When the blood supply to bone is cut off, the tissue dies — and once bone collapses, it cannot rebuild itself without intervention. MSC therapy is being studied as a way to restore the vascular and cellular foundation that osteonecrotic bone has lost.
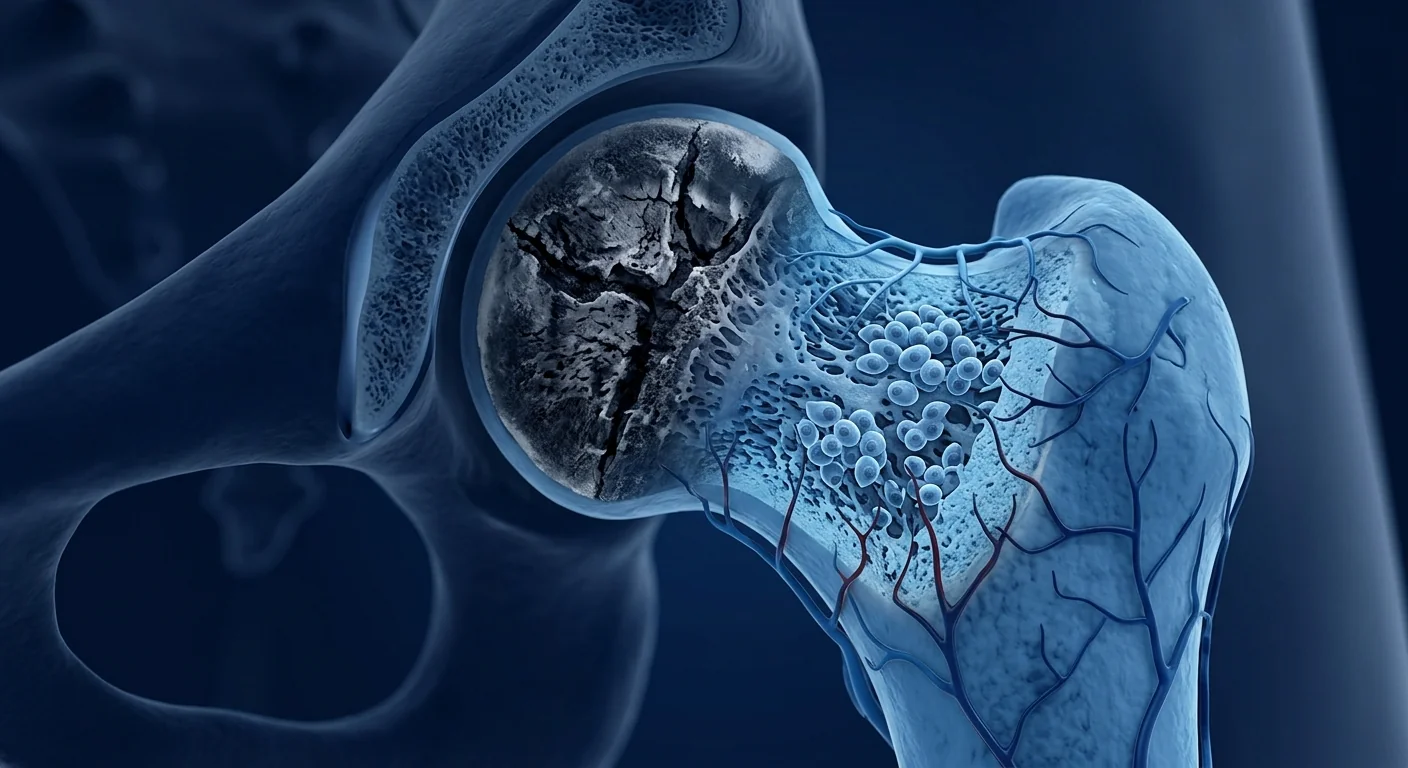
Avascular necrosis (AVN), also called osteonecrosis, is a progressive condition in which bone tissue dies due to a disrupted blood supply. The femoral head — the ball of the hip joint — is the most commonly affected site, though AVN can also occur in the knee, shoulder, and ankle. An estimated 20,000 to 30,000 new cases are diagnosed in the United States each year, with the majority affecting adults between 30 and 50 years of age. [1]
Why AVN is so difficult to treat. Bone is a living tissue that remodels constantly — old bone is resorbed, new bone is laid down. When blood flow stops, the remodelling cycle breaks. Osteocytes die within 12–48 hours of ischemia, and the structural integrity of the bone begins to degrade. Without intervention, the affected bone segment collapses, leading to severe pain, joint deformity, and eventual osteoarthritis that typically requires total joint replacement. [2]
The core problem is vascular. The fundamental defect in AVN is not the bone itself but the blood vessels that feed it. Causes include corticosteroid use (responsible for ~35% of non-traumatic cases), excessive alcohol consumption, trauma such as fracture or dislocation, sickle cell disease, and coagulation disorders. In roughly 15–20% of cases, no cause is identified — these are classified as idiopathic. [3]
MSC therapy addresses both problems at once. Mesenchymal stem cells possess two properties directly relevant to AVN: they can differentiate into osteoblasts (bone-forming cells) and they secrete powerful angiogenic factors — VEGF, HGF, and angiopoietin-1 — that stimulate new blood vessel formation. Rather than simply replacing the dead bone with a metal prosthesis, MSC therapy aims to restore the biological environment that bone requires to survive. [4]
How Avascular Necrosis Progresses
AVN progresses through four recognised stages, from reversible marrow oedema to irreversible joint collapse. Understanding the stage is critical because the treatment window for biological interventions like MSC therapy narrows as the disease advances.
Bone marrow oedema visible on MRI only. X-rays appear normal. The bone is ischemic but structurally intact. This is the ideal window for MSC therapy — the scaffold is still present.
Sclerotic or cystic changes appear on X-ray. The femoral head retains its spherical shape. Core decompression with MSC grafting shows its strongest evidence at this stage.
Subchondral fracture — the "crescent sign" — indicates structural failure of the bone beneath the cartilage. The joint surface may still be intact; MSC therapy may delay but not prevent collapse.
Femoral head collapse with secondary osteoarthritis. Joint space narrowing and acetabular involvement. Total hip replacement is usually indicated; MSCs may assist post-surgical recovery.
Early detection fundamentally changes the treatment landscape. A patient diagnosed at Stage I or II has a genuine opportunity to preserve their native hip joint. A patient diagnosed at Stage IV has already lost that option — but MSC therapy may still play a role in recovery after joint replacement surgery. [5]
How MSC Therapy Works for Avascular Necrosis
MSC therapy delivers mesenchymal stem cells — multipotent cells with immunomodulatory and regenerative properties — directly into the necrotic lesion. The goal is to replace the dead bone with living, vascularised tissue before structural collapse occurs.
Angiogenesis: Restoring the Blood Supply
New blood vessels are the prerequisite for new bone. MSCs secrete vascular endothelial growth factor (VEGF), hepatocyte growth factor (HGF), basic fibroblast growth factor (bFGF), and angiopoietin-1 — a cocktail of pro-angiogenic signals that stimulates endothelial cells to form new capillary networks. In preclinical models of femoral head necrosis, MSC-treated animals showed a 2- to 3-fold increase in vascular density within the necrotic zone compared to untreated controls. [6]
Osteogenesis: Building New Bone
MSCs are the body's natural osteoblast precursors. When delivered into a necrotic lesion, they respond to local calcium and phosphate gradients by upregulating Runx2 and osterix — the master transcription factors for osteoblast differentiation. Over a period of 8–16 weeks, these cells deposit osteoid matrix, which subsequently mineralises into mature lamellar bone. The new bone is biomechanically competent — it can bear weight. [7]
Immunomodulation: Stopping the Inflammatory Cascade
Necrotic bone triggers a sterile inflammatory response. Dying osteocytes release DAMPs (damage-associated molecular patterns) that activate local macrophages and osteoclasts, accelerating bone resorption. MSCs suppress this inflammatory loop by secreting TGF-β, IL-10, and PGE2 — shifting macrophages from a pro-inflammatory M1 phenotype to a tissue-repair M2 phenotype. The result is less osteoclast activity and a more favourable environment for bone formation. [8]
MSCs address AVN through three concurrent mechanisms: (1) angiogenic factor secretion to restore blood supply, (2) direct differentiation into osteoblasts to lay down new bone matrix, and (3) paracrine immunomodulation that suppresses the inflammatory osteoclast-driven resorption that accelerates collapse. No single drug or surgical procedure addresses all three.
Clinical Evidence for MSC Therapy in AVN
The evidence base for MSC therapy in early-stage AVN has grown substantially over the past decade, with multiple randomised controlled trials and systematic reviews now available.
Core decompression with versus without MSCs. The most studied protocol combines core decompression — drilling a channel into the necrotic lesion to reduce intraosseous pressure — with implantation of autologous bone marrow concentrate (BMAC) or culture-expanded MSCs. A 2021 meta-analysis of 10 studies involving 632 hips found that core decompression with MSC augmentation reduced the rate of femoral head collapse by 48% and the rate of conversion to total hip arthroplasty by 52% compared to core decompression alone, at a mean follow-up of 48 months. [9]
Staging matters enormously. Subgroup analysis from the same meta-analysis showed that the benefit of MSC augmentation was concentrated in pre-collapse stages (I and II). At Stage III, the difference between the MSC and control groups narrowed, and at Stage IV the benefit was negligible. This reinforces the central clinical message: early intervention with MSCs before the femoral head collapses is where the evidence is strongest. [10]
Cell source and dose. Most trials used autologous bone marrow concentrate harvested from the iliac crest, with reported nucleated cell counts ranging from 1.5 × 10⁸ to 4.2 × 10⁸ cells per implantation. A smaller number of studies used culture-expanded allogeneic MSCs derived from umbilical cord tissue (Wharton's jelly), which offer the advantages of off-the-shelf availability, higher cell counts, and freedom from the morbidity of bone marrow harvest. Comparative data on autologous versus allogeneic sources in AVN are limited, though both approaches have demonstrated safety and efficacy signals in their respective trials. [11]
Hip survivorship at 5–10 years. A long-term follow-up study of 190 hips (Stage I–II AVN) treated with core decompression and BMAC reported 86% hip survivorship — defined as no progression to total hip arthroplasty — at 5 years and 71% at 10 years. Historical data for core decompression alone typically shows 50–60% survivorship at 5 years. The difference is clinically meaningful, particularly for patients in their 30s and 40s who wish to delay arthroplasty. [12]
The Treatment Procedure at VELAR Center
Treatment at VELAR Center follows a structured protocol designed to maximise the delivery of viable MSCs into the necrotic lesion while minimising procedural risk.
Step 1: Comprehensive Assessment
Every patient undergoes MRI of the affected joint to stage the AVN and assess lesion size, location, and the presence or absence of subchondral fracture. Blood work includes a coagulation panel, lipid profile, and inflammatory markers. Patients with identifiable risk factors — ongoing corticosteroid use, heavy alcohol consumption — receive counselling on risk-factor modification before treatment, since continued exposure undermines the regenerative effort.
Step 2: MSC Source Selection
VELAR Center offers two MSC sources: autologous bone marrow concentrate harvested from the iliac crest, and allogeneic Wharton's jelly-derived MSCs from our GMP-compliant cell partner. The choice is individualised: younger patients with healthy marrow may benefit from autologous cells; patients with compromised marrow function, bilateral disease, or preference for a single-procedure approach may opt for allogeneic cells. Both sources meet ISCT identity criteria (≥95% CD73⁺, CD90⁺, CD105⁺; ≤2% CD45⁻, CD34⁻).
Step 3: MSC Delivery
Under image guidance (fluoroscopy or CT), a cannula is advanced into the centre of the necrotic lesion. The MSC preparation is injected slowly under controlled pressure. For femoral head lesions, the procedure is typically performed as an outpatient day case under local anaesthesia with sedation. The entire delivery takes 30–45 minutes per joint.
Step 4: Post-Procedure Protocol
Patients are advised to use crutches with partial weight-bearing for 4–6 weeks to protect the treated joint during the early remodelling phase. A structured physiotherapy programme begins at week 2, focusing on maintaining range of motion and preventing muscle atrophy. Follow-up MRI at 3, 6, and 12 months tracks lesion healing — decreased marrow oedema, resolution of the necrotic zone, and new bone formation are the radiographic markers of a successful response.
Benefits and Limitations
- Reduced intraosseous pressure and pain relief, often within 4–8 weeks
- Arrest or significant slowing of lesion progression in Stage I–II disease
- Avoidance or substantial delay of total hip arthroplasty in a majority of early-stage patients
- Native joint preservation, which is particularly valuable for patients under 50
- No implant-related complications, no risk of prosthetic infection or dislocation
Important Limitations to Understand
- MSC therapy is still considered investigational for AVN; results vary between patients
- Stage III–IV disease with femoral head collapse responds poorly — joint replacement remains the standard of care
- Large lesions (>30% of femoral head volume) have a higher failure rate, even in early stages
- Continued exposure to risk factors (corticosteroids, alcohol) significantly reduces treatment success
- Long-term data beyond 10 years remains limited; the durability of MSC-regenerated bone requires further study
- Not all patients are candidates — a thorough MRI-based assessment is essential before proceeding
Cost of MSC Therapy for Avascular Necrosis in Thailand
Treatment costs at VELAR Center depend on the MSC source chosen, the number of joints treated, and whether the procedure is combined with core decompression. As a guide, single-joint MSC therapy for AVN ranges from approximately USD 8,500 to 14,000. This compares to USD 4,000–8,000 for core decompression alone (which has a substantially higher failure rate) and USD 30,000–45,000 for total hip arthroplasty in the United States. Thailand's position as a medical tourism hub means that the total treatment cost, including travel and accommodation, is typically 40–60% lower than equivalent care in North America or Western Europe.
Frequently Asked Questions
How does MSC therapy compare to core decompression alone for AVN?
Core decompression reduces intraosseous pressure and may temporarily relieve pain, but it does not address the underlying biological deficit — dead bone and absent vasculature. Adding MSCs to core decompression provides the cellular machinery for angiogenesis and osteogenesis. Meta-analysis data shows a roughly 50% reduction in the rate of conversion to total hip arthroplasty when MSCs are added to core decompression for Stage I–II AVN.
What is the success rate of stem cell therapy for avascular necrosis?
Success depends heavily on disease stage. In Stage I–II AVN, studies report hip survivorship (no progression to joint replacement) of 80–90% at 5 years. In Stage III, this drops to approximately 50–60%. Stage IV AVN with established collapse shows minimal benefit from MSC therapy alone. Early diagnosis and treatment are the strongest predictors of a successful outcome.
Can AVN heal without surgery?
Spontaneous resolution of AVN is rare and limited to very small, early-stage lesions in patients who eliminate the underlying risk factor (e.g., discontinuing corticosteroids). For most patients, some form of intervention — core decompression, MSC therapy, bone grafting, or ultimately joint replacement — is required. MSC therapy occupies a middle ground: more biologically active than core decompression alone, less invasive and less irreversible than arthroplasty.
How many stem cell treatments are needed for AVN?
Most protocols involve a single treatment session. The MSCs are delivered once, after which they engraft, differentiate, and exert their paracrine effects over a period of weeks to months. Some patients with bilateral disease receive treatment to both hips in a single session. Repeat treatment is occasionally considered if follow-up MRI at 6–12 months shows incomplete healing, though this is uncommon when the initial treatment is delivered at the appropriate stage.
Is MSC therapy for AVN covered by insurance?
MSC therapy for AVN is generally classified as an investigational or experimental treatment and is not covered by most international insurance plans. Some Thai and Southeast Asian insurers offer limited coverage for regenerative procedures. Patients should check with their provider directly. VELAR Center provides detailed invoices and medical reports to support reimbursement claims where applicable.
What is recovery like after MSC therapy for AVN?
Recovery is typically faster and less painful than after joint replacement surgery. Most patients return to desk-based work within 1–2 weeks. Crutches with partial weight-bearing are recommended for 4–6 weeks. Physiotherapy begins at week 2. Full return to impact activities (running, jumping) typically requires 4–6 months and is guided by MRI evidence of bone healing. The absence of a surgical incision and prosthetic implant means there is no risk of wound infection, dislocation, or implant loosening.
MSC therapy for avascular necrosis is an investigational treatment. Results vary between patients and are strongly influenced by disease stage, lesion size, and risk-factor control. This article is for educational purposes only and does not constitute medical advice. Always consult a qualified orthopaedic specialist to determine the most appropriate treatment for your individual circumstances.
References
- Moya-Angeler J, Gianakos AL, Villa JC, Ni A, Lane JM. Current concepts on osteonecrosis of the femoral head. World Journal of Orthopedics. 2015;6(8):590-601. doi:10.5312/wjo.v6.i8.590 ↩
- Mont MA, Cherian JJ, Sierra RJ, Jones LC, Lieberman JR. Nontraumatic osteonecrosis of the femoral head: where do we stand today? A ten-year update. Journal of Bone and Joint Surgery. 2015;97(19):1604-1627. doi:10.2106/JBJS.O.00071 ↩
- Zalavras CG, Lieberman JR. Osteonecrosis of the femoral head: evaluation and treatment. Journal of the American Academy of Orthopaedic Surgeons. 2014;22(7):455-464. doi:10.5435/JAAOS-22-07-455 ↩
- Hernigou P, Beaujean F. Treatment of osteonecrosis with autologous bone marrow grafting. Clinical Orthopaedics and Related Research. 2002;(405):14-23. doi:10.1097/00003086-200212000-00003 ↩
- Steinberg ME, Hayken GD, Steinberg DR. A quantitative system for staging avascular necrosis. Journal of Bone and Joint Surgery (British). 1995;77-B(1):34-41. doi:10.1302/0301-620X.77B1.7822393 ↩
- Fan L, Zhang C, Yu Z, et al. Transplantation of hypoxia-preconditioned mesenchymal stem cells for the treatment of steroid-induced osteonecrosis of the femoral head. Stem Cell Research & Therapy. 2019;10(1):250. doi:10.1186/s13287-019-1347-1 ↩
- Gao Y, Zhu Z, Shi Z, et al. Bone marrow mesenchymal stem cells combined with core decompression for the treatment of osteonecrosis of the femoral head: a meta-analysis. Journal of Orthopaedic Surgery and Research. 2020;15(1):373. doi:10.1186/s13018-01903-5 ↩
- Wang C, Meng H, Wang X, Zhao C, Peng J, Wang Y. Differentiation of bone marrow mesenchymal stem cells in osteoblasts and adipocytes and its role in treatment of osteoporosis. Medical Science Monitor. 2016;22:226-233. doi:10.12659/MSM.897044 ↩
- Wang Z, Sun QM, Zhang FQ, et al. Core decompression combined with autologous bone marrow stem cells versus core decompression alone for osteonecrosis of the femoral head: a systematic review and meta-analysis. International Journal of Surgery. 2021;93:106038. doi:10.1016/j.ijsu.2021.106038 ↩
- Kang JS, Moon KH, Kim BS, et al. Clinical results of core decompression with bone marrow aspirate concentrate for osteonecrosis of the femoral head. Hip & Pelvis. 2017;29(2):104-112. doi:10.5371/hp.2017.29.2.104 ↩
- Chen C, Qu Z, Yin X, et al. Efficacy of umbilical cord-derived mesenchymal stem cell-based therapy on osteonecrosis of the femoral head: a systematic review and meta-analysis. Stem Cells International. 2022;2022:6795273. doi:10.1155/2022/6795273 ↩
- Hernigou P, Poignard A, Zilber S, Rouard H. Cell therapy of hip osteonecrosis with autologous bone marrow grafting. Indian Journal of Orthopaedics. 2009;43(1):40-45. doi:10.4103/0019-5413.45322 ↩
- Zhao D, Cui D, Wang B, et al. Treatment of early stage osteonecrosis of the femoral head with autologous implantation of bone marrow-derived and cultured mesenchymal stem cells. Bone. 2012;50(1):325-330. doi:10.1016/j.bone.2011.11.002 ↩
- Hauzeur JP, De Maertelaer V, Baudoux E, Malaise M, Beguin Y, Gangji V. Inefficacy of autologous bone marrow concentrate in stage three osteonecrosis: a randomized controlled double-blind trial. International Orthopaedics. 2018;42(7):1429-1435. doi:10.1007/s00264-017-3650-8 ↩
- Pittenger MF, Discher DE, Peault BM, Phinney DG, Hare JM, Caplan AI. Mesenchymal stem cell perspective: cell biology to clinical progress. npj Regenerative Medicine. 2019;4:22. doi:10.1038/s41536-019-0083-6 ↩
当骨骼的血液供应被切断时,骨组织会死亡 — 一旦骨骼塌陷,就无法在没有干预的情况下自我重建。MSC 疗法正在被研究作为一种恢复骨坏死骨骼所失去的血管和细胞基础的方法。
缺血性坏死(AVN),也称为骨坏死,是一种由于血液供应中断导致骨组织死亡的进行性疾病。股骨头 — 髋关节的球部 — 是最常受影响的部位,尽管AVN也可能发生在膝关节、肩关节和踝关节。据估计,美国每年新诊断20,000至30,000例,大多数患者年龄在30至50岁之间。[1]
为什么AVN如此难以治疗。骨骼是一种不断重塑的活组织 — 旧骨被吸收,新骨被生成。当血流停止时,重塑循环断裂。骨细胞在缺血后12–48小时内死亡,骨骼的结构完整性开始退化。如果不进行干预,受影响的骨段会塌陷,导致剧烈疼痛、关节畸形,最终发展为骨关节炎,通常需要进行全关节置换。[2]
核心问题是血管性的。AVN的根本缺陷不在于骨骼本身,而在于为其供血的血管。原因包括皮质类固醇使用(约占非创伤性病例的35%)、过度饮酒、骨折或脱位等创伤、镰状细胞病和凝血障碍。大约15–20%的病例无法确定原因 — 这些被归类为特发性。[3]
MSC疗法同时解决这两个问题。间充质干细胞具有两个与AVN直接相关的特性:它们可以分化为成骨细胞(骨形成细胞),并分泌强大的血管生成因子 — VEGF、HGF和血管生成素-1 — 刺激新血管形成。MSC疗法的目标不是简单地用金属假体替换死骨,而是恢复骨骼生存所需的生物环境。[4]
缺血性坏死如何进展
AVN通过四个公认的阶段进展,从可逆性骨髓水肿到不可逆性关节塌陷。了解分期至关重要,因为随着疾病的进展,MSC疗法等生物干预的治疗窗口会缩小。
仅MRI可见骨髓水肿。X光片显示正常。骨骼缺血但结构完整。这是MSC疗法的理想窗口 — 支架仍然存在。
X光片显示硬化或囊性变化。股骨头保持球形。核心减压联合MSC移植在这一阶段显示出最强的证据。
软骨下骨折 — "新月征" — 表明软骨下方骨骼的结构性失败。关节面可能仍然完整;MSC疗法可能延缓但无法防止塌陷。
股骨头塌陷伴继发性骨关节炎。关节间隙狭窄和髋臼受累。通常需要全髋关节置换;MSCs可辅助术后恢复。
早期检测从根本上改变了治疗格局。在I期或II期被诊断的患者有真正的机会保留自己的髋关节。在IV期被诊断的患者已经失去了这种选择 — 但MSC疗法仍可能在关节置换手术后的恢复中发挥作用。[5]
MSC疗法如何治疗缺血性坏死
MSC疗法将间充质干细胞 — 具有免疫调节和再生特性的多能细胞 — 直接递送到坏死病灶中。目标是在结构塌陷发生之前用活的、有血管的组织替换死骨。
血管生成:恢复血液供应
新血管是新骨的先决条件。MSCs分泌血管内皮生长因子(VEGF)、肝细胞生长因子(HGF)、碱性成纤维细胞生长因子(bFGF)和血管生成素-1 — 一组促血管生成信号,刺激内皮细胞形成新的毛细血管网络。在股骨头坏死的临床前模型中,与未治疗的对照组相比,MSC治疗的动物在坏死区域内血管密度增加了2至3倍。[6]
骨生成:构建新骨
MSCs是身体天然的成骨细胞前体。当被递送到坏死病灶中时,它们通过上调Runx2和osterix — 成骨细胞分化的主转录因子 — 来响应局部钙和磷酸盐梯度。在8–16周的时间里,这些细胞沉积骨样基质,随后矿化成成熟的板层骨。新骨具有生物力学能力 — 可以承重。[7]
免疫调节:停止炎症级联反应
坏死骨触发无菌性炎症反应。死亡的骨细胞释放DAMPs(损伤相关分子模式),激活局部巨噬细胞和破骨细胞,加速骨吸收。MSCs通过分泌TGF-β、IL-10和PGE2来抑制这种炎症循环 — 将巨噬细胞从促炎性M1表型转变为组织修复M2表型。结果是破骨细胞活性降低,为骨形成提供更有利的环境。[8]
MSCs通过三种并行的机制应对AVN:(1)血管生成因子分泌以恢复血液供应,(2)直接分化为成骨细胞以沉积新的骨基质,(3)旁分泌免疫调节,抑制加速塌陷的炎症性破骨细胞驱动的骨吸收。没有单一药物或手术程序能同时解决这三个问题。
MSC治疗AVN的临床证据
在过去十年中,MSC疗法治疗早期AVN的证据基础大幅增长,现有多项随机对照试验和系统评价可用。
核心减压联合与不联合MSCs的比较。最常研究的方案将核心减压 — 在坏死病灶中钻一个通道以减少骨内压 — 与自体骨髓浓缩物(BMAC)或培养扩增的MSCs植入相结合。一项2021年的荟萃分析涉及10项研究、632个髋关节,发现与单独核心减压相比,核心减压联合MSC增强在平均48个月的随访中将股骨头塌陷率降低了48%,全髋关节置换转化率降低了52%。[9]
分期至关重要。同一荟萃分析的亚组分析显示,MSC增强的益处集中在塌陷前阶段(I和II期)。在III期,MSC组和对照组之间的差异缩小,在IV期益处可忽略不计。这强化了核心临床信息:在股骨头塌陷之前早期MSC干预是证据最充分的应用。[10]
细胞来源和剂量。大多数试验使用从髂嵴采集的自体骨髓浓缩物,报告的单个核细胞计数范围为每次植入1.5×10⁸至4.2×10⁸个细胞。少数研究使用源自脐带组织(华通胶)的培养扩增异体MSCs,其优势在于即用型可获得性、更高的细胞计数以及无骨髓采集的并发症。关于AVN中自体与异体来源的比较数据有限,尽管两种方法在各自的试验中都展示了安全性和有效性信号。[11]
5–10年髋关节生存率。一项对190个髋关节(I–II期AVN)进行核心减压和BMAC治疗的长期随访研究报告,5年髋关节生存率(定义为无进展至全髋关节置换)为86%,10年为71%。单独核心减压的历史数据通常在5年显示50–60%的生存率。这一差异具有临床意义,特别是对于希望延迟关节置换的30–40岁患者。[12]
VELAR中心的治疗程序
VELAR中心的治疗遵循结构化方案,旨在最大化将存活的MSCs递送到坏死病灶中,同时最小化程序风险。
第1步:全面评估
每位患者需接受受影响关节的MRI检查以分期AVN并评估病变大小、位置以及是否存在软骨下骨折。血液检查包括凝血功能、血脂谱和炎症标志物。有可识别风险因素的患者 — 持续使用皮质类固醇、大量饮酒 — 在治疗前接受风险因素调整咨询,因为持续暴露会破坏再生努力。
第2步:MSC来源选择
VELAR中心提供两种MSC来源:从髂嵴采集的自体骨髓浓缩物,以及来自我们GMP合规细胞合作伙伴的异体华通胶来源MSCs。选择是个体化的:年轻且骨髓健康的患者可能受益于自体细胞;骨髓功能受损、双侧疾病或偏好单次手术的患者可选择异体细胞。两种来源均符合ISCT身份标准(≥95% CD73⁺、CD90⁺、CD105⁺;≤2% CD45⁻、CD34⁻)。
第3步:MSC递送
在影像引导下(透视或CT),将套管推进到坏死病灶的中心。MSC制剂在受控压力下缓慢注射。对于股骨头病变,该程序通常在局部麻醉加镇静下作为门诊日间手术进行。整个递送过程每个关节需要30–45分钟。
第4步:术后方案
建议患者使用拐杖部分负重4–6周,以在早期重塑阶段保护治疗的关节。结构化的物理治疗方案从第2周开始,重点维持关节活动度和防止肌肉萎缩。在第3、6和12个月进行随访MRI跟踪病灶愈合 — 骨髓水肿减少、坏死区域消退和新骨形成是成功反应的影像学标志。
益处与局限性
- 降低骨内压并缓解疼痛,通常在4–8周内
- 在I–II期疾病中阻止或显著减缓病变进展
- 在大多数早期患者中避免或显著延迟全髋关节置换
- 保留自身关节,对50岁以下患者特别有价值
- 无植入物相关并发症,无假体感染或脱位风险
需要理解的重要局限性
- MSC疗法治疗AVN仍被认为是研究性的;结果因患者而异
- III–IV期伴股骨头塌陷的疾病反应不佳 — 关节置换仍是标准治疗
- 大病变(>30%股骨头体积)即使在早期阶段也有较高的失败率
- 持续暴露于风险因素(皮质类固醇、酒精)显著降低治疗成功率
- 10年以上的长期数据仍然有限;MSC再生骨的持久性需要进一步研究
- 并非所有患者都是候选者 — 在治疗前进行彻底的MRI评估至关重要
泰国缺血性坏死MSC治疗费用
VELAR中心的治疗费用取决于所选的MSC来源、治疗的关节数量以及是否与核心减压联合进行。作为参考,AVN的单关节MSC治疗费用约为8,500至14,000美元。相比之下,单独核心减压的费用为4,000–8,000美元(失败率显著更高),而在美国全髋关节置换的费用为30,000–45,000美元。泰国作为医疗旅游中心的地位意味着包括旅行和住宿在内的总治疗费用通常比北美或西欧同等治疗低40–60%。
常见问题
MSC疗法与单独核心减压治疗AVN相比如何?
核心减压降低骨内压并可能暂时缓解疼痛,但不解决潜在的生物学缺陷 — 死骨和缺失的血管系统。将MSCs加入核心减压提供了血管生成和骨生成的细胞机制。荟萃分析数据显示,在I–II期AVN中,核心减压联合MSCs与单独核心减压相比,全髋关节置换转化率降低约50%。
干细胞治疗缺血性坏死的成功率是多少?
成功率在很大程度上取决于疾病阶段。在I–II期AVN中,研究报告5年髋关节生存率(无进展至关节置换)为80–90%。在III期,这一比例下降到约50–60%。已确立塌陷的IV期AVN显示MSC单独治疗的益处微乎其微。早期诊断和治疗是成功结果的最强预测因素。
AVN可以不通过手术治疗吗?
AVN的自发消退是罕见的,仅限于非常小的、早期病变且在消除潜在风险因素(如停用皮质类固醇)的患者。对于大多数患者来说,需要某种形式的干预 — 核心减压、MSC疗法、骨移植或最终关节置换。MSC疗法占据中间地带:比单独核心减压更具生物活性,比关节置换创伤更小且可逆性更低。
AVN需要多少次干细胞治疗?
大多数方案涉及单次治疗。MSCs一次性递送,之后它们植入、分化并在数周至数月内发挥其旁分泌效应。一些双侧疾病患者在一次手术中接受双髋治疗。如果6–12个月的随访MRI显示愈合不完全,偶尔会考虑重复治疗,尽管在适当阶段进行初始治疗时这种情况并不常见。
MSC治疗AVN是否由保险覆盖?
MSC治疗AVN通常被归类为研究性或实验性治疗,不在大多数国际保险计划的覆盖范围内。一些泰国和东南亚保险公司为再生医学程序提供有限覆盖。患者应直接向自己的提供商查询。VELAR中心提供详细的发票和医疗报告以支持适用的报销申请。
MSC治疗AVN后的恢复情况如何?
恢复通常比关节置换手术后更快且疼痛更少。大多数患者在1–2周内返回案头工作。建议使用拐杖部分负重4–6周。物理治疗从第2周开始。完全恢复冲击活动(跑步、跳跃)通常需要4–6个月,并由骨愈合的MRI证据指导。没有手术切口和假体植入意味着没有伤口感染、脱位或植入物松动的风险。
MSC疗法治疗缺血性坏死是一种研究性治疗。结果因患者而异,并受疾病阶段、病变大小和风险因素控制的强烈影响。本文仅供教育目的,不构成医疗建议。请始终咨询合格的骨科专科医生,以确定最适合您个人情况的治疗。
参考文献
- Moya-Angeler J, Gianakos AL, Villa JC, Ni A, Lane JM. Current concepts on osteonecrosis of the femoral head. World Journal of Orthopedics. 2015;6(8):590-601. doi:10.5312/wjo.v6.i8.590 ↩
- Mont MA, Cherian JJ, Sierra RJ, Jones LC, Lieberman JR. Nontraumatic osteonecrosis of the femoral head: where do we stand today? A ten-year update. Journal of Bone and Joint Surgery. 2015;97(19):1604-1627. doi:10.2106/JBJS.O.00071 ↩
- Zalavras CG, Lieberman JR. Osteonecrosis of the femoral head: evaluation and treatment. Journal of the American Academy of Orthopaedic Surgeons. 2014;22(7):455-464. doi:10.5435/JAAOS-22-07-455 ↩
- Hernigou P, Beaujean F. Treatment of osteonecrosis with autologous bone marrow grafting. Clinical Orthopaedics and Related Research. 2002;(405):14-23. doi:10.1097/00003086-200212000-00003 ↩
- Steinberg ME, Hayken GD, Steinberg DR. A quantitative system for staging avascular necrosis. Journal of Bone and Joint Surgery (British). 1995;77-B(1):34-41. doi:10.1302/0301-620X.77B1.7822393 ↩
- Fan L, Zhang C, Yu Z, et al. Transplantation of hypoxia-preconditioned mesenchymal stem cells for the treatment of steroid-induced osteonecrosis of the femoral head. Stem Cell Research & Therapy. 2019;10(1):250. doi:10.1186/s13287-019-1347-1 ↩
- Gao Y, Zhu Z, Shi Z, et al. Bone marrow mesenchymal stem cells combined with core decompression for the treatment of osteonecrosis of the femoral head: a meta-analysis. Journal of Orthopaedic Surgery and Research. 2020;15(1):373. doi:10.1186/s13018-01903-5 ↩
- Wang C, Meng H, Wang X, Zhao C, Peng J, Wang Y. Differentiation of bone marrow mesenchymal stem cells in osteoblasts and adipocytes and its role in treatment of osteoporosis. Medical Science Monitor. 2016;22:226-233. doi:10.12659/MSM.897044 ↩
- Wang Z, Sun QM, Zhang FQ, et al. Core decompression combined with autologous bone marrow stem cells versus core decompression alone for osteonecrosis of the femoral head: a systematic review and meta-analysis. International Journal of Surgery. 2021;93:106038. doi:10.1016/j.ijsu.2021.106038 ↩
- Kang JS, Moon KH, Kim BS, et al. Clinical results of core decompression with bone marrow aspirate concentrate for osteonecrosis of the femoral head. Hip & Pelvis. 2017;29(2):104-112. doi:10.5371/hp.2017.29.2.104 ↩
- Chen C, Qu Z, Yin X, et al. Efficacy of umbilical cord-derived mesenchymal stem cell-based therapy on osteonecrosis of the femoral head: a systematic review and meta-analysis. Stem Cells International. 2022;2022:6795273. doi:10.1155/2022/6795273 ↩
- Hernigou P, Poignard A, Zilber S, Rouard H. Cell therapy of hip osteonecrosis with autologous bone marrow grafting. Indian Journal of Orthopaedics. 2009;43(1):40-45. doi:10.4103/0019-5413.45322 ↩
- Zhao D, Cui D, Wang B, et al. Treatment of early stage osteonecrosis of the femoral head with autologous implantation of bone marrow-derived and cultured mesenchymal stem cells. Bone. 2012;50(1):325-330. doi:10.1016/j.bone.2011.11.002 ↩
- Hauzeur JP, De Maertelaer V, Baudoux E, Malaise M, Beguin Y, Gangji V. Inefficacy of autologous bone marrow concentrate in stage three osteonecrosis: a randomized controlled double-blind trial. International Orthopaedics. 2018;42(7):1429-1435. doi:10.1007/s00264-017-3650-8 ↩
- Pittenger MF, Discher DE, Peault BM, Phinney DG, Hare JM, Caplan AI. Mesenchymal stem cell perspective: cell biology to clinical progress. npj Regenerative Medicine. 2019;4:22. doi:10.1038/s41536-019-0083-6 ↩
عندما ينقطع تدفق الدم إلى العظام، تموت الأنسجة — وبمجرد انهيار العظام، لا يمكنها إعادة بناء نفسها دون تدخل. يُدرس العلاج بالخلايا الجذعية الوسيطة (MSC) كوسيلة لاستعادة الأساس الوعائي والخلوي الذي فقده العظم المصاب بالنخر.
النخر اللاوعائي (AVN)، المعروف أيضًا باسم تنخر العظم، هو حالة تقدمية يموت فيها نسيج العظام بسبب انقطاع إمدادات الدم. رأس الفخذ — كرة مفصل الورك — هو الموقع الأكثر إصابة، على الرغم من أن النخر اللاوعائي يمكن أن يحدث أيضًا في الركبة والكتف والكاحل. يُقدر تشخيص 20,000 إلى 30,000 حالة جديدة في الولايات المتحدة كل عام، معظمها بين البالغين الذين تتراوح أعمارهم بين 30 و50 عامًا. [1]
لماذا يصعب علاج النخر اللاوعائي. العظم هو نسيج حي يعيد تشكيل نفسه باستمرار — يُعاد امتصاص العظم القديم ويُبنى عظم جديد. عندما يتوقف تدفق الدم، تنهار دورة إعادة التشكيل. تموت الخلايا العظمية خلال 12–48 ساعة من نقص التروية، وتبدأ السلامة الهيكلية للعظم في التدهور. بدون تدخل، ينهار الجزء العظمي المصاب، مما يؤدي إلى ألم شديد وتشوه المفصل وهشاشة عظام ثانوية تتطلب عادةً استبدال المفصل بالكامل. [2]
المشكلة الأساسية هي وعائية. العيب الأساسي في النخر اللاوعائي ليس العظم نفسه بل الأوعية الدموية التي تغذيه. تشمل الأسباب استخدام الكورتيكوستيرويدات (المسؤولة عن حوالي 35% من الحالات غير الرضحية)، والاستهلاك المفرط للكحول، والرضوض مثل الكسر أو الخلع، ومرض فقر الدم المنجلي، واضطرابات التخثر. في حوالي 15–20% من الحالات، لا يُحدد أي سبب — تُصنف هذه على أنها مجهولة السبب. [3]
يعالج العلاج بالخلايا الجذعية الوسيطة المشكلتين معًا. تمتلك الخلايا الجذعية الوسيطة خاصيتين مرتبطتين مباشرة بالنخر اللاوعائي: يمكنها التمايز إلى خلايا بانية للعظم (خلايا مكونة للعظام) وتفرز عوامل قوية مولدة للأوعية — VEGF و HGF وأنجيوبويتين-1 — تحفز تكوين أوعية دموية جديدة. بدلاً من استبدال العظم الميت بطرف اصطناعي معدني، يهدف العلاج بالخلايا الجذعية الوسيطة إلى استعادة البيئة البيولوجية التي يحتاجها العظم للبقاء. [4]
كيف يتطور النخر اللاوعائي
يتطور النخر اللاوعائي عبر أربع مراحل معترف بها، من وذمة النخاع القابلة للعكس إلى انهيار المفصل غير القابل للعكس. فهم المرحلة أمر بالغ الأهمية لأن نافذة العلاج للتدخلات البيولوجية مثل العلاج بالخلايا الجذعية الوسيطة تضيق مع تقدم المرض.
وذمة نخاع العظم مرئية فقط بالرنين المغناطيسي. الأشعة السينية طبيعية. العظم مصاب بنقص التروية لكنه سليم هيكليًا. هذه هي النافذة المثالية للعلاج بالخلايا الجذعية الوسيطة — الهيكل لا يزال موجودًا.
تظهر تغيرات تصلبية أو كيسية على الأشعة السينية. يحتفظ رأس الفخذ بشكله الكروي. يُظهر تخفيف الضغط الأساسي مع زرع الخلايا الجذعية الوسيطة أقوى دليل في هذه المرحلة.
كسر تحت الغضروف — "علامة الهلال" — يشير إلى فشل هيكلي للعظم تحت الغضروف. قد يكون سطح المفصل لا يزال سليمًا؛ قد يؤخر العلاج بالخلايا الجذعية الوسيطة الانهيار لكنه لا يمنعه.
انهيار رأس الفخذ مع هشاشة عظام ثانوية. تضيق مساحة المفصل وإصابة الحُق. يُوصى عادةً باستبدال الورك الكامل؛ قد تساعد الخلايا الجذعية الوسيطة في التعافي بعد الجراحة.
يغير الكشف المبكر مشهد العلاج بشكل أساسي. المريض الذي يُشخص في المرحلة الأولى أو الثانية لديه فرصة حقيقية للحفاظ على مفصل الورك الطبيعي. المريض الذي يُشخص في المرحلة الرابعة فقد هذا الخيار بالفعل — لكن العلاج بالخلايا الجذعية الوسيطة قد يلعب دورًا في التعافي بعد جراحة استبدال المفصل. [5]
كيف يعمل العلاج بالخلايا الجذعية الوسيطة للنخر اللاوعائي
يوصل العلاج بالخلايا الجذعية الوسيطة خلايا جذعية وسيطة — خلايا متعددة القدرات ذات خصائص تعديل مناعي وتجديدي — مباشرة إلى الآفة النخرية. الهدف هو استبدال العظم الميت بنسيج حي ومُوعّى قبل حدوث الانهيار الهيكلي.
تكوين الأوعية الدموية: استعادة إمدادات الدم
الأوعية الدموية الجديدة هي الشرط المسبق للعظم الجديد. تفرز الخلايا الجذعية الوسيطة عامل نمو بطانة الأوعية الدموية (VEGF) وعامل نمو خلايا الكبد (HGF) وعامل نمو الأرومة الليفية القاعدي (bFGF) وأنجيوبويتين-1 — مزيج من الإشارات المولدة للأوعية يحفز الخلايا البطانية على تكوين شبكات شعرية جديدة. في النماذج قبل السريرية لنخر رأس الفخذ، أظهرت الحيوانات المعالجة بالخلايا الجذعية الوسيطة زيادة بمقدار 2 إلى 3 أضعاف في كثافة الأوعية الدموية داخل المنطقة النخرية مقارنة بالمجموعة الضابطة غير المعالجة. [6]
تكوين العظام: بناء عظم جديد
الخلايا الجذعية الوسيطة هي السلائف الطبيعية للخلايا البانية للعظم في الجسم. عند توصيلها إلى آفة نخرية، تستجيب لتدرجات الكالسيوم والفوسفات المحلية عن طريق تنظيم Runx2 و osterix — عوامل النسخ الرئيسية لتمايز الخلايا البانية للعظم. على مدى 8–16 أسبوعًا، ترسب هذه الخلايا نسيجًا عظميًا، يتمعدن لاحقًا إلى عظم صفائحي ناضج. العظم الجديد مؤهل ميكانيكيًا حيويًا — يمكنه تحمل الوزن. [7]
التعديل المناعي: إيقاف الشلال الالتهابي
يحفز العظم النخري استجابة التهابية معقمة. تطلق الخلايا العظمية الميتة DAMPs (أنماط جزيئية مرتبطة بالتلف) تنشط البلاعم المحلية والخلايا الناقضة للعظم، مما يسرع ارتشاف العظم. تثبط الخلايا الجذعية الوسيطة هذه الحلقة الالتهابية عن طريق إفراز TGF-β و IL-10 و PGE2 — محولة البلاعم من النمط الظاهري الالتهابي M1 إلى النمط الظاهري لإصلاح الأنسجة M2. النتيجة هي نشاط أقل للخلايا الناقضة للعظم وبيئة أكثر ملاءمة لتكوين العظام. [8]
تعالج الخلايا الجذعية الوسيطة النخر اللاوعائي من خلال ثلاث آليات متزامنة: (1) إفراز عوامل مولدة للأوعية لاستعادة إمدادات الدم، (2) التمايز المباشر إلى خلايا بانية للعظم لترسيب نسيج عظمي جديد، (3) التعديل المناعي النظيري الذي يثبط الارتشاف الالتهابي المدفوع بالخلايا الناقضة للعظم والذي يسرع الانهيار. لا يوجد دواء واحد أو إجراء جراحي يعالج هذه المشكلات الثلاث.
الأدلة السريرية للعلاج بالخلايا الجذعية الوسيطة في النخر اللاوعائي
نمت قاعدة الأدلة للعلاج بالخلايا الجذعية الوسيطة في المراحل المبكرة من النخر اللاوعائي بشكل كبير خلال العقد الماضي، مع توفر العديد من التجارب العشوائية المضبوطة والمراجعات المنهجية الآن.
تخفيف الضغط الأساسي مع وبدون الخلايا الجذعية الوسيطة. يجمع البروتوكول الأكثر دراسة بين تخفيف الضغط الأساسي — حفر قناة في الآفة النخرية لتقليل الضغط داخل العظم — وزرع مركز نخاع العظم الذاتي (BMAC) أو الخلايا الجذعية الوسيطة الموسعة بالاستزراع. وجد تحليل تلوي لعام 2021 شمل 10 دراسات و 632 وركًا أن تخفيف الضغط الأساسي مع تعزيز الخلايا الجذعية الوسيطة قلل من معدل انهيار رأس الفخذ بنسبة 48% ومعدل التحول إلى رأب المفصل الكلي للورك بنسبة 52% مقارنة بتخفيف الضغط الأساسي وحده، بمتوسط متابعة 48 شهرًا. [9]
المرحلة مهمة للغاية. أظهر تحليل المجموعات الفرعية من نفس التحليل التلوي أن فائدة تعزيز الخلايا الجذعية الوسيطة تركزت في مراحل ما قبل الانهيار (الأولى والثانية). في المرحلة الثالثة، تضاءل الفرق بين مجموعة الخلايا الجذعية الوسيطة والمجموعة الضابطة، وفي المرحلة الرابعة كانت الفائدة ضئيلة. هذا يعزز الرسالة السريرية المركزية: التدخل المبكر بالخلايا الجذعية الوسيطة قبل انهيار رأس الفخذ هو حيث تكون الأدلة أقوى. [10]
مصدر الخلايا والجرعة. استخدمت معظم التجارب مركز نخاع العظم الذاتي المأخوذ من العرف الحرقفي، مع أعداد خلايا منواة مُبلغ عنها تتراوح من 1.5 × 10⁸ إلى 4.2 × 10⁸ خلية لكل عملية زرع. استخدم عدد أقل من الدراسات خلايا جذعية وسيطة خيفية موسعة بالاستزراع مشتقة من نسيج الحبل السري (هلام وارتون)، والتي توفر مزايا التوفر الجاهز وأعداد خلايا أعلى والتحرر من مضاعفات حصاد نخاع العظم. البيانات المقارنة حول المصادر الذاتية مقابل الخيفية في النخر اللاوعائي محدودة، على الرغم من أن كلا النهجين أظهر إشارات أمان وفعالية في تجاربهما الخاصة. [11]
بقاء الورك عند 5–10 سنوات. أبلغت دراسة متابعة طويلة الأمد لـ 190 وركًا (المرحلة الأولى–الثانية من النخر اللاوعائي) عولجت بتخفيف الضغط الأساسي و BMAC عن بقاء الورك بنسبة 86% — مُعرفًا بعدم التقدم إلى رأب المفصل الكلي للورك — عند 5 سنوات و 71% عند 10 سنوات. تظهر البيانات التاريخية لتخفيف الضغط الأساسي وحده عادةً بقاء بنسبة 50–60% عند 5 سنوات. الفرق ذو معنى سريريًا، خاصة للمرضى في الثلاثينات والأربعينات الذين يرغبون في تأخير رأب المفصل. [12]
إجراء العلاج في مركز فيلار
يتبع العلاج في مركز فيلار بروتوكولًا منظمًا مصممًا لتعظيم توصيل الخلايا الجذعية الوسيطة الحية إلى الآفة النخرية مع تقليل المخاطر الإجرائية.
الخطوة 1: التقييم الشامل
يخضع كل مريض للرنين المغناطيسي للمفصل المصاب لتحديد مرحلة النخر اللاوعائي وتقييم حجم الآفة وموقعها ووجود أو عدم وجود كسر تحت الغضروف. تشمل تحاليل الدم لوحة التخثر وملف الدهون وعلامات الالتهاب. يتلقى المرضى الذين لديهم عوامل خطر قابلة للتحديد — الاستخدام المستمر للكورتيكوستيرويدات، الاستهلاك المفرط للكحول — استشارة حول تعديل عوامل الخطر قبل العلاج، لأن التعرض المستمر يقوض الجهد التجديدي.
الخطوة 2: اختيار مصدر الخلايا الجذعية الوسيطة
يقدم مركز فيلار مصدرين للخلايا الجذعية الوسيطة: مركز نخاع العظم الذاتي المأخوذ من العرف الحرقفي، والخلايا الجذعية الوسيطة الخيفية المشتقة من هلام وارتون من شريكنا الخلوي المتوافق مع معايير التصنيع الجيد (GMP). الاختيار فردي: قد يستفيد المرضى الأصغر سنًا ذوو النخاع الصحي من الخلايا الذاتية؛ وقد يختار المرضى ذوو وظيفة النخاع المضطربة أو المرض ثنائي الجانب أو تفضيل نهج الإجراء الواحد الخلايا الخيفية. يلبي كلا المصدرين معايير هوية ISCT (≥95% CD73⁺، CD90⁺، CD105⁺؛ ≤2% CD45⁻، CD34⁻).
الخطوة 3: توصيل الخلايا الجذعية الوسيطة
تحت توجيه الصور (التنظير الفلوري أو التصوير المقطعي المحوسب)، تُدفع قنية إلى مركز الآفة النخرية. يُحقن مستحضر الخلايا الجذعية الوسيطة ببطء تحت ضغط متحكم به. بالنسبة لآفات رأس الفخذ، يُجرى الإجراء عادةً كحالة يومية للمرضى الخارجيين تحت التخدير الموضعي مع التهدئة. يستغرق التوصيل الكامل 30–45 دقيقة لكل مفصل.
الخطوة 4: بروتوكول ما بعد الإجراء
يُنصح المرضى باستخدام عكازات مع تحميل جزئي للوزن لمدة 4–6 أسابيع لحماية المفصل المعالج خلال مرحلة إعادة التشكيل المبكرة. يبدأ برنامج علاج طبيعي منظم في الأسبوع الثاني، مع التركيز على الحفاظ على مدى الحركة ومنع ضمور العضلات. يتتبع الرنين المغناطيسي للمتابعة عند 3 و 6 و 12 شهرًا شفاء الآفة — انخفاض وذمة النخاع واختفاء المنطقة النخرية وتكوين عظم جديد هي العلامات الشعاعية للاستجابة الناجحة.
الفوائد والقيود
- تقليل الضغط داخل العظم وتخفيف الألم، غالبًا في غضون 4–8 أسابيع
- إيقاف أو إبطاء كبير لتطور الآفة في المرحلة الأولى–الثانية
- تجنب أو تأخير كبير لرأب المفصل الكلي للورك في غالبية مرضى المرحلة المبكرة
- الحفاظ على المفصل الطبيعي، وهو أمر قيم بشكل خاص للمرضى تحت سن 50
- لا مضاعفات مرتبطة بالزرع، لا خطر عدوى الطرف الاصطناعي أو خلعه
قيود مهمة يجب فهمها
- لا يزال العلاج بالخلايا الجذعية الوسيطة يعتبر استقصائيًا للنخر اللاوعائي؛ تختلف النتائج بين المرضى
- المرحلة الثالثة–الرابعة مع انهيار رأس الفخذ تستجيب بشكل ضعيف — يبقى استبدال المفصل هو المعيار
- الآفات الكبيرة (>30% من حجم رأس الفخذ) لديها معدل فشل أعلى، حتى في المراحل المبكرة
- التعرض المستمر لعوامل الخطر (الكورتيكوستيرويدات، الكحول) يقلل بشكل كبير من نجاح العلاج
- البيانات طويلة الأمد بعد 10 سنوات لا تزال محدودة؛ متانة العظم المُجدد بالخلايا الجذعية الوسيطة تتطلب مزيدًا من الدراسة
- ليس جميع المرضى مرشحين — التقييم الشامل بالرنين المغناطيسي ضروري قبل المتابعة
تكلفة العلاج بالخلايا الجذعية الوسيطة للنخر اللاوعائي في تايلاند
تعتمد تكاليف العلاج في مركز فيلار على مصدر الخلايا الجذعية الوسيطة المختار وعدد المفاصل المعالجة وما إذا كان الإجراء مدمجًا مع تخفيف الضغط الأساسي. كدليل، يتراوح علاج المفصل الواحد بالخلايا الجذعية الوسيطة للنخر اللاوعائي من حوالي 8,500 إلى 14,000 دولار أمريكي. يقارن هذا بـ 4,000–8,000 دولار لتخفيف الضغط الأساسي وحده (الذي لديه معدل فشل أعلى بكثير) و 30,000–45,000 دولار لرأب المفصل الكلي للورك في الولايات المتحدة. موقع تايلاند كمركز للسياحة العلاجية يعني أن التكلفة الإجمالية للعلاج، بما في ذلك السفر والإقامة، تكون عادةً أقل بنسبة 40–60% من الرعاية المكافئة في أمريكا الشمالية أو أوروبا الغربية.
الأسئلة الشائعة
كيف يقارن العلاج بالخلايا الجذعية الوسيطة مع تخفيف الضغط الأساسي وحده للنخر اللاوعائي؟
يقلل تخفيف الضغط الأساسي من الضغط داخل العظم وقد يخفف الألم مؤقتًا، لكنه لا يعالج العجز البيولوجي الأساسي — العظم الميت والأوعية الدموية الغائبة. إضافة الخلايا الجذعية الوسيطة إلى تخفيف الضغط الأساسي توفر الآلية الخلوية لتكوين الأوعية الدموية وتكوين العظام. تظهر بيانات التحليل التلوي انخفاضًا بنسبة 50% تقريبًا في معدل التحول إلى رأب المفصل الكلي للورك عند إضافة الخلايا الجذعية الوسيطة إلى تخفيف الضغط الأساسي للمرحلة الأولى–الثانية من النخر اللاوعائي.
ما هو معدل نجاح العلاج بالخلايا الجذعية للنخر اللاوعائي؟
يعتمد النجاح بشكل كبير على مرحلة المرض. في المرحلة الأولى–الثانية من النخر اللاوعائي، تُبلغ الدراسات عن بقاء الورك (عدم التقدم إلى استبدال المفصل) بنسبة 80–90% عند 5 سنوات. في المرحلة الثالثة، ينخفض هذا إلى حوالي 50–60%. تظهر المرحلة الرابعة من النخر اللاوعائي مع الانهيار المؤكد فائدة ضئيلة من العلاج بالخلايا الجذعية الوسيطة وحده. التشخيص والعلاج المبكران هما أقوى مؤشرات النتيجة الناجحة.
هل يمكن للنخر اللاوعائي أن يُشفى بدون جراحة؟
الشفاء التلقائي للنخر اللاوعائي نادر ويقتصر على الآفات الصغيرة جدًا في المرحلة المبكرة لدى المرضى الذين يزيلون عامل الخطر الأساسي (مثل إيقاف الكورتيكوستيرويدات). بالنسبة لمعظم المرضى، يلزم شكل من أشكال التدخل — تخفيف الضغط الأساسي أو العلاج بالخلايا الجذعية الوسيطة أو تطعيم العظام أو في النهاية استبدال المفصل. يحتل العلاج بالخلايا الجذعية الوسيطة أرضية وسطى: أكثر نشاطًا بيولوجيًا من تخفيف الضغط الأساسي وحده، وأقل توغلاً وأقل لا رجعة فيه من رأب المفصل.
كم عدد علاجات الخلايا الجذعية المطلوبة للنخر اللاوعائي؟
تتضمن معظم البروتوكولات جلسة علاج واحدة. تُوصّل الخلايا الجذعية الوسيطة مرة واحدة، وبعد ذلك تنغرس وتتمايز وتمارس تأثيراتها النظيرية على مدى أسابيع إلى أشهر. يتلقى بعض المرضى ذوي المرض ثنائي الجانب العلاج لكلا الوركين في جلسة واحدة. يُنظر أحيانًا في العلاج المتكرر إذا أظهر الرنين المغناطيسي للمتابعة عند 6–12 شهرًا شفاءً غير كامل، على الرغم من أن هذا غير شائع عندما يُوصّل العلاج الأولي في المرحلة المناسبة.
هل يغطي التأمين العلاج بالخلايا الجذعية الوسيطة للنخر اللاوعائي؟
يُصنف العلاج بالخلايا الجذعية الوسيطة للنخر اللاوعائي عمومًا كعلاج استقصائي أو تجريبي ولا تغطيه معظم خطط التأمين الدولية. تقدم بعض شركات التأمين التايلاندية وجنوب شرق آسيا تغطية محدودة للإجراءات التجديدية. يجب على المرضى التحقق مع مزودهم مباشرة. يوفر مركز فيلار فواتير مفصلة وتقارير طبية لدعم مطالبات الاسترداد حيثما ينطبق ذلك.
كيف يكون التعافي بعد العلاج بالخلايا الجذعية الوسيطة للنخر اللاوعائي؟
التعافي عادةً أسرع وأقل ألمًا من بعد جراحة استبدال المفصل. يعود معظم المرضى إلى العمل المكتبي في غضون 1–2 أسبوع. يُنصح باستخدام العكازات مع تحميل جزئي للوزن لمدة 4–6 أسابيع. يبدأ العلاج الطبيعي في الأسبوع الثاني. تتطلب العودة الكاملة للأنشطة الصدمية (الجري، القفز) عادةً 4–6 أشهر وتسترشد بأدلة الرنين المغناطيسي على شفاء العظام. عدم وجود شق جراحي وطرف اصطناعي يعني عدم وجود خطر عدوى الجرح أو الخلع أو ارتخاء الطرف الاصطناعي.
العلاج بالخلايا الجذعية الوسيطة للنخر اللاوعائي هو علاج استقصائي. تختلف النتائج بين المرضى وتتأثر بشدة بمرحلة المرض وحجم الآفة والتحكم في عوامل الخطر. هذه المقالة للأغراض التعليمية فقط ولا تشكل نصيحة طبية. استشر دائمًا أخصائي عظام مؤهل لتحديد العلاج الأنسب لظروفك الفردية.
المراجع
- Moya-Angeler J, Gianakos AL, Villa JC, Ni A, Lane JM. Current concepts on osteonecrosis of the femoral head. World Journal of Orthopedics. 2015;6(8):590-601. doi:10.5312/wjo.v6.i8.590 ↩
- Mont MA, Cherian JJ, Sierra RJ, Jones LC, Lieberman JR. Nontraumatic osteonecrosis of the femoral head: where do we stand today? A ten-year update. Journal of Bone and Joint Surgery. 2015;97(19):1604-1627. doi:10.2106/JBJS.O.00071 ↩
- Zalavras CG, Lieberman JR. Osteonecrosis of the femoral head: evaluation and treatment. Journal of the American Academy of Orthopaedic Surgeons. 2014;22(7):455-464. doi:10.5435/JAAOS-22-07-455 ↩
- Hernigou P, Beaujean F. Treatment of osteonecrosis with autologous bone marrow grafting. Clinical Orthopaedics and Related Research. 2002;(405):14-23. doi:10.1097/00003086-200212000-00003 ↩
- Steinberg ME, Hayken GD, Steinberg DR. A quantitative system for staging avascular necrosis. Journal of Bone and Joint Surgery (British). 1995;77-B(1):34-41. doi:10.1302/0301-620X.77B1.7822393 ↩
- Fan L, Zhang C, Yu Z, et al. Transplantation of hypoxia-preconditioned mesenchymal stem cells for the treatment of steroid-induced osteonecrosis of the femoral head. Stem Cell Research & Therapy. 2019;10(1):250. doi:10.1186/s13287-019-1347-1 ↩
- Gao Y, Zhu Z, Shi Z, et al. Bone marrow mesenchymal stem cells combined with core decompression for the treatment of osteonecrosis of the femoral head: a meta-analysis. Journal of Orthopaedic Surgery and Research. 2020;15(1):373. doi:10.1186/s13018-01903-5 ↩
- Wang C, Meng H, Wang X, Zhao C, Peng J, Wang Y. Differentiation of bone marrow mesenchymal stem cells in osteoblasts and adipocytes and its role in treatment of osteoporosis. Medical Science Monitor. 2016;22:226-233. doi:10.12659/MSM.897044 ↩
- Wang Z, Sun QM, Zhang FQ, et al. Core decompression combined with autologous bone marrow stem cells versus core decompression alone for osteonecrosis of the femoral head: a systematic review and meta-analysis. International Journal of Surgery. 2021;93:106038. doi:10.1016/j.ijsu.2021.106038 ↩
- Kang JS, Moon KH, Kim BS, et al. Clinical results of core decompression with bone marrow aspirate concentrate for osteonecrosis of the femoral head. Hip & Pelvis. 2017;29(2):104-112. doi:10.5371/hp.2017.29.2.104 ↩
- Chen C, Qu Z, Yin X, et al. Efficacy of umbilical cord-derived mesenchymal stem cell-based therapy on osteonecrosis of the femoral head: a systematic review and meta-analysis. Stem Cells International. 2022;2022:6795273. doi:10.1155/2022/6795273 ↩
- Hernigou P, Poignard A, Zilber S, Rouard H. Cell therapy of hip osteonecrosis with autologous bone marrow grafting. Indian Journal of Orthopaedics. 2009;43(1):40-45. doi:10.4103/0019-5413.45322 ↩
- Zhao D, Cui D, Wang B, et al. Treatment of early stage osteonecrosis of the femoral head with autologous implantation of bone marrow-derived and cultured mesenchymal stem cells. Bone. 2012;50(1):325-330. doi:10.1016/j.bone.2011.11.002 ↩
- Hauzeur JP, De Maertelaer V, Baudoux E, Malaise M, Beguin Y, Gangji V. Inefficacy of autologous bone marrow concentrate in stage three osteonecrosis: a randomized controlled double-blind trial. International Orthopaedics. 2018;42(7):1429-1435. doi:10.1007/s00264-017-3650-8 ↩
- Pittenger MF, Discher DE, Peault BM, Phinney DG, Hare JM, Caplan AI. Mesenchymal stem cell perspective: cell biology to clinical progress. npj Regenerative Medicine. 2019;4:22. doi:10.1038/s41536-019-0083-6 ↩
