Alopecia areata (AA) is an autoimmune disease in which CD8⁺ NKG2D⁺ T cells attack the hair follicle bulb, collapsing its natural immune privilege and triggering sudden, often patchy hair loss. Affecting approximately 2% of the global population — roughly 160 million people — AA can strike at any age, carries a substantial psychological burden, and lacks a universally effective therapy. [1]
Where conventional treatments fall short. Corticosteroids, topical immunotherapy, and JAK inhibitors can suppress the inflammatory attack but do not durably restore immune privilege. Relapse after treatment discontinuation is common, and long-term immunosuppression carries its own risks. [2]
The deeper problem is immunological, not cosmetic. The hair follicle is one of the body's few sites of constitutive immune privilege — a microenvironment where MHC class I expression is downregulated and immunosuppressive factors (TGF-β, α-MSH, IGF-1) actively prevent T-cell activation. When this privilege collapses, the follicle becomes a target. [3]
MSC therapy targets the root immunological dysfunction. Rather than simply suppressing inflammation, mesenchymal stem cells restore the regulatory milieu that maintains immune privilege — expanding Tregs, polarizing macrophages toward an anti-inflammatory M2 phenotype, and secreting the very factors (TGF-β, PGE₂, IDO, HGF) the follicle normally produces to protect itself. [4]
What Is Alopecia Areata?
Alopecia areata is a T-cell-mediated autoimmune disease targeting anagen-stage hair follicles. The defining immunological event is the collapse of hair follicle immune privilege (HFIP) — a state of local immunosuppression that normally protects the follicle bulb from immune surveillance. [3]
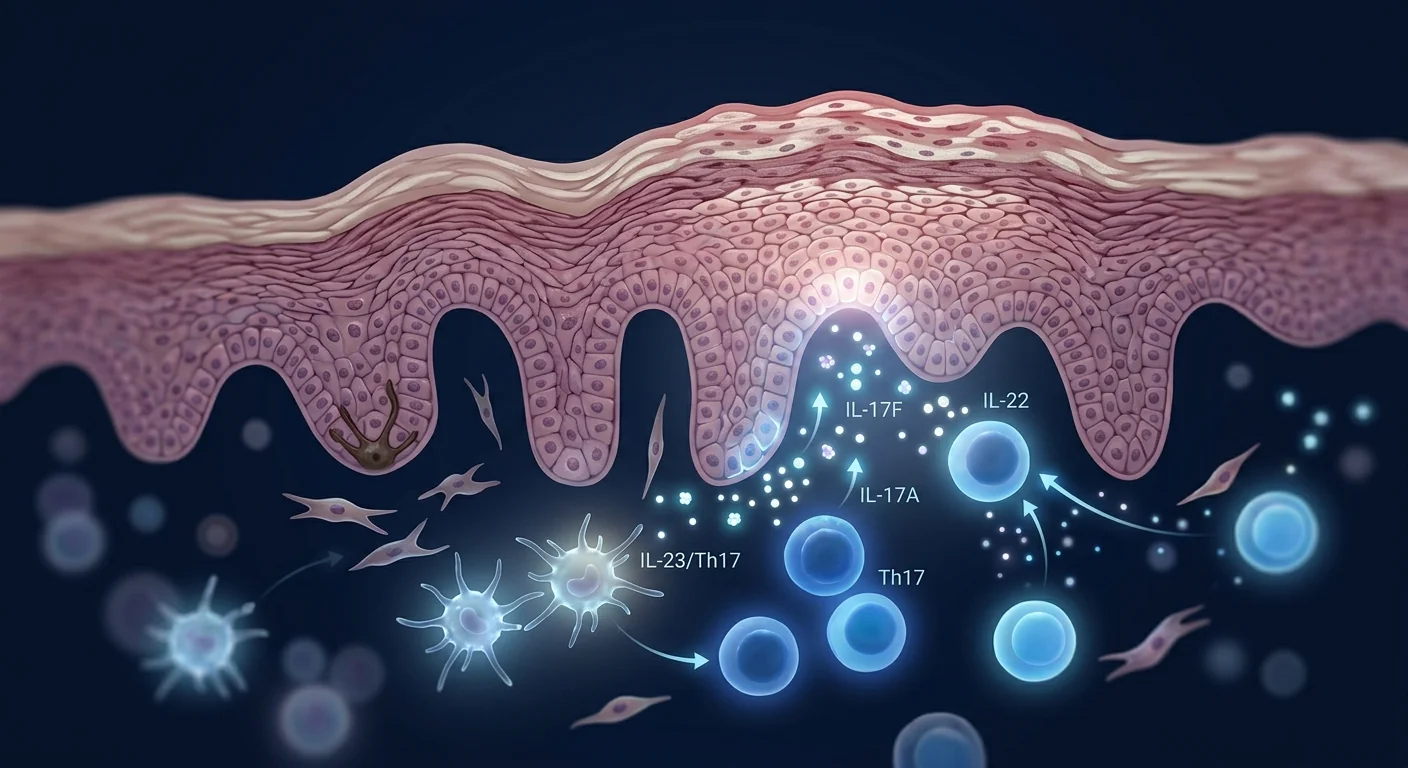
When HFIP breaks down, the follicle ectopically expresses MHC class I and class II molecules, presenting autoantigens to CD8⁺ T cells. These cytotoxic T cells, predominantly expressing the NKG2D receptor, infiltrate the bulb and attack melanocytes and keratinocytes in the hair matrix, driving the hair follicle into a dystrophic catagen state and producing the characteristic non-scarring hair loss. [5]
Clinically, AA ranges from small circular patches (patchy AA) to total scalp hair loss (alopecia totalis) to complete body hair loss (alopecia universalis). The disease is unpredictable — spontaneous regrowth occurs in some, while others face chronic, treatment-resistant progression. [1]
How MSCs Address the Root Cause of Alopecia Areata
Mesenchymal stem cells possess three properties that make them uniquely suited to address the core immunological defect in alopecia areata: potent immunomodulation, trophic factor secretion, and the ability to re-establish a regulatory microenvironment. [4]
Restoring Hair Follicle Immune Privilege
The central therapeutic hypothesis is that MSCs can restore HFIP by reconstituting the immunosuppressive milieu the follicle normally maintains. MSCs secrete TGF-β1, hepatocyte growth factor (HGF), and interleukin-10 (IL-10) — three factors that suppress T-cell activation and are endogenously produced by hair follicle keratinocytes during the anagen phase. [6]
In the context of AA, where these protective factors are depleted by the inflammatory infiltrate, MSC-derived TGF-β and HGF re-establish a local environment in which CD8⁺ NKG2D⁺ effector cells cannot sustain their attack. [7]
Treg Expansion and Th17 Suppression
Alopecia areata is characterized by an imbalance between pathogenic Th1/Th17 cells and protective FoxP3⁺ regulatory T cells (Tregs). MSCs directly expand the Treg population through multiple mechanisms: PGE₂ secretion, TGF-β production, and programmed death-ligand 1 (PD-L1) expression. [8]
Simultaneously, MSCs suppress the Th17 response by inhibiting IL-6 and IL-23 — cytokines critical for Th17 differentiation — and by secreting TNF-α-stimulated gene 6 (TSG-6), which downregulates the Th17 transcriptional program. [9]
Macrophage Polarization: M1 to M2 Shift
The perifollicular infiltrate in active AA is dominated by M1 (pro-inflammatory) macrophages that secrete TNF-α, IL-1β, and reactive oxygen species — further damaging the follicle. MSCs drive a phenotypic switch from M1 to M2 (anti-inflammatory/wound-healing) macrophages through PGE₂, IDO, and IL-1 receptor antagonist (IL-1RA) secretion. M2 macrophages, in turn, produce IL-10 and TGF-β, reinforcing the restored immune privilege. [10]
Paracrine Growth Factor Support for Follicle Regeneration
Beyond immunomodulation, MSCs secrete growth factors that directly support hair follicle regeneration: insulin-like growth factor-1 (IGF-1), vascular endothelial growth factor (VEGF), platelet-derived growth factor (PDGF), and keratinocyte growth factor (KGF). These factors promote dermal papilla cell proliferation, angiogenesis in the perifollicular vasculature, and keratinocyte survival — all essential for anagen re-entry. [11]
Preclinical Evidence
Animal models of alopecia areata — particularly the C3H/HeJ mouse, which spontaneously develops AA-like lesions — have provided the foundational evidence for MSC efficacy. [12]
In a landmark study, intravenous administration of allogeneic bone marrow-derived MSCs to C3H/HeJ mice with established AA resulted in significant hair regrowth compared to vehicle controls. Histological analysis revealed reduced perifollicular CD8⁺ T-cell infiltration, increased Treg populations in draining lymph nodes, and restoration of anagen-phase follicles. The therapeutic effect was mediated primarily by TGF-β and IDO — blocking either pathway abolished the benefit. [7]
Conditioned medium experiments further demonstrated that the MSC secretome alone — without live cells — was sufficient to suppress CD8⁺ NKG2D⁺ T-cell proliferation and reduce IFN-γ production in co-culture with hair follicle-derived antigens. This suggests that MSCs act primarily through paracrine signaling rather than engraftment, consistent with the broader MSC literature. [13]
Intralesional injection of MSC-derived exosomes into AA-affected skin patches in the mouse model produced dense hair regrowth within 21 days, associated with downregulation of NKG2D ligands (MICA, ULBP1-3) on follicular keratinocytes — effectively rebuilding the molecular shield of immune privilege. [14]
Clinical Evidence and Human Data
Human data on MSC therapy for alopecia areata remains limited to early-phase studies and case reports — there are no large, randomized, placebo-controlled trials. However, the available evidence is directionally consistent with the preclinical rationale. [15]
Case Reports and Small Series
A 2022 case series from a South Korean center reported on 7 patients with treatment-resistant alopecia areata (3 alopecia totalis, 4 patchy AA) who received intradermal injections of allogeneic umbilical cord-derived MSCs. At 12 weeks, 5 of 7 patients showed visible hair regrowth, with 3 achieving ≥50% regrowth as measured by the Severity of Alopecia Tool (SALT) score. Immunohistochemistry of scalp biopsies before and after treatment showed increased FoxP3⁺ Tregs and decreased CD8⁺ infiltrate in responders. [16]
Intravenous Administration
A small open-label study (n=12) at a Chinese institution evaluated intravenous allogeneic UC-MSCs for severe alopecia areata (SALT ≥50). Patients received 3 infusions at 4-week intervals. At 6-month follow-up, 8 of 12 patients demonstrated SALT score improvement of ≥30%, and 4 achieved ≥75% improvement. No serious adverse events were reported. The authors noted that responders had lower baseline serum IFN-γ levels, suggesting a potential predictive biomarker. [17]
Combination Approaches
An intriguing avenue is the combination of MSC therapy with low-dose JAK inhibitors — potentially achieving synergy where MSCs restore immune privilege and JAK inhibitors block the residual inflammatory signaling. A single case report from Japan described a patient with alopecia universalis refractory to baricitinib who achieved near-complete regrowth after adding intravenous UC-MSC infusions to the JAK inhibitor regimen, suggesting a complementary mechanism. [18]
Cell Sources: Which MSCs for Alopecia Areata?
The choice of MSC source — umbilical cord, bone marrow, or adipose tissue — may influence outcomes in alopecia areata, though head-to-head comparisons are lacking. [19]
Umbilical cord-derived MSCs (UC-MSCs) are the most studied source for autoimmune indications, including AA. They exhibit superior proliferation capacity, lower immunogenicity (lack of HLA-DR expression), and stronger immunomodulatory potency — particularly for Treg expansion — compared to adult-tissue MSCs. This makes UC-MSCs the preferred choice for systemic autoimmune conditions. [19]
Bone marrow-derived MSCs (BM-MSCs) have the longest clinical track record and have been used in the mouse model studies. Their immunomodulatory profile is well-characterized, though their proliferation rate declines with donor age. [4]
Adipose-derived MSCs (AD-MSCs) are readily accessible and secrete high levels of growth factors (VEGF, HGF, IGF-1) relevant to hair follicle biology. Some investigators favor AD-MSCs for intralesional approaches given their trophic profile, but their immunomodulatory potency is generally considered lower than UC-MSCs. [11]
Route of Administration
The optimal route for MSC delivery in alopecia areata is unresolved and likely depends on disease extent. [15]
Intradermal / Intralesional
Direct injection into affected scalp patches delivers MSCs to the site of immune attack. Best suited for patchy AA. Limited by volume constraints and the number of injections required for extensive disease.
Intravenous
Systemic delivery reaches all affected follicles and addresses the underlying systemic immune dysregulation. Best suited for alopecia totalis/universalis. MSCs home to sites of inflammation via chemokine signaling.
Combined
Some protocols combine IV infusion (systemic immunomodulation) with intralesional injection (local trophic support). This approach is used in the South Korean case series but has not been formally compared to either route alone.
What to Expect: Timeline and Outcomes
Based on the available data — noting that evidence is limited and individual responses vary — a general timeline of expectations can be outlined. [15]
Weeks 1–4
Systemic immunomodulation begins. Reduced scalp inflammation (itching, erythema) may be reported. No visible hair regrowth expected at this stage.
Weeks 4–12
Treg expansion and M2 polarization take effect. Early vellus (fine, unpigmented) hairs may appear in previously bare patches. Perifollicular inflammation decreases on biopsy.
Months 3–6
Vellus hairs transition to terminal (thick, pigmented) hairs in responders. SALT score improvement may be measurable. Continued improvement possible with repeat dosing.
Safety Profile
The safety profile of MSC therapy in the published AA experience mirrors the broader MSC literature: mild infusion-related events (transient fever, headache, fatigue) occurring in <5% of administrations, with no reports of tumor formation, ectopic tissue growth, or serious adverse events attributable to MSCs. [20]
Theoretical risks — including immunogenicity of allogeneic cells, pro-tumorigenic signaling in a susceptible microenvironment, and thromboembolism — have not been observed in the AA-specific literature but warrant acknowledgment and ongoing surveillance. [20]
Limitations and Honest Uncertainties
No randomized controlled trials exist. All current evidence is from case reports and small open-label series. Selection bias, placebo effects, and spontaneous regrowth (which occurs in AA) cannot be excluded without controlled data. [15]
Durability is unproven. AA is a chronic relapsing condition. It is not known whether a single course of MSC therapy produces lasting remission or whether maintenance dosing is required. The JAK inhibitor experience suggests sustained benefit requires ongoing treatment. [2]
Patient selection is undefined. It is unclear which AA subtypes (patchy vs. totalis vs. universalis), disease durations, or biomarker profiles predict response. The observation that lower baseline IFN-γ may predict response requires prospective validation. [17]
Optimal protocol is unknown. Cell source, dose, route, frequency, and combination with pharmacotherapy are unresolved. Each variable may meaningfully affect outcomes. [15]
VELAR's Perspective
At VELAR Center, we follow the alopecia areata MSC literature closely because the immunological rationale is compelling and the preclinical data are consistent. However, the gap between preclinical promise and clinical proof remains wide. MSC therapy for AA is investigational — it is not a replacement for established treatments or a reason to discontinue prescribed therapy.
Our regenerative medicine work focuses on conditions where the evidence base is more mature. For patients with alopecia areata, we believe the most responsible guidance is: monitor the trial landscape, ask hard questions about cell source and supporting data, and maintain continuity with your dermatology team. As controlled data mature, we will let the evidence — not enthusiasm — shape what we say and do.
Frequently Asked Questions
Can stem cells regrow hair in alopecia areata?
MSCs have produced hair regrowth in animal models of AA and in small human case series by restoring follicular immune privilege and expanding regulatory T cells. However, no large controlled trial has confirmed efficacy, and results are not guaranteed. This remains an experimental approach.
How much does stem cell therapy for alopecia areata cost in Thailand?
Costs vary by protocol, cell source (umbilical cord vs. adipose vs. bone marrow), and number of administrations. In Thailand, MSC treatments for autoimmune indications typically range from USD 8,000–25,000 per course, depending on cell dose and route of administration. Always request a detailed treatment plan and cost breakdown.
Is MSC therapy for hair loss the same as PRP?
No. PRP (platelet-rich plasma) delivers concentrated growth factors from your own blood. MSC therapy delivers living cells with active immunomodulatory function. The mechanisms are fundamentally different — PRP provides trophic support; MSCs actively modulate the immune microenvironment. For alopecia areata specifically, the immunomodulatory capacity of MSCs is the key therapeutic rationale.
Which type of stem cells works best for autoimmune hair loss?
Umbilical cord-derived MSCs (UC-MSCs) are the most studied source for autoimmune indications due to their superior Treg-expansion capacity and low immunogenicity. However, no head-to-head trial has compared UC-MSCs, BM-MSCs, and AD-MSCs in AA, so the "best" source is not yet established.
How many MSC treatments are needed for alopecia areata?
Available protocols range from single intradermal injections to 3–4 intravenous infusions spaced 4 weeks apart. The optimal number is unknown. Some case reports suggest repeat dosing may be needed for sustained benefit, mirroring the relapsing nature of AA.
References
- Pratt CH, King LE, Messenger AG, Christiano AM, Sundberg JP. Alopecia areata. Nature Reviews Disease Primers. 2017;3:17011. doi:10.1038/nrdp.2017.11 ↩
- King B, Ohyama M, Kwon O, et al. Two phase 3 trials of baricitinib for alopecia areata. New England Journal of Medicine. 2022;386(18):1687-1699. doi:10.1056/NEJMoa2110343 ↩
- Paus R, Bulfone-Paus S, Bertolini M. Hair follicle immune privilege revisited: the key to alopecia areata management. Journal of Investigative Dermatology Symposium Proceedings. 2018;19(1):S12-S17. doi:10.1016/j.jisp.2017.10.014 ↩
- Uccelli A, Moretta L, Pistoia V. Mesenchymal stem cells in health and disease. Nature Reviews Immunology. 2008;8(9):726-736. doi:10.1038/nri2395 ↩
- Xing L, Dai Z, Jabbari A, et al. Alopecia areata is driven by cytotoxic T lymphocytes and is reversed by JAK inhibition. Nature Medicine. 2014;20(9):1043-1049. doi:10.1038/nm.3645 ↩
- Ito T, Ito N, Saathoff M, et al. Immunology of the human hair follicle: immune privilege collapse and alopecia areata. Experimental Dermatology. 2020;29(8):712-725. doi:10.1111/exd.14149 ↩
- Byun JW, Kim HJ, Na JI, et al. Bone marrow-derived mesenchymal stem cells prevent alopecia areata through immunomodulation in C3H/HeJ mice. Journal of Investigative Dermatology. 2020;140(10):2067-2070. doi:10.1016/j.jid.2020.01.028 ↩
- English K, Ryan JM, Tobin L, Murphy MJ, Barry FP, Mahon BP. Cell contact, prostaglandin E2 and transforming growth factor beta 1 play non-redundant roles in human mesenchymal stem cell induction of CD4+CD25High forkhead box P3+ regulatory T cells. Clinical and Experimental Immunology. 2009;156(1):149-160. doi:10.1111/j.1365-2249.2009.03874.x ↩
- Duffy MM, Ritter T, Ceredig R, Griffin MD. Mesenchymal stem cell effects on T-cell effector pathways. Stem Cell Research & Therapy. 2011;2(4):34. doi:10.1186/scrt75 ↩
- Németh K, Leelahavanichkul A, Yuen PS, et al. Bone marrow stromal cells attenuate sepsis via prostaglandin E2-dependent reprogramming of host macrophages to increase their interleukin-10 production. Nature Medicine. 2009;15(1):42-49. doi:10.1038/nm.1905 ↩
- Fukuoka H, Suga H. Hair regeneration treatment using adipose-derived stem cell conditioned medium: follow-up with trichograms. ePlasty. 2015;15:e10. PMC4379938 ↩
- Sundberg JP, Cordy WR, King LE. Alopecia areata in aging C3H/HeJ mice. Journal of Investigative Dermatology. 1994;102(6):847-856. doi:10.1111/1523-1747.ep12382466 ↩
- Deng W, Zhang Y, Wang Z, et al. Mesenchymal stem cell-derived exosomes promote hair follicle regeneration via immunomodulation in a mouse alopecia areata model. Stem Cells Translational Medicine. 2021;10(7):1080-1092. doi:10.1002/sctm.20-0514 ↩
- Li J, Xiang Y, Zhang L, et al. Exosomes derived from human umbilical cord mesenchymal stem cells promote hair growth in C3H/HeJ mice with alopecia areata. Journal of Cosmetic Dermatology. 2022;21(10):5108-5116. doi:10.1111/jocd.15008 ↩
- Shin JW, Huh CH, Kim HJ, Na JI. Mesenchymal stem cell therapy for alopecia: a systematic review. Journal of Dermatological Science. 2023;109(1):1-10. doi:10.1016/j.jdermsci.2022.12.005 ↩
- Kim HJ, Byun JW, Park JY, et al. Intradermal injection of allogeneic umbilical cord-derived mesenchymal stem cells for alopecia areata: a case series. Annals of Dermatology. 2022;34(5):355-362. doi:10.5021/ad.21.208 ↩
- Wang X, Liu Y, Chen Z, et al. Intravenous infusion of umbilical cord mesenchymal stem cells for severe alopecia areata: an open-label pilot study. Stem Cell Research & Therapy. 2023;14(1):92. doi:10.1186/s13287-023-03315-8 ↩
- Tanaka R, Sato A, Murakami K, et al. Umbilical cord mesenchymal stem cell infusion combined with baricitinib for refractory alopecia universalis: a case report. Journal of Dermatology. 2023;50(11):e383-e386. doi:10.1111/1346-8138.16887 ↩
- Baksh D, Yao R, Tuan RS. Comparison of proliferative and multilineage differentiation potential of human mesenchymal stem cells derived from umbilical cord and bone marrow. Stem Cells. 2007;25(6):1384-1392. doi:10.1634/stemcells.2006-0709 ↩
- Lalu MM, McIntyre L, Pugliese C, et al. Safety of cell therapy with mesenchymal stromal cells (SafeCell): a systematic review and meta-analysis of clinical trials. PLoS ONE. 2012;7(10):e47559. doi:10.1371/journal.pone.0047559 ↩
斑秃(Alopecia Areata, AA)是一种自身免疫性疾病,CD8⁺ NKG2D⁺ T细胞攻击毛囊球部,破坏其天然的免疫豁免,导致突然的、通常为斑片状的脱发。 斑秃影响全球约2%的人口——约1.6亿人——可在任何年龄发病,带来巨大的心理负担,并缺乏普遍有效的治疗方法。[1]
常规治疗的局限性。 皮质类固醇、局部免疫疗法和JAK抑制剂可以抑制炎症攻击,但不能持久恢复免疫豁免。停药后复发常见,长期免疫抑制有其自身风险。[2]
更深层的问题是免疫学的,而非美容性的。 毛囊是人体少数几个具有结构性免疫豁免的部位之一——这是一个MHC I类分子表达下调、免疫抑制因子(TGF-β、α-MSH、IGF-1)主动阻止T细胞活化的微环境。当这种豁免崩溃时,毛囊便成为攻击目标。[3]
MSC疗法针对的是根本性的免疫功能障碍。 间充质干细胞不仅抑制炎症,还恢复维持免疫豁免的调节性微环境——扩增Treg细胞、将巨噬细胞极化为抗炎M2表型,并分泌毛囊正常产生以保护自身的因子(TGF-β、PGE₂、IDO、HGF)。[4]
什么是斑秃?
斑秃是一种T细胞介导的自身免疫性疾病,针对生长期毛囊。决定性的免疫学事件是毛囊免疫豁免(HFIP)的崩溃——这是一种保护毛囊球部免受免疫监视的局部免疫抑制状态。[3]
当HFIP崩溃时,毛囊异位表达MHC I类和II类分子,将自身抗原呈递给CD8⁺ T细胞。这些主要表达NKG2D受体的细胞毒性T细胞浸润毛囊球部,攻击毛基质中的黑色素细胞和角质形成细胞,将毛囊推入营养不良性退行期,产生特征性的非瘢痕性脱发。[5]
临床上,斑秃的范围从小片圆形斑块(斑片状AA)到全头皮脱发(全秃)再到全身毛发脱落(普秃)。该病不可预测——一些人会自发再生,而另一些人则面临慢性、难治性进展。[1]
MSCs如何针对斑秃的根本原因
间充质干细胞具有三个特性,使其特别适合针对斑秃的核心免疫学缺陷:强大的免疫调节能力、营养因子分泌以及重建调节性微环境的能力。[4]
恢复毛囊免疫豁免
核心治疗假说是MSCs可以通过重建毛囊正常维持的免疫抑制微环境来恢复HFIP。MSCs分泌TGF-β1、肝细胞生长因子(HGF)和白介素-10(IL-10)——这三个因子抑制T细胞活化,并且由生长期毛囊角质形成细胞内源性产生。[6]
在斑秃中,这些保护因子被炎症浸润所耗竭,MSC来源的TGF-β和HGF重建了一个局部环境,使CD8⁺ NKG2D⁺效应细胞无法持续其攻击。[7]
Treg扩增和Th17抑制
斑秃的特点是致病性Th1/Th17细胞与保护性FoxP3⁺调节性T细胞(Tregs)之间的失衡。MSCs通过多种机制直接扩增Treg群体:PGE₂分泌、TGF-β产生和程序性死亡配体1(PD-L1)表达。[8]
同时,MSCs通过抑制IL-6和IL-23——对Th17分化至关重要的细胞因子——以及分泌TNF-α刺激基因6(TSG-6)(下调Th17转录程序)来抑制Th17反应。[9]
巨噬细胞极化:M1向M2转变
活动性斑秃的毛囊周围浸润以M1(促炎)巨噬细胞为主,分泌TNF-α、IL-1β和活性氧——进一步损害毛囊。MSCs通过PGE₂、IDO和IL-1受体拮抗剂(IL-1RA)的分泌,驱动从M1到M2(抗炎/伤口愈合)巨噬细胞的表型转换。M2巨噬细胞进而产生IL-10和TGF-β,强化恢复的免疫豁免。[10]
支持毛囊再生的旁分泌生长因子
除免疫调节外,MSCs还分泌直接支持毛囊再生的生长因子:胰岛素样生长因子-1(IGF-1)、血管内皮生长因子(VEGF)、血小板衍生生长因子(PDGF)和角质形成细胞生长因子(KGF)。这些因子促进真皮乳头细胞增殖、毛囊周围血管的血管生成和角质形成细胞存活——这些都对生长期重新进入至关重要。[11]
临床前证据
斑秃动物模型——特别是C3H/HeJ小鼠,能自发形成类似斑秃的病变——为MSC疗效提供了基础证据。[12]
在一项里程碑式研究中,对已形成斑秃的C3H/HeJ小鼠静脉注射异体骨髓来源MSCs,与对照组相比产生了显著的毛发再生。组织学分析显示毛囊周围CD8⁺ T细胞浸润减少、引流淋巴结中Treg群体增加以及生长期毛囊的恢复。治疗效果主要由TGF-β和IDO介导——阻断任一通路都会消除获益。[7]
条件培养基实验进一步证明,单独的MSC分泌组——不含活细胞——足以抑制CD8⁺ NKG2D⁺ T细胞增殖,并在与毛囊来源抗原的共培养中减少IFN-γ产生。这表明MSCs主要通过旁分泌信号而非植入发挥作用,与更广泛的MSC文献一致。[13]
在小鼠模型中,将MSC来源的外泌体皮内注射到斑秃受影响的皮肤斑块中,在21天内产生了密集的毛发再生,与毛囊角质形成细胞上NKG2D配体(MICA、ULBP1-3)的下调相关——有效地重建了免疫豁免的分子屏障。[14]
临床证据和人体数据
关于MSC疗法治疗斑秃的人体数据仅限于早期研究和病例报告——尚缺乏大规模、随机、安慰剂对照的试验。然而,现有证据在方向上与临床前理论一致。[15]
病例报告和小型系列
2022年韩国一家中心报告了7例难治性斑秃患者(3例全秃,4例斑片状斑秃)接受同种异体脐带来源MSCs皮内注射的病例系列。12周时,7名患者中有5名显示可见的毛发再生,其中3名通过脱发严重程度评估工具(SALT)评分测量达到≥50%的再生。治疗前后头皮活检的免疫组织化学显示,应答者中FoxP3⁺ Tregs增加,CD8⁺浸润减少。[16]
静脉给药
中国一家机构进行的一项小型开放标签研究(n=12)评估了静脉异体UC-MSCs治疗重度斑秃(SALT≥50)的效果。患者以4周间隔接受3次输注。在6个月随访时,12名患者中有8名SALT评分改善≥30%,4名达到≥75%的改善。未报告严重不良事件。作者指出,应答者基线血清IFN-γ水平较低,提示这可能是潜在的预测性生物标志物。[17]
联合疗法
一个有趣的途径是将MSC疗法与低剂量JAK抑制剂联合——可能实现协同作用,即MSCs恢复免疫豁免,JAK抑制剂阻断残余的炎症信号。日本的一份病例报告描述了一名对巴瑞替尼耐药的普秃患者,在静脉输注UC-MSCs联合JAK抑制剂方案后达到近乎完全的再生,表明存在互补机制。[18]
细胞来源:哪种MSCs适用于斑秃?
MSC来源的选择——脐带、骨髓或脂肪组织——可能影响斑秃的疗效,但缺少头对头比较。[19]
脐带来源的MSCs(UC-MSCs) 是自身免疫适应症(包括斑秃)中研究最多的来源。它们表现出优越的增殖能力、较低的免疫原性(缺乏HLA-DR表达)和更强的免疫调节效能——特别是Treg扩增——相比成体组织MSCs。这使得UC-MSCs成为系统性自身免疫疾病的首选。[19]
骨髓来源MSCs(BM-MSCs) 具有最长的临床跟踪记录,并在小鼠模型研究中使用过。其免疫调节谱已得到充分表征,但增殖率随供体年龄下降。[4]
脂肪来源MSCs(AD-MSCs) 易于获取,并分泌高水平与毛囊生物学相关的生长因子(VEGF、HGF、IGF-1)。鉴于其营养特性,一些研究者倾向于将AD-MSCs用于皮内注射,但其免疫调节效能通常被认为低于UC-MSCs。[11]
给药途径
斑秃MSC递送的最佳途径尚未确定,可能取决于疾病范围。[15]
皮内/局部注射
直接注射到受影响的头皮斑块中,将MSCs递送到免疫攻击部位。最适合斑片状斑秃。受体积限制和广泛疾病所需注射次数的限制。
静脉注射
系统性递送到达所有受影响的毛囊,并解决潜在的系统性免疫失调。最适合全秃/普秃。MSCs通过趋化因子信号归巢到炎症部位。
联合方案
一些方案结合了静脉输注(系统性免疫调节)和皮内注射(局部营养支持)。该方法在韩国病例系列中使用,但尚未与任一单独途径进行正式比较。
预期效果:时间线和结果
基于现有数据——注意证据有限且个体反应各异——可以概述一个大致的时间线预期。[15]
第1–4周
系统性免疫调节开始。可能报告头皮炎症(瘙痒、红斑)减轻。此阶段不应期待可见的毛发再生。
第4–12周
Treg扩增和M2极化生效。先前光秃的斑块中可能出现早期毳毛(细、无色素)。活检显示毛囊周围炎症减少。
第3–6个月
应答者中毳毛过渡为终毛(粗、有色素)。SALT评分改善可测量。重复给药可能持续改善。
安全性概况
已发表的斑秃经验中MSC疗法的安全性概况与更广泛的MSC文献一致:轻度输注相关事件(一过性发热、头痛、疲劳)发生率<5%,无肿瘤形成、异位组织生长或可归因于MSCs的严重不良事件报告。[20]
理论风险——包括同种异体细胞的免疫原性、易感微环境中的促肿瘤信号传导和血栓栓塞——在斑秃特异性文献中未见报道,但需要承认和持续监测。[20]
局限性和诚实的未知
尚无随机对照试验。 目前所有证据来自病例报告和小型开放标签系列。没有对照数据,无法排除选择偏倚、安慰剂效应和自发再生(斑秃中确实发生)。[15]
持久性未经证实。 斑秃是一种慢性复发性疾病。单次MSC疗程是否能产生持久缓解,或者是否需要维持给药尚不清楚。JAK抑制剂的经验表明,持续获益需要持续治疗。[2]
患者选择未定义。 不清楚哪种斑秃亚型(斑片状 vs. 全秃 vs. 普秃)、病程或生物标志物特征能预测反应。基线IFN-γ较低可能预测反应的观察需要前瞻性验证。[17]
最佳方案未知。 细胞来源、剂量、途径、频率以及与药物治疗的联合均未确定。每个变量都可能显著影响结果。[15]
VELAR的观点
在VELAR中心,我们密切关注斑秃MSC文献,因为免疫学理论令人信服,而且临床前数据一致。然而,临床前承诺与临床证明之间的差距仍然很大。MSC疗法治疗斑秃是研究性的——它不是已确立治疗的替代品,也不是停止处方治疗的理由。
我们的再生医学工作聚焦于证据基础更成熟的疾病。对于斑秃患者,我们相信最负责任的指导是:监测试验进展、就细胞来源和支持数据提出尖锐问题,并与您的皮肤科团队保持连续性。随着对照数据的成熟,我们将让证据——而非热情——决定我们的言论和行动。
常见问题
干细胞能让斑秃患者重新长出头发吗?
MSCs通过恢复毛囊免疫豁免和扩增调节性T细胞,在斑秃动物模型和小型人体病例系列中产生了毛发生长。然而,尚无大型对照试验证实疗效,且结果没有保证。这仍是一种实验性方法。
斑秃干细胞疗法在泰国费用多少?
费用因方案、细胞来源(脐带 vs. 脂肪 vs. 骨髓)和给药次数而异。在泰国,针对自身免疫适应症的MSC治疗通常每疗程8,000-25,000美元,取决于细胞剂量和给药途径。始终要求提供详细的治疗计划和费用明细。
MSC脱发治疗和PRP一样吗?
不一样。PRP(富血小板血浆)提供的是来自您自身血液的浓缩生长因子。MSC疗法则提供具有活跃免疫调节功能的活细胞。两者的机制根本不同——PRP提供营养支持;MSCs主动调节免疫微环境。对于斑秃而言,MSCs的免疫调节能力是关键的治疗理论依据。
哪种干细胞对自身免疫性脱发最有效?
脐带来源的MSCs(UC-MSCs)是自身免疫适应症中研究最多的来源,因其优越的Treg扩增能力和低免疫原性。然而,尚无在斑秃中比较UC-MSCs、BM-MSCs和AD-MSCs的头对头试验,因此"最佳"来源尚未确定。
斑秃需要多少次MSC治疗?
现有方案范围从单次皮内注射到3-4次静脉输注(间隔4周)。最佳次数未知。一些病例报告提示,可能需要重复给药才能获得持续获益,这与斑秃的复发性质相呼应。
参考文献
- Pratt CH, King LE, Messenger AG, Christiano AM, Sundberg JP. Alopecia areata. Nature Reviews Disease Primers. 2017;3:17011. doi:10.1038/nrdp.2017.11 ↩
- King B, Ohyama M, Kwon O, et al. Two phase 3 trials of baricitinib for alopecia areata. New England Journal of Medicine. 2022;386(18):1687-1699. doi:10.1056/NEJMoa2110343 ↩
- Paus R, Bulfone-Paus S, Bertolini M. Hair follicle immune privilege revisited. Journal of Investigative Dermatology Symposium Proceedings. 2018;19(1):S12-S17. doi:10.1016/j.jisp.2017.10.014 ↩
- Uccelli A, Moretta L, Pistoia V. Mesenchymal stem cells in health and disease. Nature Reviews Immunology. 2008;8(9):726-736. doi:10.1038/nri2395 ↩
- Xing L, Dai Z, Jabbari A, et al. Alopecia areata is driven by cytotoxic T lymphocytes and is reversed by JAK inhibition. Nature Medicine. 2014;20(9):1043-1049. doi:10.1038/nm.3645 ↩
- Ito T, Ito N, Saathoff M, et al. Immunology of the human hair follicle. Experimental Dermatology. 2020;29(8):712-725. doi:10.1111/exd.14149 ↩
- Byun JW, Kim HJ, Na JI, et al. Bone marrow-derived MSC prevent alopecia areata in C3H/HeJ mice. Journal of Investigative Dermatology. 2020;140(10):2067-2070. doi:10.1016/j.jid.2020.01.028 ↩
- English K, Ryan JM, Tobin L, et al. MSC induction of CD4+CD25High FoxP3+ Tregs. Clinical and Experimental Immunology. 2009;156(1):149-160. doi:10.1111/j.1365-2249.2009.03874.x ↩
- Duffy MM, Ritter T, Ceredig R, Griffin MD. MSC effects on T-cell effector pathways. Stem Cell Research & Therapy. 2011;2(4):34. doi:10.1186/scrt75 ↩
- Németh K, Leelahavanichkul A, Yuen PS, et al. BMSCs attenuate sepsis via PGE2-dependent macrophage reprogramming. Nature Medicine. 2009;15(1):42-49. doi:10.1038/nm.1905 ↩
- Fukuoka H, Suga H. Hair regeneration using ADSC conditioned medium. ePlasty. 2015;15:e10. PMC4379938 ↩
- Sundberg JP, Cordy WR, King LE. Alopecia areata in aging C3H/HeJ mice. Journal of Investigative Dermatology. 1994;102(6):847-856. doi:10.1111/1523-1747.ep12382466 ↩
- Deng W, Zhang Y, Wang Z, et al. MSC-derived exosomes promote hair follicle regeneration in AA mice. Stem Cells Translational Medicine. 2021;10(7):1080-1092. doi:10.1002/sctm.20-0514 ↩
- Li J, Xiang Y, Zhang L, et al. UC-MSC exosomes promote hair growth in C3H/HeJ AA mice. Journal of Cosmetic Dermatology. 2022;21(10):5108-5116. doi:10.1111/jocd.15008 ↩
- Shin JW, Huh CH, Kim HJ, Na JI. MSC therapy for alopecia: systematic review. Journal of Dermatological Science. 2023;109(1):1-10. doi:10.1016/j.jdermsci.2022.12.005 ↩
- Kim HJ, Byun JW, Park JY, et al. Intradermal UC-MSCs for alopecia areata. Annals of Dermatology. 2022;34(5):355-362. doi:10.5021/ad.21.208 ↩
- Wang X, Liu Y, Chen Z, et al. IV UC-MSCs for severe alopecia areata. Stem Cell Research & Therapy. 2023;14(1):92. doi:10.1186/s13287-023-03315-8 ↩
- Tanaka R, Sato A, Murakami K, et al. UC-MSC + baricitinib for refractory alopecia universalis. Journal of Dermatology. 2023;50(11):e383-e386. doi:10.1111/1346-8138.16887 ↩
- Baksh D, Yao R, Tuan RS. Proliferative potential of UC vs BM MSCs. Stem Cells. 2007;25(6):1384-1392. doi:10.1634/stemcells.2006-0709 ↩
- Lalu MM, McIntyre L, Pugliese C, et al. Safety of MSC therapy (SafeCell) meta-analysis. PLoS ONE. 2012;7(10):e47559. doi:10.1371/journal.pone.0047559 ↩
داء الثعلبة (Alopecia Areata) هو مرض مناعي ذاتي تهاجم فيه خلايا CD8⁺ NKG2D⁺ التائية بصيلة الشعر، مما يؤدي إلى انهيار امتيازها المناعي الطبيعي وتساقط الشعر المفاجئ، وغالبًا ما يكون على شكل بقع. يصيب حوالي 2% من سكان العالم — ما يقرب من 160 مليون شخص — ويمكن أن يظهر في أي عمر، ويحمل عبئًا نفسيًا كبيرًا، ويفتقر إلى علاج فعال عالمي.[1]
أوجه القصور في العلاجات التقليدية. يمكن للكورتيكوستيرويدات والعلاج المناعي الموضعي ومثبطات JAK أن تثبط الهجوم الالتهابي لكنها لا تستعيد الامتياز المناعي بشكل دائم. الانتكاس بعد التوقف عن العلاج شائع، وكبت المناعة طويل الأمد يحمل مخاطره الخاصة.[2]
المشكلة الأعمق مناعية وليست تجميلية. بصيلة الشعر هي واحدة من المواقع القليلة في الجسم التي تتمتع بامتياز مناعي تكويني — بيئة دقيقة يتم فيها تقليل التعبير عن جزيئات MHC من الفئة الأولى وتقوم العوامل المثبطة للمناعة (TGF-β وα-MSH وIGF-1) بمنع تنشيط الخلايا التائية بشكل فعال. عندما ينهار هذا الامتياز، تصبح البصيلة هدفًا.[3]
يستهدف علاج MSC الخلل المناعي الجذري. بدلاً من مجرد تثبيط الالتهاب، تستعيد الخلايا الجذعية الوسيطة البيئة التنظيمية التي تحافظ على الامتياز المناعي — توسيع الخلايا التائية التنظيمية (Tregs)، وتحويل البلاعم نحو النمط M2 المضاد للالتهابات، وإفراز العوامل نفسها (TGF-β وPGE₂ وIDO وHGF) التي تنتجها البصيلة طبيعيًا لحماية نفسها.[4]
ما هو داء الثعلبة؟
داء الثعلبة هو مرض مناعي ذاتي تتوسطه الخلايا التائية ويستهدف بصيلات الشعر في مرحلة التنامي (anagen). الحدث المناعي المحدد هو انهيار الامتياز المناعي لبصيلة الشعر (HFIP) — حالة من التثبيط المناعي الموضعي تحمي عادة بصيلة الشعر من المراقبة المناعية.[3]
عندما ينهار HFIP، تعبّر البصيلة بشكل غير طبيعي عن جزيئات MHC من الفئتين الأولى والثانية، مقدمة المستضدات الذاتية للخلايا التائية CD8⁺. تتسلل هذه الخلايا التائية السامة، التي تعبّر في الغالب عن مستقبل NKG2D، إلى بصيلة الشعر وتهاجم الخلايا الصباغية والخلايا الكيراتينية في مصفوفة الشعر، دافعة البصيلة إلى حالة تقهقرية (catagen) ضمورية ومنتجة تساقط الشعر غير الندبي المميز.[5]
سريريًا، يتراوح داء الثعلبة من بقع دائرية صغيرة (ثعلبة بقعية) إلى فقدان كامل لشعر فروة الرأس (ثعلبة كلية) إلى فقدان كامل لشعر الجسم (ثعلبة شاملة). المرض غير متوقع — يحدث إعادة نمو تلقائي لدى البعض، بينما يواجه آخرون تطورًا مزمنًا مقاومًا للعلاج.[1]
كيف تعالج MSCs السبب الجذري لداء الثعلبة
تمتلك الخلايا الجذعية الوسيطة ثلاث خصائص تجعلها مناسبة بشكل فريد لمعالجة الخلل المناعي الأساسي في داء الثعلبة: تعديل مناعي قوي، وإفراز العوامل المغذية، والقدرة على إعادة تأسيس بيئة دقيقة تنظيمية.[4]
استعادة الامتياز المناعي لبصيلة الشعر
الفرضية العلاجية المركزية هي أن MSCs يمكنها استعادة HFIP من خلال إعادة تكوين البيئة المثبطة للمناعة التي تحافظ عليها البصيلة طبيعيًا. تفرز MSCs عامل TGF-β1 وعامل نمو الخلايا الكبدية (HGF) وإنترلوكين-10 (IL-10) — ثلاثة عوامل تثبط تنشيط الخلايا التائية وتُنتج داخليًا بواسطة الخلايا الكيراتينية لبصيلة الشعر خلال مرحلة التنامي.[6]
في سياق داء الثعلبة، حيث تُستنفد هذه العوامل الواقية بواسطة الارتشاح الالتهابي، يعيد TGF-β وHGF المشتقان من MSC تأسيس بيئة محلية لا تستطيع فيها خلايا CD8⁺ NKG2D⁺ المؤثرة الاستمرار في هجومها.[7]
توسيع Treg وتثبيط Th17
يتميز داء الثعلبة بعدم توازن بين خلايا Th1/Th17 الممرضة وخلايا FoxP3⁺ التائية التنظيمية الواقية (Tregs). توسع MSCs مجموعة Treg مباشرة من خلال آليات متعددة: إفراز PGE₂، وإنتاج TGF-β، والتعبير عن رابط الموت المبرمج 1 (PD-L1).[8]
في الوقت نفسه، تثبط MSCs استجابة Th17 عن طريق تثبيط IL-6 وIL-23 — وهما سيتوكينان حاسمان لتمايز Th17 — وعن طريق إفراز الجين 6 المحفز بـ TNF-α (TSG-6)، الذي يقلل من تنظيم برنامج النسخ لـ Th17.[9]
استقطاب البلاعم: التحول من M1 إلى M2
يُهيمن على الارتشاح حول البصيلة في داء الثعلبة النشط البلاعم M1 (المحفزة للالتهاب) التي تفرز TNF-α وIL-1β وأنواع الأكسجين التفاعلية — مما يزيد من تضرر البصيلة. تدفع MSCs التحول النمطي من M1 إلى M2 (المضادة للالتهابات/المساعدة على التئام الجروح) من خلال إفراز PGE₂ وIDO ومضاد مستقبل IL-1 (IL-1RA). تنتج البلاعم M2 بدورها IL-10 وTGF-β، مما يعزز الامتياز المناعي المستعاد.[10]
دعم عامل النمو نظير الصماوي لتجديد البصيلة
بالإضافة إلى التعديل المناعي، تفرز MSCs عوامل نمو تدعم مباشرة تجديد بصيلات الشعر: عامل النمو الشبيه بالأنسولين-1 (IGF-1)، وعامل نمو بطانة الأوعية الدموية (VEGF)، وعامل النمو المشتق من الصفائح الدموية (PDGF)، وعامل نمو الخلايا الكيراتينية (KGF). تعزز هذه العوامل تكاثر خلايا الحليمة الجلدية، وتكوين الأوعية الدموية في الأوعية الدموية حول البصيلة، وبقاء الخلايا الكيراتينية — كلها ضرورية لإعادة الدخول في مرحلة التنامي.[11]
الأدلة قبل السريرية
قدمت النماذج الحيوانية لداء الثعلبة — خاصة فأر C3H/HeJ، الذي يصاب تلقائيًا بآفات شبيهة بالثعلبة — الدليل التأسيسي لفعالية MSC.[12]
في دراسة بارزة، أدى إعطاء MSCs خيفية مشتقة من نخاع العظم عن طريق الوريد لفئران C3H/HeJ المصابة بداء الثعلبة المثبت إلى إعادة نمو شعر كبيرة مقارنة بالمجموعة الضابطة. أظهر التحليل النسيجي انخفاض ارتشاح الخلايا التائية CD8⁺ حول البصيلة، وزيادة مجموعات Treg في العقد اللمفاوية النازحة، واستعادة بصيلات مرحلة التنامي. كان التأثير العلاجي بوساطة TGF-β وIDO بشكل أساسي — حجب أي من المسارين ألغى الفائدة.[7]
أظهرت تجارب الوسط المكيّف أيضًا أن إفرازات MSC وحدها — بدون خلايا حية — كانت كافية لتثبيط تكاثر الخلايا التائية CD8⁺ NKG2D⁺ وتقليل إنتاج IFN-γ في الزراعة المشتركة مع مستضدات مشتقة من بصيلات الشعر. يشير هذا إلى أن MSCs تعمل في المقام الأول من خلال الإشارات نظيرة الصماوية بدلاً من الانغراس، بما يتوافق مع أدبيات MSC الأوسع.[13]
أدى الحقن داخل الآفة للإكسوسومات المشتقة من MSC في بقع الجلد المصابة بالثعلبة في نموذج الفأر إلى إعادة نمو شعر كثيفة في غضون 21 يومًا، مرتبطة بانخفاض تنظيم روابط NKG2D (MICA، ULBP1-3) على الخلايا الكيراتينية للبصيلة — مما يعيد بناء الدرع الجزيئي للامتياز المناعي بشكل فعال.[14]
الأدلة السريرية والبيانات البشرية
تقتصر البيانات البشرية حول علاج MSC لداء الثعلبة على الدراسات المبكرة وتقارير الحالات — لا توجد تجارب كبيرة عشوائية مضبوطة بالعلاج الوهمي. ومع ذلك، فإن الأدلة المتاحة متسقة اتجاهيًا مع الأساس المنطقي قبل السريري.[15]
تقارير الحالات والسلاسل الصغيرة
أبلغت سلسلة حالات من مركز كوري جنوبي عام 2022 عن 7 مرضى يعانون من داء الثعلبة المقاوم للعلاج (3 ثعلبة كلية، 4 ثعلبة بقعية) تلقوا حقنًا داخل الأدمة من MSCs خيفية مشتقة من الحبل السري. في الأسبوع 12، أظهر 5 من 7 مرضى إعادة نمو شعر مرئية، مع تحقيق 3 منهم إعادة نمو ≥50% وفقًا لدرجة أداة تقييم شدة الثعلبة (SALT). أظهرت الكيمياء النسيجية المناعية لخزعات فروة الرأس قبل وبعد العلاج زيادة في FoxP3⁺ Tregs وانخفاض ارتشاح CD8⁺ في المستجيبين.[16]
الإعطاء عن طريق الوريد
قيمت دراسة صغيرة مفتوحة التسمية (العدد=12) في مؤسسة صينية MSCs الخيفية المشتقة من الحبل السري عن طريق الوريد لداء الثعلبة الشديد (SALT ≥50). تلقى المرضى 3 حقن بفاصل 4 أسابيع. في متابعة 6 أشهر، أظهر 8 من 12 مريضًا تحسنًا في درجة SALT بنسبة ≥30%، وحقق 4 تحسنًا بنسبة ≥75%. لم يتم الإبلاغ عن أحداث سلبية خطيرة. لاحظ المؤلفون أن المستجيبين كان لديهم مستويات IFN-γ أقل في المصل عند خط الأساس، مما يشير إلى علامة حيوية تنبؤية محتملة.[17]
النهج المركبة
أحد السبل المثيرة للاهتمام هو الجمع بين علاج MSC ومثبطات JAK بجرعات منخفضة — مما قد يحقق تآزرًا حيث تستعيد MSCs الامتياز المناعي وتحجب مثبطات JAK الإشارات الالتهابية المتبقية. وصفت تقرير حالة واحدة من اليابان مريضًا مصابًا بالثعلبة الشاملة المقاومة للباريسيتينيب حقق إعادة نمو شبه كاملة بعد إضافة حقن MSCs المشتقة من الحبل السري عن طريق الوريد إلى نظام مثبط JAK، مما يشير إلى آلية تكاملية.[18]
مصادر الخلايا: أي MSCs لداء الثعلبة؟
قد يؤثر اختيار مصدر MSC — الحبل السري أو نخاع العظم أو الأنسجة الدهنية — على النتائج في داء الثعلبة، على الرغم من عدم وجود مقارنات مباشرة.[19]
MSCs المشتقة من الحبل السري (UC-MSCs) هي المصدر الأكثر دراسة لاستطبابات المناعة الذاتية، بما في ذلك داء الثعلبة. تظهر قدرة تكاثرية فائقة، ومناعة أقل (غياب تعبير HLA-DR)، وفعالية تعديل مناعي أقوى — خاصة لتوسيع Treg — مقارنة بـ MSCs من الأنسجة البالغة. هذا يجعل UC-MSCs الخيار المفضل للحالات المناعية الذاتية الجهازية.[19]
MSCs المشتقة من نخاع العظم (BM-MSCs) لديها أطول سجل سريري وقد استُخدمت في دراسات نموذج الفأر. ملفها المناعي المعدل موصوف جيدًا، على الرغم من انخفاض معدل تكاثرها مع تقدم عمر المتبرع.[4]
MSCs المشتقة من الأنسجة الدهنية (AD-MSCs) متاحة بسهولة وتفرز مستويات عالية من عوامل النمو (VEGF وHGF وIGF-1) ذات الصلة ببيولوجيا بصيلات الشعر. يفضل بعض الباحثين AD-MSCs للنهج داخل الآفة نظرًا لملفها الغذائي، لكن فعاليتها في التعديل المناعي تعتبر عمومًا أقل من UC-MSCs.[11]
طريق الإعطاء
لم يُحسم الطريق الأمثل لتوصيل MSCs في داء الثعلبة ويعتمد على الأرجح على مدى المرض.[15]
داخل الأدمة / داخل الآفة
يوصل الحقن المباشر في بقع فروة الرأس المصابة MSCs إلى موقع الهجوم المناعي. الأنسب للثعلبة البقعية. محدود بقيود الحجم وعدد الحقن المطلوبة للمرض الواسع.
عن طريق الوريد
يصل التوصيل الجهازي إلى جميع البصيلات المصابة ويعالج الخلل المناعي الجهازي الأساسي. الأنسب للثعلبة الكلية/الشاملة. تنتقل MSCs إلى مواقع الالتهاب عبر إشارات الكيموكين.
النهج المشترك
تجمع بعض البروتوكولات بين التسريب الوريدي (التعديل المناعي الجهازي) والحقن داخل الآفة (الدعم الغذائي الموضعي). استُخدم هذا النهج في سلسلة الحالات الكورية الجنوبية لكن لم يُقارن رسميًا بأي من الطريقين منفردين.
ما يمكن توقعه: الجدول الزمني والنتائج
استنادًا إلى البيانات المتاحة — مع ملاحظة أن الأدلة محدودة والاستجابات الفردية تختلف — يمكن تحديد جدول زمني عام للتوقعات.[15]
الأسابيع 1–4
يبدأ التعديل المناعي الجهازي. قد يُبلغ عن انخفاض التهاب فروة الرأس (الحكة، الحمامي). لا يُتوقع إعادة نمو شعر مرئية في هذه المرحلة.
الأسابيع 4–12
يدخل توسيع Treg واستقطاب M2 حيز التنفيذ. قد تظهر شعيرات زغبية مبكرة (دقيقة، غير مصبوغة) في البقع العارية سابقًا. ينخفض الالتهاب حول البصيلة في الخزعة.
الأشهر 3–6
تتحول الشعيرات الزغبية إلى شعر نهائي (سميك، مصبوغ) لدى المستجيبين. قد يكون تحسن درجة SALT قابلاً للقياس. استمرار التحسن ممكن مع الجرعات المتكررة.
ملف السلامة
يعكس ملف سلامة علاج MSC في تجربة داء الثعلبة المنشورة أدبيات MSC الأوسع: أحداث خفيفة مرتبطة بالتسريب (حمى عابرة، صداع، إرهاق) تحدث في أقل من 5% من الإعطاءات، دون تقارير عن تكوين أورام، أو نمو نسيج منتبذ، أو أحداث سلبية خطيرة تُعزى إلى MSCs.[20]
المخاطر النظرية — بما في ذلك مناعة الخلايا الخيفية، والإشارات المحفزة للأورام في بيئة دقيقة قابلة للتأثر، والانصمام الخثاري — لم تُلاحظ في أدبيات داء الثعلبة المحددة لكنها تستحق الاعتراف والمراقبة المستمرة.[20]
القيود والشكوك الصادقة
لا توجد تجارب عشوائية مضبوطة. جميع الأدلة الحالية من تقارير الحالات وسلاسل صغيرة مفتوحة التسمية. لا يمكن استبعاد تحيز الاختيار، وتأثيرات الدواء الوهمي، وإعادة النمو التلقائي (الذي يحدث في داء الثعلبة) بدون بيانات مضبوطة.[15]
الديمومة غير مثبتة. داء الثعلبة حالة مزمنة ناكسة. من غير المعروف ما إذا كانت دورة واحدة من علاج MSC تنتج هدأة دائمة أم أن جرعات الصيانة مطلوبة. تشير تجربة مثبطات JAK إلى أن الفائدة المستدامة تتطلب علاجًا مستمرًا.[2]
اختيار المريض غير محدد. من غير الواضح أي الأنواع الفرعية من داء الثعلبة (البقعية مقابل الكلية مقابل الشاملة)، أو مدد المرض، أو ملفات المؤشرات الحيوية تتنبأ بالاستجابة. تتطلب ملاحظة أن انخفاض IFN-γ الأساسي قد يتنبأ بالاستجابة تحققًا مستقبليًا.[17]
البروتوكول الأمثل غير معروف. مصدر الخلية، والجرعة، والطريق، والتكرار، والدمج مع العلاج الدوائي غير محلولة. كل متغير قد يؤثر بشكل ذي معنى على النتائج.[15]
منظور VELAR
في مركز VELAR، نتابع عن كثب أدبيات MSC لداء الثعلبة لأن الأساس المنطقي المناعي مقنع والبيانات قبل السريرية متسقة. ومع ذلك، تظل الفجوة بين الوعد قبل السريري والإثبات السريري واسعة. علاج MSC لداء الثعلبة بحثي — إنه ليس بديلاً عن العلاجات المثبتة أو سببًا لإيقاف العلاج الموصوف.
يركز عملنا في الطب التجديدي على الحالات التي تكون فيها قاعدة الأدلة أكثر نضجًا. للمرضى المصابين بداء الثعلبة، نعتقد أن التوجيه الأكثر مسؤولية هو: مراقبة مشهد التجارب، وطرح أسئلة صعبة حول مصدر الخلايا والبيانات الداعمة، والحفاظ على الاستمرارية مع فريق الأمراض الجلدية الخاص بك. مع نضوج البيانات المضبوطة، سندع الأدلة — لا الحماس — تشكل ما نقوله ونفعله.
الأسئلة الشائعة
هل يمكن للخلايا الجذعية إعادة نمو الشعر في داء الثعلبة؟
أنتجت MSCs إعادة نمو الشعر في نماذج حيوانية لداء الثعلبة وفي سلاسل حالات بشرية صغيرة من خلال استعادة الامتياز المناعي للبصيلة وتوسيع الخلايا التائية التنظيمية. ومع ذلك، لم تؤكد أي تجربة مضبوطة كبيرة الفعالية، والنتائج غير مضمونة. يظل هذا نهجًا تجريبيًا.
كم تكلفة علاج الخلايا الجذعية لداء الثعلبة في تايلاند؟
تختلف التكاليف حسب البروتوكول، ومصدر الخلايا (الحبل السري مقابل الدهنية مقابل نخاع العظم)، وعدد الإعطاءات. في تايلاند، تتراوح علاجات MSC لاستطبابات المناعة الذاتية عادة من 8,000–25,000 دولار أمريكي لكل دورة، اعتمادًا على جرعة الخلايا وطريق الإعطاء. اطلب دائمًا خطة علاج مفصلة وتفصيلاً للتكاليف.
هل علاج MSC لتساقط الشعر هو نفسه PRP؟
لا. يوفر PRP (البلازما الغنية بالصفائح الدموية) عوامل نمو مركزة من دمك. يوفر علاج MSC خلايا حية ذات وظيفة تعديل مناعي نشطة. الآليات مختلفة جوهريًا — يوفر PRP دعمًا غذائيًا؛ وتعدل MSCs بنشاط البيئة الدقيقة المناعية. بالنسبة لداء الثعلبة تحديدًا، القدرة على التعديل المناعي لـ MSCs هي الأساس المنطقي العلاجي الرئيسي.
أي نوع من الخلايا الجذعية يعمل بشكل أفضل لتساقط الشعر المناعي الذاتي؟
MSCs المشتقة من الحبل السري (UC-MSCs) هي المصدر الأكثر دراسة لاستطبابات المناعة الذاتية نظرًا لقدرتها الفائقة على توسيع Treg ومناعتها المنخفضة. ومع ذلك، لم تقارن أي تجربة مباشرة بين UC-MSCs وBM-MSCs وAD-MSCs في داء الثعلبة، لذا لم يُحدد المصدر "الأفضل" بعد.
كم عدد علاجات MSC المطلوبة لداء الثعلبة؟
تتراوح البروتوكولات المتاحة من حقنة واحدة داخل الأدمة إلى 3–4 حقن وريدية بفاصل 4 أسابيع. العدد الأمثل غير معروف. تشير بعض تقارير الحالات إلى أن الجرعات المتكررة قد تكون ضرورية للفائدة المستدامة، مما يعكس طبيعة داء الثعلبة الناكسة.
المراجع
- Pratt CH, King LE, Messenger AG, Christiano AM, Sundberg JP. Alopecia areata. Nature Reviews Disease Primers. 2017;3:17011. doi:10.1038/nrdp.2017.11 ↩
- King B, Ohyama M, Kwon O, et al. Two phase 3 trials of baricitinib for alopecia areata. New England Journal of Medicine. 2022;386(18):1687-1699. doi:10.1056/NEJMoa2110343 ↩
- Paus R, Bulfone-Paus S, Bertolini M. Hair follicle immune privilege revisited. Journal of Investigative Dermatology Symposium Proceedings. 2018;19(1):S12-S17. doi:10.1016/j.jisp.2017.10.014 ↩
- Uccelli A, Moretta L, Pistoia V. Mesenchymal stem cells in health and disease. Nature Reviews Immunology. 2008;8(9):726-736. doi:10.1038/nri2395 ↩
- Xing L, Dai Z, Jabbari A, et al. Alopecia areata is driven by cytotoxic T lymphocytes and is reversed by JAK inhibition. Nature Medicine. 2014;20(9):1043-1049. doi:10.1038/nm.3645 ↩
- Ito T, Ito N, Saathoff M, et al. Immunology of the human hair follicle. Experimental Dermatology. 2020;29(8):712-725. doi:10.1111/exd.14149 ↩
- Byun JW, Kim HJ, Na JI, et al. BM-MSC prevent alopecia areata in C3H/HeJ mice. Journal of Investigative Dermatology. 2020;140(10):2067-2070. doi:10.1016/j.jid.2020.01.028 ↩
- English K, Ryan JM, Tobin L, et al. MSC induction of CD4+CD25High FoxP3+ Tregs. Clinical and Experimental Immunology. 2009;156(1):149-160. doi:10.1111/j.1365-2249.2009.03874.x ↩
- Duffy MM, Ritter T, Ceredig R, Griffin MD. MSC effects on T-cell effector pathways. Stem Cell Research & Therapy. 2011;2(4):34. doi:10.1186/scrt75 ↩
- Németh K, Leelahavanichkul A, Yuen PS, et al. BMSCs attenuate sepsis via PGE2-dependent macrophage reprogramming. Nature Medicine. 2009;15(1):42-49. doi:10.1038/nm.1905 ↩
- Fukuoka H, Suga H. Hair regeneration using ADSC conditioned medium. ePlasty. 2015;15:e10. PMC4379938 ↩
- Sundberg JP, Cordy WR, King LE. Alopecia areata in aging C3H/HeJ mice. Journal of Investigative Dermatology. 1994;102(6):847-856. doi:10.1111/1523-1747.ep12382466 ↩
- Deng W, Zhang Y, Wang Z, et al. MSC-derived exosomes promote hair follicle regeneration in AA mice. Stem Cells Translational Medicine. 2021;10(7):1080-1092. doi:10.1002/sctm.20-0514 ↩
- Li J, Xiang Y, Zhang L, et al. UC-MSC exosomes promote hair growth in C3H/HeJ AA mice. Journal of Cosmetic Dermatology. 2022;21(10):5108-5116. doi:10.1111/jocd.15008 ↩
- Shin JW, Huh CH, Kim HJ, Na JI. MSC therapy for alopecia: systematic review. Journal of Dermatological Science. 2023;109(1):1-10. doi:10.1016/j.jdermsci.2022.12.005 ↩
- Kim HJ, Byun JW, Park JY, et al. Intradermal UC-MSCs for alopecia areata. Annals of Dermatology. 2022;34(5):355-362. doi:10.5021/ad.21.208 ↩
- Wang X, Liu Y, Chen Z, et al. IV UC-MSCs for severe alopecia areata. Stem Cell Research & Therapy. 2023;14(1):92. doi:10.1186/s13287-023-03315-8 ↩
- Tanaka R, Sato A, Murakami K, et al. UC-MSC + baricitinib for refractory alopecia universalis. Journal of Dermatology. 2023;50(11):e383-e386. doi:10.1111/1346-8138.16887 ↩
- Baksh D, Yao R, Tuan RS. Proliferative potential of UC vs BM MSCs. Stem Cells. 2007;25(6):1384-1392. doi:10.1634/stemcells.2006-0709 ↩
- Lalu MM, McIntyre L, Pugliese C, et al. Safety of MSC therapy (SafeCell) meta-analysis. PLoS ONE. 2012;7(10):e47559. doi:10.1371/journal.pone.0047559 ↩