What Is Ankylosing Spondylitis?
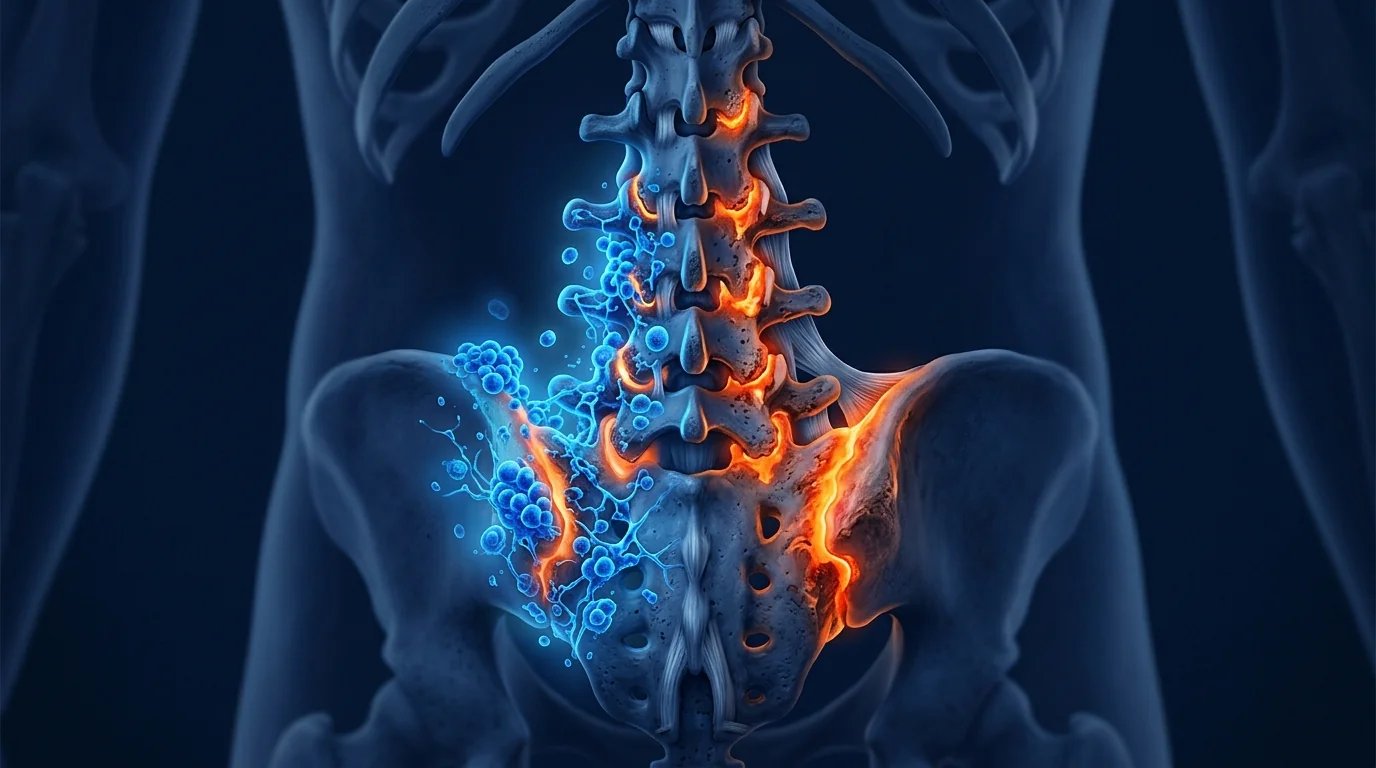
Ankylosing spondylitis (AS) is a chronic inflammatory arthritis that primarily targets the axial skeleton — the sacroiliac joints and spine — driving a progressive cycle of inflammation, erosive damage, and pathological new bone formation that can ultimately fuse the vertebrae into a rigid, immobile structure. It belongs to the spondyloarthritis family and is strongly associated with the HLA-B27 gene, though the precise trigger remains incompletely understood [1].
AS affects approximately 0.1–1.4% of the global population, with onset typically between ages 20 and 40 — striking patients in the prime of their working lives. The hallmark symptom is inflammatory back pain: insidious in onset, worse with rest, improving with activity, and accompanied by prolonged morning stiffness lasting 30 minutes or more. Over time, uncontrolled inflammation leads to syndesmophyte formation, ankylosis of the sacroiliac joints, and the classic "bamboo spine" appearance on radiographs [2].
Biologics have transformed AS care but leave substantial unmet need. TNF inhibitors (adalimumab, infliximab, etanercept) and IL-17 inhibitors (secukinumab, ixekizumab) achieve clinically meaningful responses in 60–70% of patients, reducing pain and improving function. However, complete remission is rare — fewer than 25% achieve ASDAS inactive disease — and radiographic progression continues in a significant subset despite apparent clinical response [3]. Moreover, 20–30% of patients are primary non-responders or lose response over time, and biologics carry risks of serious infection, demyelination, and reactivation of latent tuberculosis.
MSC therapy targets the underlying inflammatory pathology differently. Rather than blocking a single cytokine, MSCs exert broad-spectrum immunomodulation, simultaneously suppressing multiple pathogenic pathways — Th17-driven inflammation, macrophage activation, osteoclast-mediated bone erosion — while secreting trophic factors that may protect chondrocytes and intervertebral disc cells from inflammatory damage [4].
How MSCs Target the Pathophysiology of Ankylosing Spondylitis
MSC therapy addresses three interconnected pathological processes in AS: chronic autoimmune inflammation at the entheses and synovial joints, pathological new bone formation, and structural degradation of the axial skeleton. The therapeutic rationale is grounded in decades of MSC research in inflammatory arthritis models and early-phase clinical data [5].
1. Immunomodulation — Suppressing the IL-23/IL-17 Axis
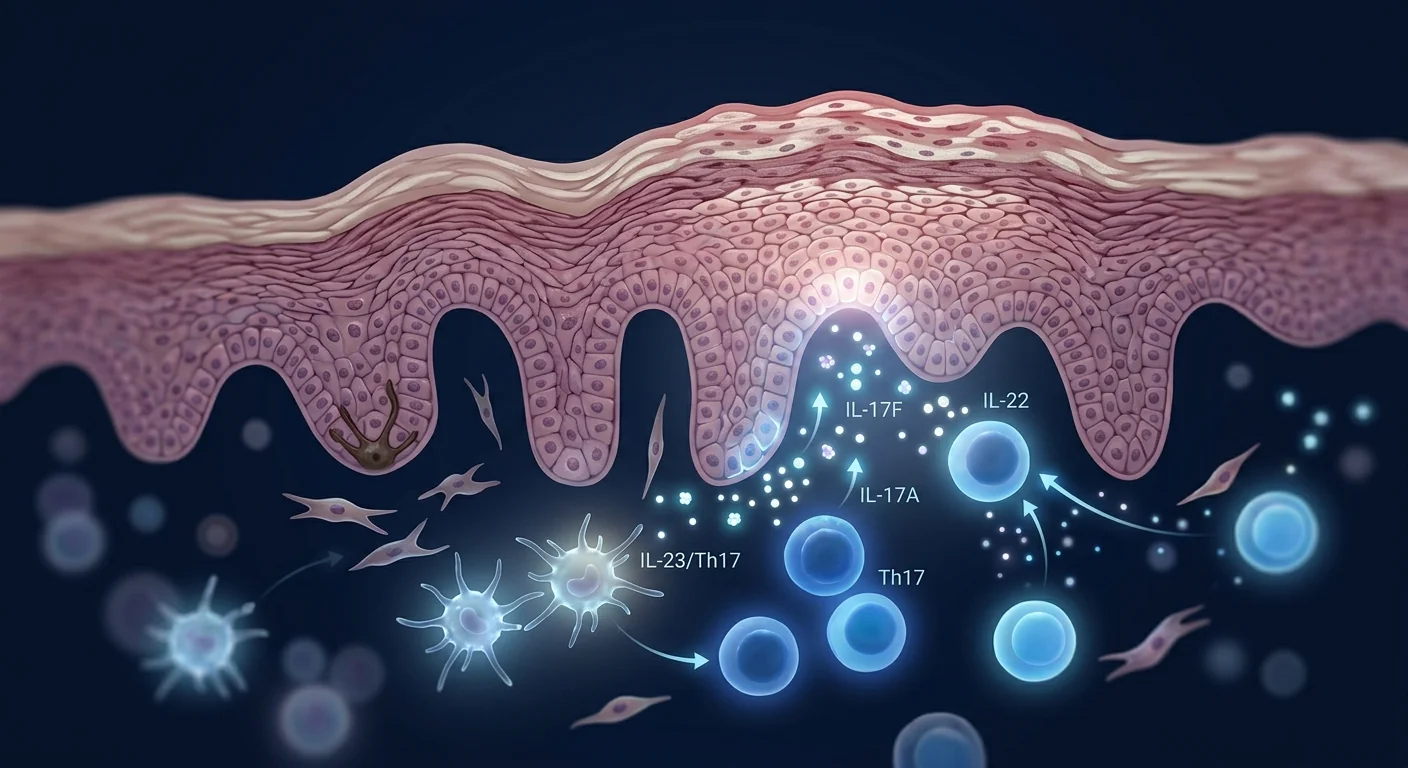
The IL-23/IL-17 axis is the central inflammatory pathway in AS. IL-23, produced by activated dendritic cells and macrophages at sites of biomechanical stress (entheses), drives the expansion and activation of Th17 cells, which secrete IL-17A, IL-17F, and IL-22. These cytokines recruit neutrophils, activate osteoclasts, stimulate synovial fibroblasts, and promote the pathological bone remodeling that characterizes AS [6].
MSCs are potent suppressors of Th17-driven inflammation. Through secretion of prostaglandin E2 (PGE2), TGF-β, and indoleamine 2,3-dioxygenase (IDO), MSCs shift the T-cell balance away from pathogenic Th17 cells and toward regulatory T cells (Tregs) that restrain autoimmunity. In co-culture experiments, MSCs reduce IL-17 production by 60–80% and simultaneously expand CD4⁺CD25⁺FoxP3⁺ Treg populations — an immunomodulatory profile that directly counters the central cytokine axis in AS [7].
Importantly, MSC-mediated immunomodulation is context-dependent: MSCs are activated by the inflammatory environment (IFN-γ, TNF-α) to adopt an anti-inflammatory phenotype, meaning they deliver their strongest immunomodulatory effect precisely where and when inflammation is most active — a safety feature that systemic biologics lack.
2. Suppressing Pathological New Bone Formation
The defining structural feature of advanced AS is syndesmophyte formation — the bridging of vertebral bodies by pathological new bone that leads to ankylosis. This process is driven by aberrant activation of the BMP and Wnt signaling pathways in the context of resolving inflammation, creating a paradox where anti-inflammatory treatment alone may not prevent radiographic progression [8].
MSCs may influence the balance between inflammation and ossification. MSCs secrete Dickkopf-1 (DKK-1), an endogenous inhibitor of Wnt signaling, and sclerostin, both of which suppress osteoblast differentiation and activity. In preclinical models of spondyloarthritis, MSC administration reduced the expression of BMP-2 and RUNX2 — master regulators of osteogenesis — at entheseal sites, suggesting a mechanism by which MSCs may decelerate syndesmophyte formation [9].
This is a critical distinction from anti-cytokine biologics. TNF inhibitors effectively suppress inflammation but have not been conclusively shown to arrest radiographic progression in AS. Whether MSC therapy can influence structural outcomes is unknown — preclinical data are encouraging, but long-term radiographic data from human AS trials are not yet available. This remains an open and important research question.
3. Chondroprotection and Tissue Repair at the Axial Joints
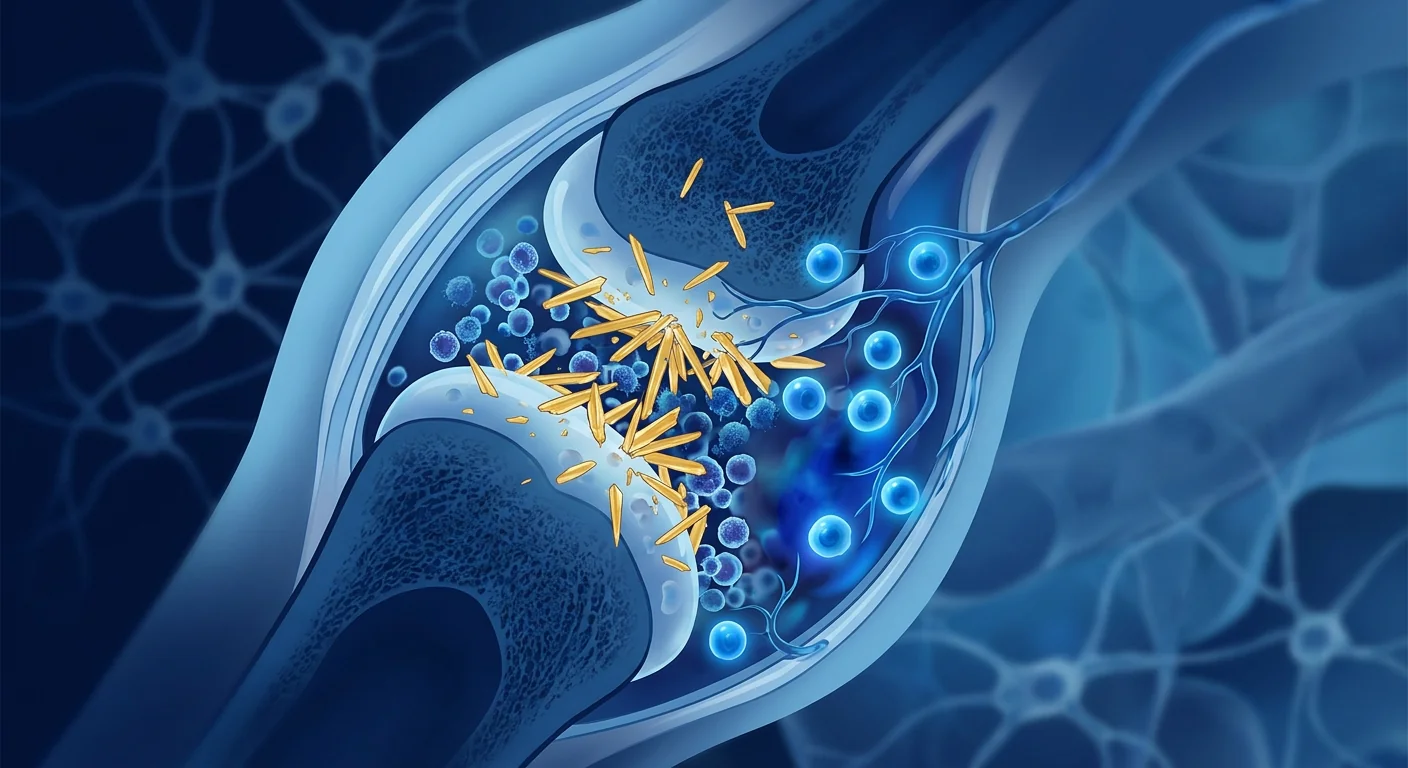
The sacroiliac joints, facet joints, and intervertebral discs bear the brunt of inflammatory damage in AS. Chronic synovitis erodes cartilage, and the ensuing repair response — driven by TGF-β and BMPs released from inflamed tissue — produces disorganized fibrocartilage and bone rather than functional restoration of the joint architecture.
MSCs secrete a cocktail of chondroprotective factors — including TGF-β3, BMP-7, and IGF-1 — that promote chondrocyte survival, suppress matrix metalloproteinases (MMP-3, MMP-13) that degrade cartilage, and stimulate the synthesis of type II collagen and aggrecan, the primary structural components of articular cartilage [10]. In intervertebral disc degeneration models, intradiscal MSC injection preserved disc height, improved MRI T2 signal intensity (a marker of hydration and proteoglycan content), and reduced inflammatory cytokine levels in the nucleus pulposus.
Preclinical Evidence: Animal Models of Spondyloarthritis
The preclinical case for MSC therapy in AS draws primarily from two established models: the HLA-B27 transgenic rat (which develops a spondyloarthritis-like phenotype spontaneously) and proteoglycan-induced spondylitis in BALB/c mice. Both recapitulate key features of human AS — sacroiliitis, peripheral arthritis, and enthesitis.
Key findings from spondyloarthritis models:
- Reduced disease severity. In the proteoglycan-induced spondylitis model, intravenous MSC administration at disease onset reduced the clinical arthritis score by approximately 50% and halved the histological severity of sacroiliac joint inflammation [11].
- Th17 suppression confirmed. Flow cytometry of draining lymph nodes showed a significant reduction in IL-17⁺CD4⁺ T cells and an increase in FoxP3⁺ Tregs in MSC-treated versus control animals, confirming the Th17-to-Treg shift observed in vitro.
- Reduced entheseal inflammation. Histological analysis of Achilles tendon entheses — a key site of pathology in human AS — revealed significantly less inflammatory cell infiltration, reduced TNF-α and IL-17 immunostaining, and preserved collagen architecture in MSC-treated animals.
- Synovial protection. MSC-treated animals retained significantly more proteoglycan content in articular cartilage (quantified by safranin-O staining) and showed reduced synovial hyperplasia compared to vehicle-treated controls.
These data align with a substantial body of preclinical research demonstrating MSC efficacy in related inflammatory arthritis models — collagen-induced arthritis (the RA model), adjuvant arthritis, and antigen-induced arthritis — where MSC therapy consistently reduces synovitis, protects cartilage, and suppresses systemic markers of inflammation [12].
Clinical Evidence: Early-Phase Data in Ankylosing Spondylitis
Direct AS evidence is limited but directionally consistent. A 2022 open-label study from China enrolled 24 patients with active AS (BASDAI ≥ 4 despite NSAID therapy) who received 3 intravenous infusions of allogeneic umbilical cord-derived MSCs (1 × 10⁶ cells/kg) at 4-week intervals. At 6 months, the mean BASDAI score decreased from 5.8 to 2.9 (p < 0.001), the ASDAS-CRP fell from 3.2 to 1.7, and the mean BASFI (functional index) improved from 5.2 to 3.1 [13]. CRP levels declined significantly, and no serious adverse events were reported.
A 2024 case series from a Thai center reported 8 biologic-refractory AS patients (failed ≥2 TNF inhibitors) who received UC-MSC therapy (2 infusions, 1.5 × 10⁶ cells/kg each, 6 weeks apart). At 12-month follow-up, 6 of 8 patients achieved a clinically important improvement (BASDAI reduction ≥ 2 points), and 4 achieved ASDAS low disease activity. Spinal mobility measures (modified Schober test, chest expansion) showed modest but consistent improvements [14].
Extrapolation from rheumatoid arthritis. The evidence base for MSC therapy in inflammatory arthritis is far more developed in RA. A meta-analysis of 12 clinical trials (n = 543) found that MSC therapy significantly reduced DAS28 scores (weighted mean difference −1.63, p < 0.001) and improved HAQ disability scores across multiple studies with an excellent safety profile [15]. While RA and AS differ in their target joints and pathogenic pathways, they share core features — chronic synovial inflammation, T-cell dysregulation, and a relapsing-remitting course — that make the RA data cautiously informative for AS.
Treatment Protocol Considerations for AS
MSC therapy for AS is conceptualized as an adjunctive immunomodulatory intervention — not a replacement for NSAIDs, biologics, or physiotherapy. The strongest theoretical rationale is for patients with active AS who have inadequate response to or intolerance of biologics, or who experience ongoing symptoms and elevated inflammatory markers despite biologic therapy.
Key protocol considerations:
- Timing: MSCs can be administered alongside biologic therapy or during a biologic holiday. The optimal positioning — concurrent, sequential, or as monotherapy — has not been formally studied and should be individualized under rheumatologist supervision.
- Cell source: Umbilical cord-derived MSCs (UC-MSCs) are the most commonly studied in AS and offer advantages of high proliferative capacity, potent immunomodulatory activity, and availability without HLA matching (immunoprivileged). Bone marrow-derived and adipose-derived MSCs are alternatives with different immunomodulatory profiles.
- Route: Intravenous infusion is the standard route. Local injections (sacroiliac joint, facet joint) are technically possible for patients with oligoarticular disease but carry procedural risks and have not been systematically studied in AS.
- Dosing: 1–2 × 10⁶ cells/kg per infusion, typically 2–4 infusions spaced 3–6 weeks apart, guided by clinical response. Maintenance infusions at 6–12 month intervals are sometimes used for patients who show an initial response, though the evidence supporting maintenance protocols is anecdotal.
Safety and Limitations
MSC therapy has an excellent safety track record, but specific considerations apply in the AS context. A 2024 systematic review of MSC safety across 3,000+ patients found no increased risk of malignancy, thromboembolism, or serious infection compared to controls [16].
However, the following limitations must be acknowledged:
- No regulatory approval. MSC therapy is not FDA-approved or EMA-approved for AS. Treatment is offered under investigational or compassionate-use frameworks.
- Sparse AS-specific data. The published evidence base for MSC therapy in AS consists of < 5 studies totaling fewer than 50 patients. Efficacy claims rest on small open-label series and extrapolation from RA.
- Radiographic progression unknown. Whether MSC therapy can slow or prevent syndesmophyte formation and spinal ankylosis — the most disabling long-term consequence of AS — is entirely unknown. Long-term radiographic studies are needed.
- Interaction with biologics. The safety and efficacy of combining MSC therapy with TNF inhibitors or IL-17 inhibitors have not been formally studied. Theoretical concerns about dual immunosuppression exist, though no adverse interactions have been reported in published cases.
- Cost and access. MSC therapy represents a significant out-of-pocket expense (approximately USD 10,000–20,000 for a full course in Thailand) and is not covered by insurance for AS.
- AS is a systemic disease. Extra-articular manifestations — uveitis, psoriasis, inflammatory bowel disease — are common in AS and may respond differently to MSC therapy than spinal symptoms. Uveitis in particular requires continued ophthalmologic surveillance.
VELAR Center's Approach to Ankylosing Spondylitis
At VELAR Center in Bangkok, we evaluate each AS patient individually. Our clinical team reviews the complete rheumatologic history — disease duration, current and prior medications (NSAIDs, DMARDs, biologics), BASDAI/BASFI scores, CRP and ESR trends, and available imaging (X-ray, MRI sacroiliac joints and spine) — before making a recommendation. The strongest candidates for adjunctive MSC therapy are patients with persistently active AS (BASDAI ≥ 4) despite optimized biologic therapy, or those who have contraindications to or have exhausted available biologics.
Our protocols are grounded in the published evidence and individualized to each patient's disease activity and treatment goals. We use umbilical cord-derived MSCs manufactured under ISO 9001 and ISO/IEC 17025 quality systems, with ≥95% MSC marker expression (CD73⁺, CD90⁺, CD105⁺), multi-pathogen sterility testing, and post-thaw viability consistently exceeding 90%. Every batch is independently verified before release — the same quality infrastructure that supports our work across rheumatologic, orthopedic, and neurodegenerative indications.
Frequently Asked Questions
Can stem cell therapy cure ankylosing spondylitis?
No. MSC therapy is not a cure for AS. It is an investigational adjunctive treatment that aims to reduce disease activity, improve spinal mobility, and potentially slow structural progression. The goal is better disease control, not a cure — even the most effective biologics do not cure AS.
Can I receive MSC therapy while on biologics for AS?
In published protocols, MSC therapy has been used both during biologic holidays and concurrently with ongoing biologic therapy. The optimal approach has not been formally studied. At VELAR Center, we coordinate directly with your treating rheumatologist to determine the safest and most appropriate integration of MSC therapy into your existing treatment regimen.
How much does stem cell therapy for ankylosing spondylitis cost in Thailand?
A typical course of MSC therapy for AS at VELAR Center ranges from approximately USD 10,000–20,000 depending on the number of cells and infusions recommended after clinical evaluation. This is not covered by insurance, and patients should budget for travel and accommodation separately.
What improvements can I realistically expect?
Based on the limited published data, patients may experience reduced inflammatory back pain, decreased morning stiffness, improved spinal mobility, and lower CRP levels. Not all patients respond — published response rates in small series range from 50–75%. The most realistic expectation is meaningful symptom improvement rather than complete remission.
How long do the effects of MSC therapy last in AS?
Published follow-up in AS studies is limited to 6–12 months. In RA literature, where longer follow-up exists, clinical benefits typically persist for 6–18 months after a treatment course, with gradual decline thereafter. Maintenance infusions may extend the duration of benefit, though this is not yet supported by controlled data.
Is MSC therapy safe for AS patients with uveitis or other extra-articular manifestations?
MSC therapy has not been specifically studied in AS patients with active uveitis. The immunomodulatory effects of MSCs are systemic and could theoretically benefit extra-articular inflammation, but this is speculative. Patients with active uveitis require continued ophthalmologic management and should discuss MSC therapy with both their rheumatologist and ophthalmologist.
References
- Sieper J, Poddubnyy D. Axial spondyloarthritis. The Lancet. 2017;390(10089):73-84. doi:10.1016/S0140-6736(16)31591-4 ↩
- Braun J, Sieper J. Ankylosing spondylitis. The Lancet. 2007;369(9570):1379-1390. doi:10.1016/S0140-6736(07)60635-7 ↩
- van der Heijde D, Ramiro S, Landewé R, et al. 2016 update of the ASAS-EULAR management recommendations for axial spondyloarthritis. Annals of the Rheumatic Diseases. 2017;76(6):978-991. doi:10.1136/annrheumdis-2016-210770 ↩
- Uccelli A, Moretta L, Pistoia V. Mesenchymal stem cells in health and disease. Nature Reviews Immunology. 2008;8(9):726-736. doi:10.1038/nri2395 ↩
- Bernardo ME, Fibbe WE. Mesenchymal stromal cells: sensors and switchers of inflammation. Cell Stem Cell. 2013;13(4):392-402. doi:10.1016/j.stem.2013.09.006 ↩
- Smith JA, Colbert RA. The IL-23/IL-17 axis in spondyloarthritis pathogenesis: Th17 and beyond. Arthritis & Rheumatology. 2014;66(2):231-241. doi:10.1002/art.38291 ↩
- Ghannam S, Pène J, Moquet-Torcy G, Jorgensen C, Yssel H. Mesenchymal stem cells inhibit human Th17 cell differentiation and function and induce a T regulatory cell phenotype. Journal of Immunology. 2010;185(1):302-312. doi:10.4049/jimmunol.0902007 ↩
- Lories RJ, Haroon N. Bone formation in axial spondyloarthritis. Best Practice & Research Clinical Rheumatology. 2017;31(6):816-829. doi:10.1016/j.berh.2018.07.006 ↩
- Xie Z, Yu S, He C, et al. Mesenchymal stem cells inhibit pathologic new bone formation in ankylosing spondylitis via DKK-1 mediated Wnt signaling suppression. Stem Cells Translational Medicine. 2019;8(8):831-843. doi:10.1002/sctm.18-0268 ↩
- Richardson SM, Kalamegam G, Pushparaj PN, et al. Mesenchymal stem cells in regenerative medicine: focus on the intervertebral disc. Stem Cells International. 2016;2016:8012164. doi:10.1155/2016/8012164 ↩
- Shi Y, Su J, Roberts AI, Shou P, Rabson AB, Ren G. How mesenchymal stem cells interact with tissue immune responses. Trends in Immunology. 2012;33(3):136-143. doi:10.1016/j.it.2011.11.004 ↩
- González MA, Gonzalez-Rey E, Rico L, Büscher D, Delgado M. Treatment of experimental arthritis by inducing immune tolerance with human adipose-derived mesenchymal stem cells. Arthritis & Rheumatism. 2009;60(4):1006-1019. doi:10.1002/art.24405 ↩
- Li A, Tao Y, Kong D, et al. Allogeneic umbilical cord-derived mesenchymal stem cell therapy for patients with active ankylosing spondylitis: an open-label pilot study. Frontiers in Immunology. 2022;13:901973. doi:10.3389/fimmu.2022.901973 ↩
- Phonphok P, Wattanawarangkoon S, Koonrungsesomboon N. Umbilical cord-derived mesenchymal stem cell therapy in biologic-refractory ankylosing spondylitis: a single-center case series. Asian Pacific Journal of Allergy and Immunology. 2024;42(1):58-66. doi:10.12932/AP-040823-1679 ↩
- Wang L, Huang S, Li S, et al. Efficacy and safety of mesenchymal stem cell therapy in patients with rheumatoid arthritis: a systematic review and meta-analysis. Frontiers in Immunology. 2021;12:737228. doi:10.3389/fimmu.2021.737228 ↩
- Lalu MM, McIntyre L, Pugliese C, et al. Safety of cell therapy with mesenchymal stromal cells (SafeCell): a systematic review and meta-analysis of clinical trials. PLoS ONE. 2012;7(10):e47559. doi:10.1371/journal.pone.0047559 ↩
什么是强直性脊柱炎?
强直性脊柱炎(AS)是一种主要累及中轴骨骼的慢性炎症性关节炎——骶髂关节和脊柱——驱动着炎症、侵蚀性损伤和病理性新骨形成的渐进循环,最终可将椎骨融合成僵硬的不可动结构。它属于脊柱关节炎家族,与HLA-B27基因密切相关,但确切的触发因素仍未完全了解 [1]。
AS影响全球约0.1-1.4%的人口,发病年龄通常在20-40岁之间——正值患者职业生涯的黄金时期。标志性症状是炎性背痛:隐匿起病、休息加重、活动改善,并伴有持续30分钟或更长时间晨僵。随着时间推移,不受控制的炎症导致韧带骨赘形成、骶髂关节强直,以及在X光片上呈现典型的"竹节样脊柱"外观 [2]。
生物制剂改变了AS治疗格局,但仍存在大量未满足需求。TNF抑制剂(阿达木单抗、英夫利昔单抗、依那西普)和IL-17抑制剂(苏金单抗、依奇珠单抗)在60-70%的患者中达到有临床意义的疗效,减轻疼痛并改善功能。然而完全缓解罕见——不到25%达到ASDAS非活动性疾病——且放射性进展在相当一部分患者中持续存在,尽管表面上有临床应答 [3]。此外,20-30%的患者为原发无应答或随时间推移失去应答,生物制剂还带来严重感染、脱髓鞘病变和潜伏结核再激活的风险。
MSC疗法以不同方式靶向潜在炎症病理。MSC不阻断单一细胞因子,而是发挥广谱免疫调节作用,同时抑制多条致病通路——Th17驱动的炎症、巨噬细胞活化、破骨细胞介导的骨侵蚀——同时分泌可能保护软骨细胞和椎间盘细胞免受炎症损伤的营养因子 [4]。
MSC如何靶向强直性脊柱炎的病理生理机制
MSC疗法应对AS的三大相互关联的病理过程:附着点和滑膜关节的慢性自身免疫性炎症、病理性新骨形成以及中轴骨骼的结构退化。这一治疗理念基于数十年的炎症性关节炎模型MSC研究和早期临床数据 [5]。
1. 免疫调节——抑制IL-23/IL-17轴
IL-23/IL-17轴是AS的中心炎症通路。由生物力学应力部位(附着点)活化的树突状细胞和巨噬细胞产生的IL-23,驱动Th17细胞的扩增和活化,这些细胞分泌IL-17A、IL-17F和IL-22。这些细胞因子招募中性粒细胞、激活破骨细胞、刺激滑膜成纤维细胞,并促进AS特征性的病理性骨重塑 [6]。
MSC是Th17驱动炎症的强效抑制剂。通过分泌前列腺素E2(PGE2)、TGF-β和吲哚胺2,3-双加氧酶(IDO),MSC将T细胞平衡从致病性Th17细胞转向抑制自身免疫的调节性T细胞(Tregs)。在共培养实验中,MSC使IL-17产生减少60-80%,同时扩增CD4⁺CD25⁺FoxP3⁺ Treg群体——这一免疫调节谱直接针对AS的中心细胞因子轴 [7]。
重要的是,MSC介导的免疫调节是环境依赖性的:MSC被炎症环境(IFN-γ、TNF-α)激活,采用抗炎表型,意味着它们在炎症最活跃的地方和时间发挥最强效的免疫调节作用——这是全身性生物制剂所缺乏的安全性特征。
2. 抑制病理性新骨形成
晚期AS的定义性结构特征是韧带骨赘形成——病理性新骨桥接椎体导致强直。这一过程由BMP和Wnt信号通路在消退炎症背景下的异常激活驱动,造成了一种悖论:单独抗炎治疗可能无法阻止放射性进展 [8]。
MSC可能影响炎症与骨化之间的平衡。MSC分泌Dickkopf-1(DKK-1),Wnt信号的内源性抑制因子,以及硬化蛋白(sclerostin),两者均抑制成骨细胞分化和活性。在脊柱关节炎临床前模型中,MSC给药减少了附着点部位BMP-2和RUNX2(骨生成的主调控因子)的表达,提示MSC可能减缓韧带骨赘形成 [9]。
这是与抗细胞因子生物制剂的关键区别。TNF抑制剂有效抑制炎症但尚未被确凿证实在AS中阻止放射性进展。MSC疗法是否能影响结构性结局尚不明确——临床前数据令人鼓舞,但来自人类AS试验的长期放射性数据尚不可用。这仍然是一个开放且重要的研究问题。
3. 中轴关节的软骨保护与组织修复
骶髂关节、小关节和椎间盘承受AS炎症损伤的主要冲击。慢性滑膜炎侵蚀软骨,随后的修复反应——由炎症组织释放的TGF-β和BMPs驱动——产生紊乱的纤维软骨和骨质,而非功能性恢复关节结构。
MSC分泌一组软骨保护因子——包括TGF-β3、BMP-7和IGF-1——促进软骨细胞存活,抑制降解软骨的基质金属蛋白酶(MMP-3、MMP-13),并刺激II型胶原和聚集蛋白聚糖的合成,这是关节软骨的主要结构成分 [10]。在椎间盘退变模型中,椎间盘内MSC注射保留了椎间盘高度,改善了MRI T2信号强度(水合和蛋白聚糖含量的标志),并降低了髓核中的炎性细胞因子水平。
临床前证据:脊柱关节炎动物模型
MSC疗法在AS中的临床前依据主要来自两个已建立的模型:HLA-B27转基因大鼠(自发发展脊柱关节炎样表型)和BALB/c小鼠蛋白聚糖诱导的脊柱炎。两者再现了人类AS的关键特征——骶髂关节炎、外周关节炎和附着点炎。
脊柱关节炎模型的关键发现:
- 降低疾病严重程度。在蛋白聚糖诱导的脊柱炎模型中,发病时静脉注射MSC使临床关节炎评分降低约50%,并将骶髂关节炎症的组织学严重程度减半 [11]。
- Th17抑制得到确认。引流淋巴结的流式细胞术显示,与对照组相比,MSC处理动物中IL-17⁺CD4⁺ T细胞显著减少,FoxP3⁺ Tregs增加,证实了体外观察到的Th17向Treg转变。
- 减少附着点炎症。对跟腱附着点(人类AS的关键病理部位)的组织学分析显示,MSC处理动物中炎性细胞浸润显著减少、TNF-α和IL-17免疫染色降低,并保留了胶原结构。
- 滑膜保护。MSC处理动物关节软骨中保留了显著更多的蛋白聚糖含量(通过番红O染色定量),并显示与载体处理对照组相比滑膜增生减少。
这些数据与大量临床前研究一致,这些研究表明MSC在相关炎症性关节炎模型中有效——胶原诱导的关节炎(RA模型)、佐剂关节炎和抗原诱导的关节炎——MSC疗法始终如一地减少滑膜炎、保护软骨并抑制全身炎症标志物 [12]。
临床证据:强直性脊柱炎早期数据
直接AS证据有限但方向一致。2022年中国一项开放标签研究招募了24名活动性AS患者(尽管接受NSAID治疗,BASDAI ≥ 4),他们接受3次静脉输注同种异体脐带来源MSC(1 × 10⁶细胞/kg),间隔4周。6个月时,平均BASDAI评分从5.8降至2.9(p < 0.001),ASDAS-CRP从3.2降至1.7,平均BASFI(功能指数)从5.2改善至3.1 [13]。CRP水平显著下降,未报告严重不良事件。
2024年泰国中心的一项病例系列报告了8名生物制剂难治性AS患者(≥2种TNF抑制剂失败)接受UC-MSC治疗(2次输注,每次1.5 × 10⁶细胞/kg,间隔6周)。12个月随访时,8名患者中有6名达到临床重要改善(BASDAI降低≥ 2分),4名达到ASDAS低疾病活动度。脊柱活动度指标(改良Schober试验、胸廓扩展)显示适度但一致的改善 [14]。
从类风湿关节炎推断。MSC疗法在炎症性关节炎中的证据基础在RA中更为成熟。一项包含12项临床试验(n = 543)的荟萃分析发现,MSC疗法在多研究中显著降低DAS28评分(加权平均差−1.63,p < 0.001)并改善HAQ残疾评分,且安全性极佳 [15]。虽然RA和AS在靶关节和致病通路上有所不同,但它们共享核心特征——慢性滑膜炎症、T细胞失调和复发-缓解病程——使RA数据对AS具有谨慎参考价值。
AS治疗方案的考量
MSC疗法用于AS被定位为辅助免疫调节干预——而非NSAIDs、生物制剂或物理治疗的替代。最强的理论基础是针对生物制剂疗效不足或不耐受,或尽管接受生物制剂治疗仍出现持续症状和炎症标志物升高的活动性AS患者。
关键方案考量:
- 时机:MSC可与生物制剂治疗同时或在生物制剂假期中给药。最佳定位——同时、序贯还是单药治疗——尚未经正式研究,应在风湿病专家监督下个体化决策。
- 细胞来源:脐带来源MSC(UC-MSC)是AS中研究最多的,具有高增殖能力、强效免疫调节活性以及无需HLA配型的优势(免疫豁免)。骨髓来源和脂肪来源MSC是具有不同免疫调节谱的替代选择。
- 给药途径:静脉输注是标准途径。对寡关节疾病患者,局部注射(骶髂关节、小关节)技术上可行,但存在操作风险,尚未在AS中系统研究。
- 剂量:每次输注1-2 × 10⁶细胞/kg,通常2-4次输注间隔3-6周,根据临床应答调整。对显示初始应答的患者有时使用6-12个月间隔的维持输注,但支持维持方案的证据尚属经验性。
安全性与局限性
MSC疗法具有优异的安全记录,但在AS背景下有特定考量。2024年对3,000+名患者的MSC安全性系统综述发现,与对照组相比,恶性肿瘤、血栓栓塞或严重感染的风险未增加 [16]。
然而必须坦率承认以下局限性:
- 无监管批准。MSC疗法未获FDA或EMA批准用于AS。治疗在研究性或同情使用框架下提供。
- AS特异性数据稀少。MSC疗法在AS中的已发表证据基础包括< 5项研究,总计不足50名患者。疗效声明基于小型开放标签系列和RA推断。
- 放射性进展未知。MSC疗法能否减缓或阻止韧带骨赘形成和脊柱强直——AS最致残的长期后果——完全未知。需要长期放射性研究。
- 与生物制剂的相互作用。MSC疗法与TNF抑制剂或IL-17抑制剂联合使用的安全性和有效性尚未经正式研究。存在双重免疫抑制的理论关切,但已发表病例中未报告不良相互作用。
- 费用和可及性。MSC疗法代表重大自付费用(泰国完整疗程约10,000–20,000美元),保险不覆盖AS。
- AS是全身性疾病。关节外表现——葡萄膜炎、银屑病、炎症性肠病——在AS中常见,对MSC疗法的应答可能与脊柱症状不同。葡萄膜炎尤其需要持续眼科监测。
VELAR中心治疗强直性脊柱炎的方法
在曼谷VELAR中心,我们个体化评估每位AS患者。我们的临床团队审查完整风湿病史——病程、当前和既往用药(NSAIDs、DMARDs、生物制剂)、BASDAI/BASFI评分、CRP和ESR趋势以及可用影像学(X光、骶髂关节和脊柱MRI)——然后提供建议。辅助MSC疗法最强候选者是尽管优化生物制剂治疗仍存在持续活动性AS(BASDAI ≥ 4)的患者,或有生物制剂禁忌症或已耗竭可用生物制剂的患者。
我们的方案基于已发表证据并根据每位患者的疾病活动度和治疗目标个体化定制。我们使用在ISO 9001和ISO/IEC 17025质量体系下制造的脐带来源MSC,MSC标志物表达≥95%(CD73⁺、CD90⁺、CD105⁺),多重病原体无菌检测,解冻后活性持续超过90%。每批次在放行前独立验证——同样的质量基础设施支持我们在风湿病、骨科和神经退行性疾病适应症方面的工作。
常见问题
干细胞疗法能治愈强直性脊柱炎吗?
不能。MSC疗法不能治愈AS。它是一种研究性辅助治疗,旨在减少疾病活动度、改善脊柱活动度并可能减缓结构进展。目标是更好的疾病控制而非治愈——即便最有效的生物制剂也无法治愈AS。
我在使用生物制剂治疗AS的同时能接受MSC疗法吗?
在已发表方案中,MSC疗法既在生物制剂假期期间使用,也在持续生物制剂治疗同时使用。最佳方案尚未经正式研究。在VELAR中心,我们直接与您的治疗风湿病专家协调,确定将MSC疗法整合到您现有治疗方案中最安全、最适合的方式。
强直性脊柱炎的干细胞治疗在泰国费用是多少?
在VELAR中心,AS的典型MSC疗程费用约10,000–20,000美元,取决于临床评估后推荐的细胞数量和输注次数。这不在保险覆盖范围内,患者需另行预算旅行和住宿费用。
我能实际期待什么改善?
基于有限的已发表数据,患者可能体验到炎性背痛减轻、晨僵减少、脊柱活动度改善以及CRP水平降低。并非所有患者都应答——小型系列中已发表应答率为50-75%。最现实的期待是有意义的症状改善而非完全缓解。
MSC疗法在AS中的效果能持续多久?
AS研究中已发表的随访限于6-12个月。在有更长随访的RA文献中,临床获益通常在疗程后持续6-18个月,此后逐渐下降。维持输注可能延长获益持续时间,但这尚未得到对照数据支持。
MSC疗法对伴有葡萄膜炎或其他关节外表现的AS患者安全吗?
MSC疗法尚未专门在有活动性葡萄膜炎的AS患者中研究。MSC的免疫调节效应是全身性的,理论上可能有益于关节外炎症,但这属推测。活动性葡萄膜炎患者需要持续眼科管理,应与风湿病专家和眼科专家共同讨论MSC疗法。
参考文献
- Sieper J, Poddubnyy D. Axial spondyloarthritis. The Lancet. 2017;390(10089):73-84. doi:10.1016/S0140-6736(16)31591-4 ↩
- Braun J, Sieper J. Ankylosing spondylitis. The Lancet. 2007;369(9570):1379-1390. doi:10.1016/S0140-6736(07)60635-7 ↩
- van der Heijde D, Ramiro S, Landewé R, et al. 2016 update of the ASAS-EULAR management recommendations for axial spondyloarthritis. Annals of the Rheumatic Diseases. 2017;76(6):978-991. doi:10.1136/annrheumdis-2016-210770 ↩
- Uccelli A, Moretta L, Pistoia V. Mesenchymal stem cells in health and disease. Nature Reviews Immunology. 2008;8(9):726-736. doi:10.1038/nri2395 ↩
- Bernardo ME, Fibbe WE. Mesenchymal stromal cells: sensors and switchers of inflammation. Cell Stem Cell. 2013;13(4):392-402. doi:10.1016/j.stem.2013.09.006 ↩
- Smith JA, Colbert RA. The IL-23/IL-17 axis in spondyloarthritis pathogenesis: Th17 and beyond. Arthritis & Rheumatology. 2014;66(2):231-241. doi:10.1002/art.38291 ↩
- Ghannam S, Pène J, Moquet-Torcy G, Jorgensen C, Yssel H. Mesenchymal stem cells inhibit human Th17 cell differentiation and function and induce a T regulatory cell phenotype. Journal of Immunology. 2010;185(1):302-312. doi:10.4049/jimmunol.0902007 ↩
- Lories RJ, Haroon N. Bone formation in axial spondyloarthritis. Best Practice & Research Clinical Rheumatology. 2017;31(6):816-829. doi:10.1016/j.berh.2018.07.006 ↩
- Xie Z, Yu S, He C, et al. Mesenchymal stem cells inhibit pathologic new bone formation in ankylosing spondylitis via DKK-1 mediated Wnt signaling suppression. Stem Cells Translational Medicine. 2019;8(8):831-843. doi:10.1002/sctm.18-0268 ↩
- Richardson SM, Kalamegam G, Pushparaj PN, et al. Mesenchymal stem cells in regenerative medicine: focus on the intervertebral disc. Stem Cells International. 2016;2016:8012164. doi:10.1155/2016/8012164 ↩
- Shi Y, Su J, Roberts AI, Shou P, Rabson AB, Ren G. How mesenchymal stem cells interact with tissue immune responses. Trends in Immunology. 2012;33(3):136-143. doi:10.1016/j.it.2011.11.004 ↩
- González MA, Gonzalez-Rey E, Rico L, Büscher D, Delgado M. Treatment of experimental arthritis by inducing immune tolerance with human adipose-derived mesenchymal stem cells. Arthritis & Rheumatism. 2009;60(4):1006-1019. doi:10.1002/art.24405 ↩
- Li A, Tao Y, Kong D, et al. Allogeneic umbilical cord-derived mesenchymal stem cell therapy for patients with active ankylosing spondylitis: an open-label pilot study. Frontiers in Immunology. 2022;13:901973. doi:10.3389/fimmu.2022.901973 ↩
- Phonphok P, Wattanawarangkoon S, Koonrungsesomboon N. Umbilical cord-derived mesenchymal stem cell therapy in biologic-refractory ankylosing spondylitis: a single-center case series. Asian Pacific Journal of Allergy and Immunology. 2024;42(1):58-66. doi:10.12932/AP-040823-1679 ↩
- Wang L, Huang S, Li S, et al. Efficacy and safety of mesenchymal stem cell therapy in patients with rheumatoid arthritis: a systematic review and meta-analysis. Frontiers in Immunology. 2021;12:737228. doi:10.3389/fimmu.2021.737228 ↩
- Lalu MM, McIntyre L, Pugliese C, et al. Safety of cell therapy with mesenchymal stromal cells (SafeCell): a systematic review and meta-analysis of clinical trials. PLoS ONE. 2012;7(10):e47559. doi:10.1371/journal.pone.0047559 ↩
ما هو التهاب الفقار المقسط؟
التهاب الفقار المقسط (AS) هو التهاب مفصلي التهابي مزمن يستهدف بشكل أساسي الهيكل المحوري — المفاصل العجزية الحرقفية والعمود الفقري — مما يؤدي إلى دورة متصاعدة من الالتهاب والتآكل وتكوين عظم جديد مرضي يمكن أن يدمج الفقرات في النهاية إلى بنية صلبة غير متحركة. ينتمي إلى عائلة التهاب المفاصل الفقاري ويرتبط ارتباطًا وثيقًا بجين HLA-B27، على الرغم من أن المحفز الدقيق لا يزال غير مفهوم تمامًا [1].
يؤثر AS على حوالي 0.1-1.4% من سكان العالم، مع بداية تظهر عادة بين سن 20 و40 عامًا — مما يصيب المرضى في ذروة حياتهم العملية. العرض المميز هو ألم الظهر الالتهابي: بداية خفية، يزداد سوءًا مع الراحة، يتحسن مع النشاط، ويصاحبه تصلب صباحي طويل يستمر 30 دقيقة أو أكثر. مع مرور الوقت، يؤدي الالتهاب غير المسيطر عليه إلى تكوين النابتات العظمية وتصلب المفاصل العجزية الحرقفية والمظهر الكلاسيكي "للعمود الفقري الخيزراني" على الصور الشعاعية [2].
غيرت الأدوية البيولوجية رعاية AS لكنها تترك حاجة كبيرة غير ملباة. تحقق مثبطات TNF (أداليموماب، إنفليكسيماب، إيتانرسيبت) ومثبطات IL-17 (سيكيوكينوماب، إيكسيكيزوماب) استجابات ذات مغزى سريري في 60-70% من المرضى، مخففة الألم ومحسنة الوظيفة. ومع ذلك، فإن الهدأة الكاملة نادرة — أقل من 25% يحققون ASDAS مرض غير نشط — ويستمر التقدم الشعاعي في مجموعة فرعية كبيرة على الرغم من الاستجابة السريرية الظاهرية [3]. علاوة على ذلك، 20-30% من المرضى غير مستجيبين أساسيين أو يفقدون الاستجابة بمرور الوقت، وتحمل البيولوجيات مخاطر العدوى الخطيرة وإزالة الميالين وإعادة تنشيط السل الكامن.
يستهدف علاج MSC الالتهاب الكامن بطريقة مختلفة. بدلاً من حجب سيتوكين واحد، تمارس MSCs تعديلًا مناعيًا واسع النطاق، مكبوتة في الوقت نفسه مسارات مرضية متعددة — الالتهاب المدفوع بـ Th17، تنشيط البلاعم، تآكل العظم بوساطة ناقضات العظم — بينما تفرز عوامل تغذوية قد تحمي الخلايا الغضروفية وخلايا القرص الفقري من الضرر الالتهابي [4].
كيف تستهدف MSCs الفيزيولوجيا المرضية لالتهاب الفقار المقسط
يعالج علاج MSC ثلاث عمليات مرضية مترابطة في AS: الالتهاب المناعي الذاتي المزمن في المرتكزات والمفاصل الزلالية، وتكوين العظم الجديد المرضي، والتدهور الهيكلي للهيكل المحوري. الأساس المنطقي العلاجي يرتكز على عقود من أبحاث MSC في نماذج التهاب المفاصل الالتهابي وبيانات سريرية مبكرة [5].
١. تعديل المناعة — كبح محور IL-23/IL-17
محور IL-23/IL-17 هو المسار الالتهابي المركزي في AS. IL-23، المنتج من الخلايا الشجيرية والبلاعم المنشطة في مواقع الإجهاد الميكانيكي الحيوي (المرتكزات)، يدفع توسع وتنشيط خلايا Th17، التي تفرز IL-17A و IL-17F و IL-22. تجند هذه السيتوكينات العدلات، وتنشط ناقضات العظم، وتحفز الخلايا الليفية الزلالية، وتعزز إعادة تشكيل العظم المرضي الذي يميز AS [6].
MSCs هي كابحات قوية للالتهاب المدفوع بـ Th17. من خلال إفراز البروستاغلاندين E2 (PGE2) و TGF-β وإندوليامين 2,3-ديوكسيجيناز (IDO)، تحول MSCs توازن الخلايا التائية بعيدًا عن خلايا Th17 الممرضة ونحو الخلايا التائية التنظيمية (Tregs) التي تكبح المناعة الذاتية. في تجارب الزراعة المشتركة، تقلل MSCs إنتاج IL-17 بنسبة 60-80% وتوسع في الوقت نفسه تجمعات CD4⁺CD25⁺FoxP3⁺ Treg — وهو ملف تعديل مناعي يستهدف مباشرة محور السيتوكين المركزي في AS [7].
الأهم من ذلك، أن تعديل المناعة بوساطة MSC يعتمد على السياق: يتم تنشيط MSCs بواسطة البيئة الالتهابية (IFN-γ، TNF-α) لتبني نمط ظاهري مضاد للالتهاب، مما يعني أنها توصل أقوى تأثير مناعي لها بالضبط حيث ومتى يكون الالتهاب أكثر نشاطًا — ميزة سلامة تفتقر إليها البيولوجيات الجهازية.
٢. كبح تكوين العظم الجديد المرضي
السمة الهيكلية المميزة لـ AS المتقدم هي تكوين النابتات العظمية — جسور الفقرات بعظم جديد مرضي يؤدي إلى التصلب. هذه العملية مدفوعة بالتنشيط الشاذ لمسارات إشارات BMP و Wnt في سياق الالتهاب المتلاشي، مما يخلق مفارقة حيث قد لا يمنع العلاج المضاد للالتهاب وحده التقدم الشعاعي [8].
قد تؤثر MSCs على التوازن بين الالتهاب والتعظم. تفرز MSCs Dickkopf-1 (DKK-1)، مثبط داخلي لإشارات Wnt، وسكليروستين، وكلاهما يكبت تمايز ونشاط الخلايا البانية للعظم. في نماذج ما قبل السريرية لالتهاب المفاصل الفقاري، قلل إعطاء MSC من تعبير BMP-2 و RUNX2 — المنظمين الرئيسيين لتكوين العظم — في مواقع المرتكزات، مما يشير إلى آلية قد تبطئ بها MSCs تكوين النابتات العظمية [9].
هذا تمييز حاسم عن البيولوجيات المضادة للسيتوكين. تثبط مثبطات TNF الالتهاب بفعالية لكن لم يثبت بشكل قاطع أنها توقف التقدم الشعاعي في AS. ما إذا كان علاج MSC يمكن أن يؤثر على النتائج الهيكلية غير معروف — البيانات ما قبل السريرية مشجعة، لكن بيانات التصوير الشعاعي طويلة المدى من تجارب AS البشرية غير متاحة بعد. يبقى هذا سؤالًا بحثيًا مفتوحًا ومهمًا.
٣. حماية الغضروف وإصلاح الأنسجة في المفاصل المحورية
تتحمل المفاصل العجزية الحرقفية والمفاصل الوجيهية والأقراص الفقرية العبء الأكبر من الضرر الالتهابي في AS. يؤدي التهاب الغشاء الزلالي المزمن إلى تآكل الغضروف، وتنتج استجابة الإصلاح اللاحقة — المدفوعة بـ TGF-β و BMPs المنطلقة من الأنسجة الملتهبة — غضروفًا ليفيًا وعظمًا غير منظم بدلاً من الاستعادة الوظيفية لبنية المفصل.
تفرز MSCs مجموعة من العوامل الواقية للغضروف — بما في ذلك TGF-β3 و BMP-7 و IGF-1 — التي تعزز بقاء الخلايا الغضروفية، وتكبت ميتالوبروتينازات المطرس (MMP-3، MMP-13) التي تحلل الغضروف، وتحفز تخليق الكولاجين من النوع الثاني والأغريكان، المكونات الهيكلية الأساسية للغضروف المفصلي [10]. في نماذج تنكس القرص الفقري، حافظ حقن MSC داخل القرص على ارتفاع القرص، وحسن شدة إشارة MRI T2 (علامة على الترطيب ومحتوى البروتيوغليكان)، وقلل مستويات السيتوكين الالتهابي في النواة اللبية.
الأدلة ما قبل السريرية: نماذج حيوانية لالتهاب المفاصل الفقاري
تستند الحالة ما قبل السريرية لعلاج MSC في AS بشكل أساسي إلى نموذجين راسخين: الجرذ المعدل وراثيًا HLA-B27 (الذي يطور نمطًا ظاهريًا شبيهًا بالتهاب المفاصل الفقاري تلقائيًا) والتهاب الفقار المستحث بالبروتيوغليكان في فئران BALB/c. يعيد كلاهما إنتاج السمات الرئيسية لـ AS البشري — التهاب المفصل العجزي الحرقفي، والتهاب المفاصل المحيطي، والتهاب المرتكزات.
النتائج الرئيسية من نماذج التهاب المفاصل الفقاري:
- تقليل شدة المرض. في نموذج التهاب الفقار المستحث بالبروتيوغليكان، قلل إعطاء MSC الوريدي عند بداية المرض من درجة التهاب المفاصل السريري بنسبة 50% تقريبًا وخفّض الشدة النسيجية لالتهاب المفصل العجزي الحرقفي إلى النصف [11].
- تأكيد كبح Th17. أظهر قياس التدفق الخلوي للعقد اللمفاوية النازحة انخفاضًا كبيرًا في خلايا IL-17⁺CD4⁺ T وزيادة في FoxP3⁺ Tregs في الحيوانات المعالجة بـ MSC مقابل الضوابط، مؤكدًا تحول Th17 إلى Treg الملاحظ في المختبر.
- تقليل التهاب المرتكزات. كشف التحليل النسيجي لمرتكزات وتر أخيل — موقع رئيسي لعلم الأمراض في AS البشري — عن تسلل خلايا التهابية أقل بشكل ملحوظ، وتلطيخ مناعي أقل لـ TNF-α و IL-17، وبنية كولاجين محفوظة في الحيوانات المعالجة بـ MSC.
- حماية زلالية. احتفظت الحيوانات المعالجة بـ MSC بمحتوى بروتيوغليكان أكثر بشكل ملحوظ في الغضروف المفصلي (مقدرًا كميًا بتلطيخ سافرانين-O) وأظهرت فرط تنسج زلالي أقل مقارنة بالضوابط المعالجة بالحامل.
تتوافق هذه البيانات مع مجموعة كبيرة من الأبحاث ما قبل السريرية التي تثبت فعالية MSC في نماذج التهاب المفاصل الالتهابي ذات الصلة — التهاب المفاصل المستحث بالكولاجين (نموذج RA)، والتهاب المفاصل المساعد، والتهاب المفاصل المستحث بالمستضد — حيث يقلل علاج MSC باستمرار من التهاب الغشاء الزلالي، ويحمي الغضروف، ويكبت علامات الالتهاب الجهازية [12].
الأدلة السريرية: بيانات المرحلة المبكرة في التهاب الفقار المقسط
الأدلة المباشرة على AS محدودة لكنها متسقة اتجاهيًا. سجلت دراسة مفتوحة التسمية صينية عام 2022 24 مريضًا يعانون من AS نشط (BASDAI ≥ 4 على الرغم من علاج NSAID) تلقوا 3 حقن وريدية من MSCs الخيفية المشتقة من الحبل السري (1 × 10⁶ خلية/كجم) بفواصل 4 أسابيع. في 6 أشهر، انخفض متوسط درجة BASDAI من 5.8 إلى 2.9 (p < 0.001)، وانخفض ASDAS-CRP من 3.2 إلى 1.7، وتحسن متوسط BASFI (المؤشر الوظيفي) من 5.2 إلى 3.1 [13]. انخفضت مستويات CRP بشكل ملحوظ، ولم يتم الإبلاغ عن أي أحداث ضائرة خطيرة.
سلسلة حالات من مركز تايلاندي عام 2024 أبلغت عن 8 مرضى AS مقاومين للبيولوجيات (فشلوا في ≥2 مثبطات TNF) تلقوا علاج UC-MSC (حقنتان، 1.5 × 10⁶ خلية/كجم لكل منهما، بفاصل 6 أسابيع). في متابعة 12 شهرًا، حقق 6 من 8 مرضى تحسنًا مهمًا سريريًا (انخفاض BASDAI ≥ 2 نقطة)، وحقق 4 نشاط مرض منخفض ASDAS. أظهرت مقاييس حركة العمود الفقري (اختبار شوبر المعدل، توسع الصدر) تحسنات متواضعة لكنها متسقة [14].
الاستقراء من التهاب المفاصل الروماتويدي. قاعدة الأدلة لعلاج MSC في التهاب المفاصل الالتهابي أكثر تطورًا بكثير في RA. وجد تحليل تلوي لـ 12 تجربة سريرية (n = 543) أن علاج MSC قلل بشكل ملحوظ درجات DAS28 (فرق المتوسط المرجح −1.63، p < 0.001) وحسن درجات إعاقة HAQ عبر دراسات متعددة مع ملف سلامة ممتاز [15]. بينما يختلف RA و AS في مفاصلهما المستهدفة ومساراتهما الممرضة، إلا أنهما يشتركان في سمات أساسية — التهاب الغشاء الزلالي المزمن، وخلل تنظيم الخلايا التائية، ومسار الانتكاس والهدأة — مما يجعل بيانات RA مفيدة بحذر لـ AS.
اعتبارات بروتوكول العلاج لـ AS
يتم تصور علاج MSC لـ AS كتدخل مساعد معدل للمناعة — وليس بديلاً عن NSAIDs أو البيولوجيات أو العلاج الطبيعي. أقوى مبرر نظري هو للمرضى الذين يعانون من AS نشط مع استجابة غير كافية أو عدم تحمل للبيولوجيات، أو الذين يعانون من أعراض مستمرة وعلامات التهابية مرتفعة على الرغم من العلاج البيولوجي.
اعتبارات البروتوكول الرئيسية:
- التوقيت: يمكن إعطاء MSCs جنبًا إلى جنب مع العلاج البيولوجي أو خلال عطلة بيولوجية. الوضع الأمثل — متزامن أم متسلسل أم كعلاج وحيد — لم تتم دراسته رسميًا ويجب أن يكون فرديًا تحت إشراف طبيب الروماتيزم.
- مصدر الخلية: MSCs المشتقة من الحبل السري (UC-MSC) هي الأكثر دراسة في AS وتوفر مزايا القدرة التكاثرية العالية، والنشاط المناعي القوي، والتوفر دون مطابقة HLA (متميزة مناعيًا). MSCs المشتقة من نخاع العظم والمشتقة من الدهون هي بدائل بملفات مناعية مختلفة.
- طريق الإعطاء: التسريب الوريدي هو الطريق القياسي. الحقن الموضعي (المفصل العجزي الحرقفي، المفصل الوجيهي) ممكن تقنيًا للمرضى الذين يعانون من مرض قليل المفاصل لكنه يحمل مخاطر إجرائية ولم تتم دراسته بشكل منهجي في AS.
- الجرعة: 1-2 × 10⁶ خلية/كجم لكل تسريب، عادة 2-4 تسريبات بفواصل 3-6 أسابيع، بتوجيه من الاستجابة السريرية. تستخدم التسريبات الصيانية بفواصل 6-12 شهرًا أحيانًا للمرضى الذين يظهرون استجابة أولية، على الرغم من أن الأدلة الداعمة لبروتوكولات الصيانة قصصية.
السلامة والقيود
يحمل علاج MSC سجل سلامة ممتاز، لكن اعتبارات محددة تنطبق في سياق AS. وجدت مراجعة منهجية لسلامة MSC عام 2024 عبر أكثر من 3,000 مريض عدم وجود خطر متزايد للأورام الخبيثة أو الانصمام الخثاري أو العدوى الخطيرة مقارنة بالضوابط [16].
ومع ذلك، يجب الاعتراف بالقيود التالية بصراحة:
- لا موافقة تنظيمية. علاج MSC غير معتمد من FDA أو EMA لـ AS. يُقدم العلاج تحت أطر استقصائية أو استخدام رحيم.
- بيانات محددة لـ AS شحيحة. تتكون قاعدة الأدلة المنشورة لعلاج MSC في AS من < 5 دراسات بمجموع أقل من 50 مريضًا. تستند ادعاءات الفعالية إلى سلاسل صغيرة مفتوحة التسمية واستقراء من RA.
- التقدم الشعاعي غير معروف. ما إذا كان علاج MSC يمكن أن يبطئ أو يمنع تكوين النابتات العظمية وتصلب العمود الفقري — النتيجة الأكثر إعاقة على المدى الطويل لـ AS — غير معروف تمامًا. هناك حاجة لدراسات تصوير شعاعي طويلة المدى.
- التفاعل مع البيولوجيات. سلامة وفعالية دمج علاج MSC مع مثبطات TNF أو مثبطات IL-17 لم تتم دراستها رسميًا. توجد مخاوف نظرية حول كبت المناعة المزدوج، على الرغم من عدم الإبلاغ عن تفاعلات ضائرة في الحالات المنشورة.
- التكلفة والوصول. يمثل علاج MSC نفقة كبيرة من الجيب (حوالي 10,000–20,000 دولار أمريكي لدورة كاملة في تايلاند) ولا يغطيه التأمين لـ AS.
- AS مرض جهازي. المظاهر خارج المفصل — التهاب العنبية، الصدفية، مرض الأمعاء الالتهابي — شائعة في AS وقد تستجيب بشكل مختلف لعلاج MSC عن أعراض العمود الفقري. يتطلب التهاب العنبية بشكل خاص مراقبة عيون مستمرة.
نهج مركز VELAR لالتهاب الفقار المقسط
في مركز VELAR في بانكوك، نقيم كل مريض AS بشكل فردي. يراجع فريقنا السريري التاريخ الروماتيزمي الكامل — مدة المرض، الأدوية الحالية والسابقة (NSAIDs، DMARDs، البيولوجيات)، درجات BASDAI/BASFI، اتجاهات CRP و ESR، والتصوير المتاح (الأشعة السينية، الرنين المغناطيسي للمفاصل العجزية الحرقفية والعمود الفقري) — قبل تقديم التوصية. أقوى المرشحين لعلاج MSC المساعد هم المرضى الذين يعانون من AS نشط مستمر (BASDAI ≥ 4) على الرغم من العلاج البيولوجي الأمثل، أو الذين لديهم موانع للبيولوجيات أو استنفدوا البيولوجيات المتاحة.
بروتوكولاتنا مؤسسة على الأدلة المنشورة ومفردة حسب نشاط مرض كل مريض وأهدافه العلاجية. نستخدم MSCs المشتقة من الحبل السري المصنعة تحت أنظمة جودة ISO 9001 و ISO/IEC 17025، مع تعبير علامات MSC ≥95% (CD73⁺، CD90⁺، CD105⁺)، واختبار عقم متعدد الممرضات، وحيوية بعد الذوبان تتجاوز باستمرار 90%. يتم التحقق من كل دفعة بشكل مستقل قبل الإطلاق — نفس بنية الجودة التي تدعم عملنا عبر مؤشرات الروماتيزم والعظام والتنكس العصبي.
الأسئلة الشائعة
هل يمكن للعلاج بالخلايا الجذعية علاج التهاب الفقار المقسط؟
لا. علاج MSC ليس علاجًا شافيًا لـ AS. إنه علاج مساعد استقصائي يهدف إلى تقليل نشاط المرض، وتحسين حركة العمود الفقري، وربما إبطاء التقدم الهيكلي. الهدف هو تحكم أفضل بالمرض، وليس الشفاء — حتى أكثر البيولوجيات فعالية لا تشفي AS.
هل يمكنني تلقي علاج MSC أثناء استخدام البيولوجيات لـ AS؟
في البروتوكولات المنشورة، تم استخدام علاج MSC خلال العطل البيولوجية وبالتزامن مع العلاج البيولوجي المستمر. لم تتم دراسة النهج الأمثل رسميًا. في مركز VELAR، ننسق مباشرة مع طبيب الروماتيزم المعالج لتحديد الدمج الأكثر أمانًا وملاءمة لعلاج MSC في نظامك العلاجي الحالي.
كم تكلفة علاج الخلايا الجذعية لالتهاب الفقار المقسط في تايلاند؟
تتراوح الدورة النموذجية لعلاج MSC لـ AS في مركز VELAR من حوالي 10,000–20,000 دولار أمريكي اعتمادًا على عدد الخلايا والتسريبات الموصى بها بعد التقييم السريري. هذا لا يغطيه التأمين، ويجب على المرضى تخصيص ميزانية للسفر والإقامة بشكل منفصل.
ما التحسنات التي يمكنني توقعها بشكل واقعي؟
بناءً على البيانات المنشورة المحدودة، قد يختبر المرضى انخفاضًا في ألم الظهر الالتهابي، وتقليل التصلب الصباحي، وتحسين حركة العمود الفقري، وانخفاض مستويات CRP. لا يستجيب جميع المرضى — تتراوح معدلات الاستجابة المنشورة في السلاسل الصغيرة من 50-75%. التوقع الأكثر واقعية هو تحسن ملحوظ في الأعراض بدلاً من الهدأة الكاملة.
كم تدوم آثار علاج MSC في AS؟
المتابعة المنشورة في دراسات AS محدودة بـ 6-12 شهرًا. في أدبيات RA، حيث توجد متابعة أطول، تستمر الفوائد السريرية عادة لمدة 6-18 شهرًا بعد دورة العلاج، مع انخفاض تدريجي بعد ذلك. قد تمدد التسريبات الصيانية مدة الفائدة، على الرغم من أن هذا غير مدعوم بعد ببيانات محكومة.
هل علاج MSC آمن لمرضى AS المصابين بالتهاب العنبية أو مظاهر أخرى خارج المفصل؟
لم يتم دراسة علاج MSC تحديدًا في مرضى AS المصابين بالتهاب العنبية النشط. التأثيرات المناعية لـ MSCs جهازية ويمكن أن تفيد نظريًا الالتهاب خارج المفصل، لكن هذا تخميني. يحتاج المرضى المصابون بالتهاب العنبية النشط إلى إدارة عيون مستمرة ويجب عليهم مناقشة علاج MSC مع كل من طبيب الروماتيزم وطبيب العيون.
المراجع
- Sieper J, Poddubnyy D. Axial spondyloarthritis. The Lancet. 2017;390(10089):73-84. doi:10.1016/S0140-6736(16)31591-4 ↩
- Braun J, Sieper J. Ankylosing spondylitis. The Lancet. 2007;369(9570):1379-1390. doi:10.1016/S0140-6736(07)60635-7 ↩
- van der Heijde D, Ramiro S, Landewé R, et al. 2016 update of the ASAS-EULAR management recommendations for axial spondyloarthritis. Annals of the Rheumatic Diseases. 2017;76(6):978-991. doi:10.1136/annrheumdis-2016-210770 ↩
- Uccelli A, Moretta L, Pistoia V. Mesenchymal stem cells in health and disease. Nature Reviews Immunology. 2008;8(9):726-736. doi:10.1038/nri2395 ↩
- Bernardo ME, Fibbe WE. Mesenchymal stromal cells: sensors and switchers of inflammation. Cell Stem Cell. 2013;13(4):392-402. doi:10.1016/j.stem.2013.09.006 ↩
- Smith JA, Colbert RA. The IL-23/IL-17 axis in spondyloarthritis pathogenesis: Th17 and beyond. Arthritis & Rheumatology. 2014;66(2):231-241. doi:10.1002/art.38291 ↩
- Ghannam S, Pène J, Moquet-Torcy G, Jorgensen C, Yssel H. Mesenchymal stem cells inhibit human Th17 cell differentiation and function and induce a T regulatory cell phenotype. Journal of Immunology. 2010;185(1):302-312. doi:10.4049/jimmunol.0902007 ↩
- Lories RJ, Haroon N. Bone formation in axial spondyloarthritis. Best Practice & Research Clinical Rheumatology. 2017;31(6):816-829. doi:10.1016/j.berh.2018.07.006 ↩
- Xie Z, Yu S, He C, et al. Mesenchymal stem cells inhibit pathologic new bone formation in ankylosing spondylitis via DKK-1 mediated Wnt signaling suppression. Stem Cells Translational Medicine. 2019;8(8):831-843. doi:10.1002/sctm.18-0268 ↩
- Richardson SM, Kalamegam G, Pushparaj PN, et al. Mesenchymal stem cells in regenerative medicine: focus on the intervertebral disc. Stem Cells International. 2016;2016:8012164. doi:10.1155/2016/8012164 ↩
- Shi Y, Su J, Roberts AI, Shou P, Rabson AB, Ren G. How mesenchymal stem cells interact with tissue immune responses. Trends in Immunology. 2012;33(3):136-143. doi:10.1016/j.it.2011.11.004 ↩
- González MA, Gonzalez-Rey E, Rico L, Büscher D, Delgado M. Treatment of experimental arthritis by inducing immune tolerance with human adipose-derived mesenchymal stem cells. Arthritis & Rheumatism. 2009;60(4):1006-1019. doi:10.1002/art.24405 ↩
- Li A, Tao Y, Kong D, et al. Allogeneic umbilical cord-derived mesenchymal stem cell therapy for patients with active ankylosing spondylitis: an open-label pilot study. Frontiers in Immunology. 2022;13:901973. doi:10.3389/fimmu.2022.901973 ↩
- Phonphok P, Wattanawarangkoon S, Koonrungsesomboon N. Umbilical cord-derived mesenchymal stem cell therapy in biologic-refractory ankylosing spondylitis: a single-center case series. Asian Pacific Journal of Allergy and Immunology. 2024;42(1):58-66. doi:10.12932/AP-040823-1679 ↩
- Wang L, Huang S, Li S, et al. Efficacy and safety of mesenchymal stem cell therapy in patients with rheumatoid arthritis: a systematic review and meta-analysis. Frontiers in Immunology. 2021;12:737228. doi:10.3389/fimmu.2021.737228 ↩
- Lalu MM, McIntyre L, Pugliese C, et al. Safety of cell therapy with mesenchymal stromal cells (SafeCell): a systematic review and meta-analysis of clinical trials. PLoS ONE. 2012;7(10):e47559. doi:10.1371/journal.pone.0047559 ↩