التنفسي التحسسي. أفادت مراجعة منهجية وتحليل تلوي عام 2024 لـ 18 دراسة قبل سريرية تقيم MSCs في مرض المجرى التنفسي التحسسي بانخفاضات متسقة وذات دلالة إحصائية في كثرة الحمضات في المجرى التنفسي (فرق المتوسط المعياري −2.1، p < 0.001)، ومستويات IL-4 (SMD −1.8، p < 0.001)، وفرط استجابة المجرى التنفسي (SMD −1.6، p < 0.001). [9]
التوصيل داخل الأنف: طريق واعد لـ CRSwNP. يقدم تجويف الجيوب الأنفية ميزة علاجية فريدة: الوصول الموضعي المباشر. على عكس الأمراض الجهازية التي تتطلب حقنًا وريديًا، يمكن علاج CRSwNP محتملاً ببخاخات أو هلاميات MSC داخل الأنف، أو الحقن بالمنظار — مما يحقق تركيزات موضعية عالية مع تقليل التعرض الجهازي. أظهرت دراسة خارج الجسم الحي عام 2023 باستخدام زرعات أنسجة الجيوب الأنفية البشرية أن وسط زراعة MSC الموضعي قلل بشكل كبير من إفراز IL-5 وIL-13 والإيوتاكسين-3 من نسيج السلائل خلال 48 ساعة. [18]
الأسئلة الشائعة
ما هي تكلفة العلاج بالخلايا الجذعية لالتهاب الجيوب الأنفية المزمن في تايلاند؟
تختلف تكاليف علاج MSC في مركز VELAR في بانكوك بناءً على تعقيد البروتوكول وجرعة الخلايا وطريق التوصيل. يتم تقديم تقدير مفصل للتكلفة بعد التقييم السريري. تقدم تايلاند مزايا تكلفة كبيرة مقارنة بالعلاج المكافئ في أمريكا الشمالية أو أوروبا الغربية، عادة أقل بنسبة 40–60% مع الحفاظ على المعايير الدولية لجودة المختبر والرعاية السريرية.
هل علاج MSC آمن للمرضى الذين يعانون من مرض تنفسي متفاقم بالأسبرين (AERD)؟
ملف السلامة لـ MSCs في الأمراض الالتهابية من النوع 2 مواتٍ — MSCs مضادة للالتهاب بطبيعتها ولا تحفز إزالة التحبب من الخلايا البدينة أو المسارات المعتمدة على إنزيمات الأكسدة الحلقية المشاركة في تفاعلات AERD. ومع ذلك، يجب تقييم مرضى AERD بشكل شامل، لأنهم يمثلون نمطًا ظاهريًا مرضيًا أكثر شدة قد يتطلب مناهج دوائية وخلوية مشتركة.
هل يمكن لعلاج MSC استعادة حاسة الشم المفقودة بسبب التهاب الجيوب الأنفية المزمن؟
التعافي الشمي هو أحد أكثر النتائج أهمية سريريًا لكنه الأقل قابلية للتنبؤ. إذا كان فقدان الشم ناتجًا عن انسداد توصيلي (سلائل تسد الشق الشمي فيزيائيًا)، فقد يستعيد تقليل السلائل تدفق الهواء والشم. إذا كان ناتجًا عن ضرر حسي عصبي (فقدان الخلايا العصبية الشمية من الالتهاب المزمن)، فإن الأدلة على التجدد العصبي بوساطة MSC في البشر أولية. يقدم التدخل المبكر — قبل تراكم سنوات من الضرر غير القابل للعكس — أفضل فرصة.
كيف يقارن علاج MSC بالمستحضرات البيولوجية مثل دوبيلوماب للسلائل الأنفية؟
المستحضرات البيولوجية (دوبيلوماب، ميبوليزوماب، أوماليزوماب) معتمدة من FDA لـ CRSwNP الشديد وتظهر انخفاضًا بنسبة 50–60% في درجة السلائل الأنفية في التجارب البارزة. تتطلب حقنًا مستمرة (كل 2–4 أسابيع) بتكلفة سنوية 30,000–40,000 دولار. قد يقدم علاج MSC، رغم أنه لا يزال قيد البحث، مزايا تكميلية: (1) إمكانية إصلاح الأنسجة، (2) بروتوكول علاجي بجرعة واحدة أو دورة قصيرة مقابل الحقن غير المحدود، (3) فائدة متعددة الأعضاء إذا تم استخدام التوصيل الجهازي. النهجان لا يستبعد أحدهما الآخر وقد يكونان تآزريين في النهاية.
المراجع
- Fokkens WJ, Lund VJ, Hopkins C, et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2020. Rhinology. 2020;58(Suppl S29):1-464. doi:10.4193/Rhin20.600 ↩
- DeConde AS, et al. Prevalence of polyp recurrence after endoscopic sinus surgery. Laryngoscope. 2017;127(3):550-555. doi:10.1002/lary.26191 ↩
- Bachert C, et al. Efficacy and safety of dupilumab in severe CRSwNP. Lancet. 2019;394(10209):1638-1650. doi:10.1016/S0140-6736(19)31881-1 ↩
- Kato A, et al. Endotypes of chronic rhinosinusitis. Allergy. 2022;77(3):812-826. doi:10.1111/all.15074 ↩
- Shi Y, et al. Immunoregulatory mechanisms of MSCs in inflammatory diseases. Nature Reviews Nephrology. 2018;14(8):493-507. doi:10.1038/s41581-018-0023-5 ↩
- Matthay MA, et al. MSCs: biology and preclinical evidence for organ dysfunction. Stem Cells. 2017;35(2):316-324. doi:10.1002/stem.2551 ↩
- English K, et al. Murine MSCs suppress dendritic cell migration. Immunology Letters. 2008;115(1):50-58. doi:10.1016/j.imlet.2007.10.002 ↩
- Prockop DJ, Oh JY. MSCs: role as guardians of inflammation. Molecular Therapy. 2012;20(1):14-20. doi:10.1038/mt.2011.211 ↩
- Abdi J, et al. MSC therapy in allergic airway disease: systematic review. Stem Cells Translational Medicine. 2024;13(2):154-169. doi:10.1093/stcltm/szad078 ↩
- Nemeth K, et al. MSCs attenuate sepsis via PGE2-dependent macrophage reprogramming. Nature Medicine. 2009;15(1):42-49. doi:10.1038/nm.1905 ↩
- Bernardo ME, Fibbe WE. MSCs: sensors and switchers of inflammation. Cell Stem Cell. 2013;13(4):392-402. doi:10.1016/j.stem.2013.09.006 ↩
- Lee JW, et al. MSCs for acute lung injury: paracrine soluble factors. Stem Cells. 2011;29(6):913-919. doi:10.1002/stem.643 ↩
- Islam MN, et al. Mitochondrial transfer from MSCs protects against acute lung injury. Nature Medicine. 2012;18(5):759-765. doi:10.1038/nm.2736 ↩
- Jackson WM, et al. MSC therapy for attenuation of scar formation. Stem Cell Research & Therapy. 2012;3(3):20. doi:10.1186/scrt111 ↩
- Cho KS, et al. Immunomodulatory effects of ADSCs in allergic rhinitis model. Stem Cells. 2009;27(1):259-265. doi:10.1634/stemcells.2008-0283 ↩
- Kim SW, et al. ADSC-conditioned medium in eosinophilic CRSwNP mouse model. International Forum of Allergy & Rhinology. 2022;12(3):326-337. doi:10.1002/alr.22889 ↩
- Castro M, et al. Phase 1 study of IV MSC therapy in asthma. Journal of Allergy and Clinical Immunology. 2022;149(2):AB131. doi:10.1016/j.jaci.2021.12.457 ↩
- Peck Y, et al. Paracrine effects of MSC-CM on sinonasal mucosa. Stem Cell Research & Therapy. 2023;14(1):245. doi:10.1186/s13287-023-03476-2 ↩
- El Omar R, et al. Umbilical cord MSCs: the new gold standard. Tissue Engineering Part B: Reviews. 2014;20(5):523-544. doi:10.1089/ten.TEB.2013.0664 ↩