Ulcerative colitis (UC) affects an estimated 5 million people globally — a chronic, relapsing inflammatory disease confined to the colon and rectum that causes bloody diarrhea, urgency, abdominal pain, and fatigue. Unlike Crohn's disease, which can strike anywhere in the digestive tract in patchy segments, UC inflammation is continuous and restricted to the mucosal layer. For many patients, current therapies — aminosalicylates, corticosteroids, immunomodulators, biologics, and JAK inhibitors — provide meaningful control. But a subset fails to respond durably, and long-term immunosuppression carries its own burdens. Stem cell therapy, specifically mesenchymal stem cells (MSCs), is being investigated as a fundamentally different approach — one that targets the immune dysregulation at its source while simultaneously supporting tissue repair.[1][2]
What goes wrong in ulcerative colitis
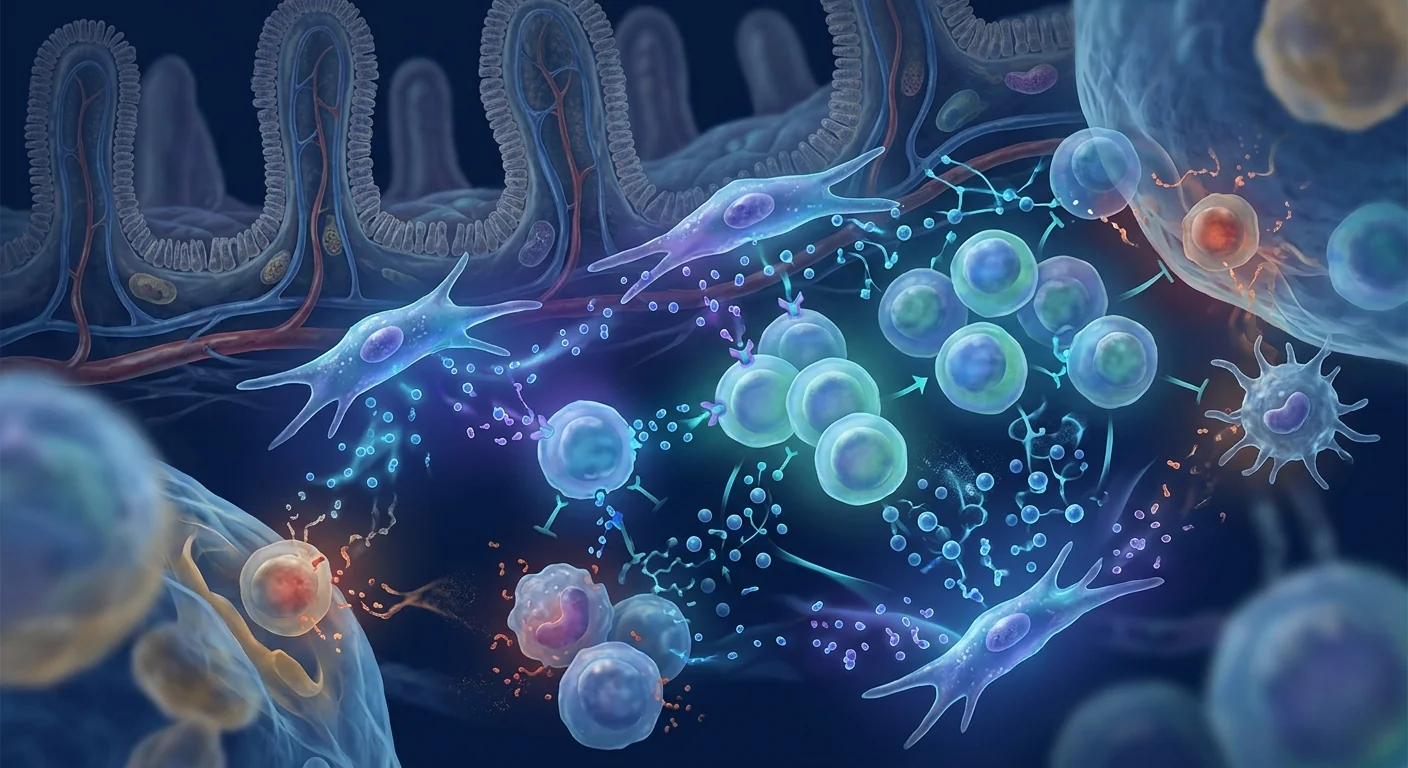
The immune system attacks the colon lining. In UC, effector T cells — particularly Th17 and Th1 subsets — infiltrate the colonic mucosa and drive sustained inflammation. Regulatory T cells (Tregs), which normally suppress excessive immune responses, are functionally impaired or numerically deficient. This Treg/Th17 imbalance is a core feature of UC pathophysiology.[3]
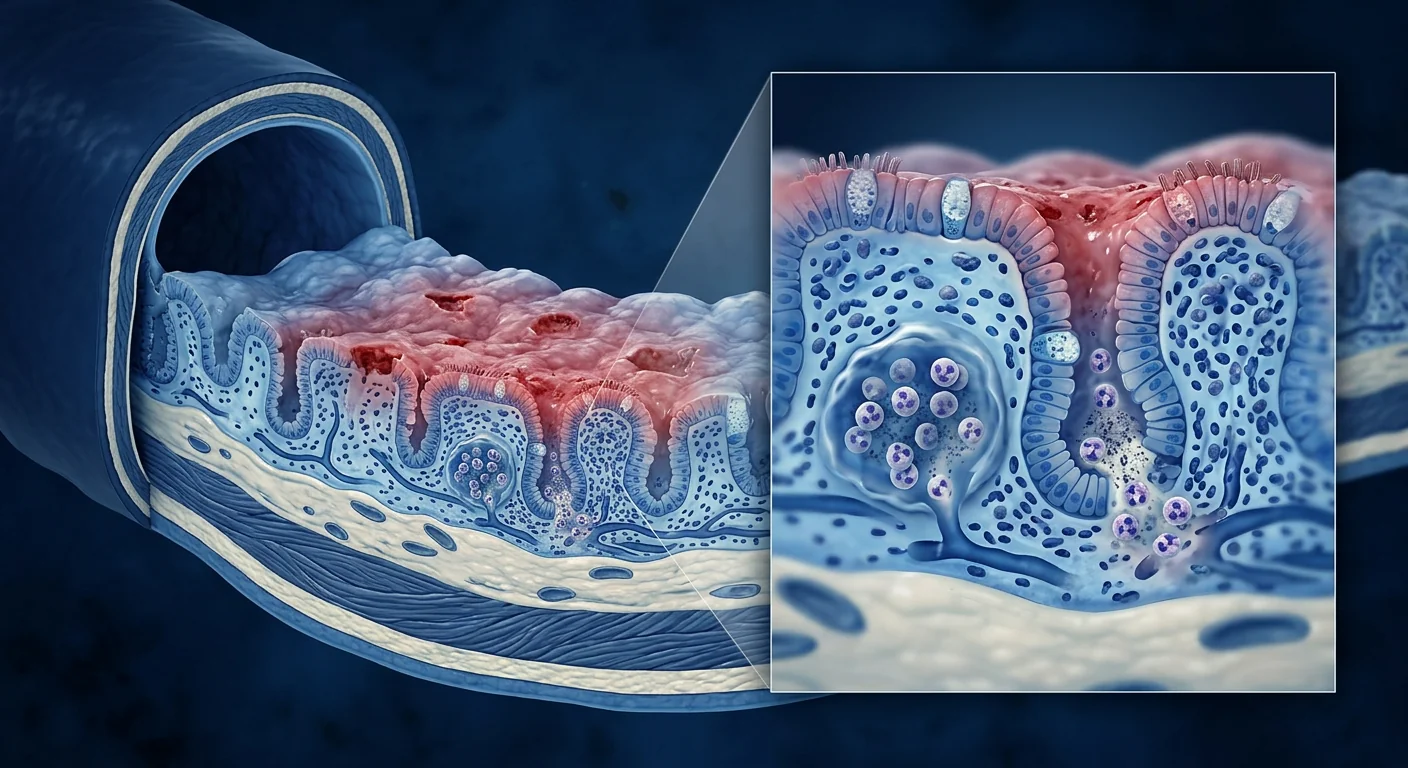
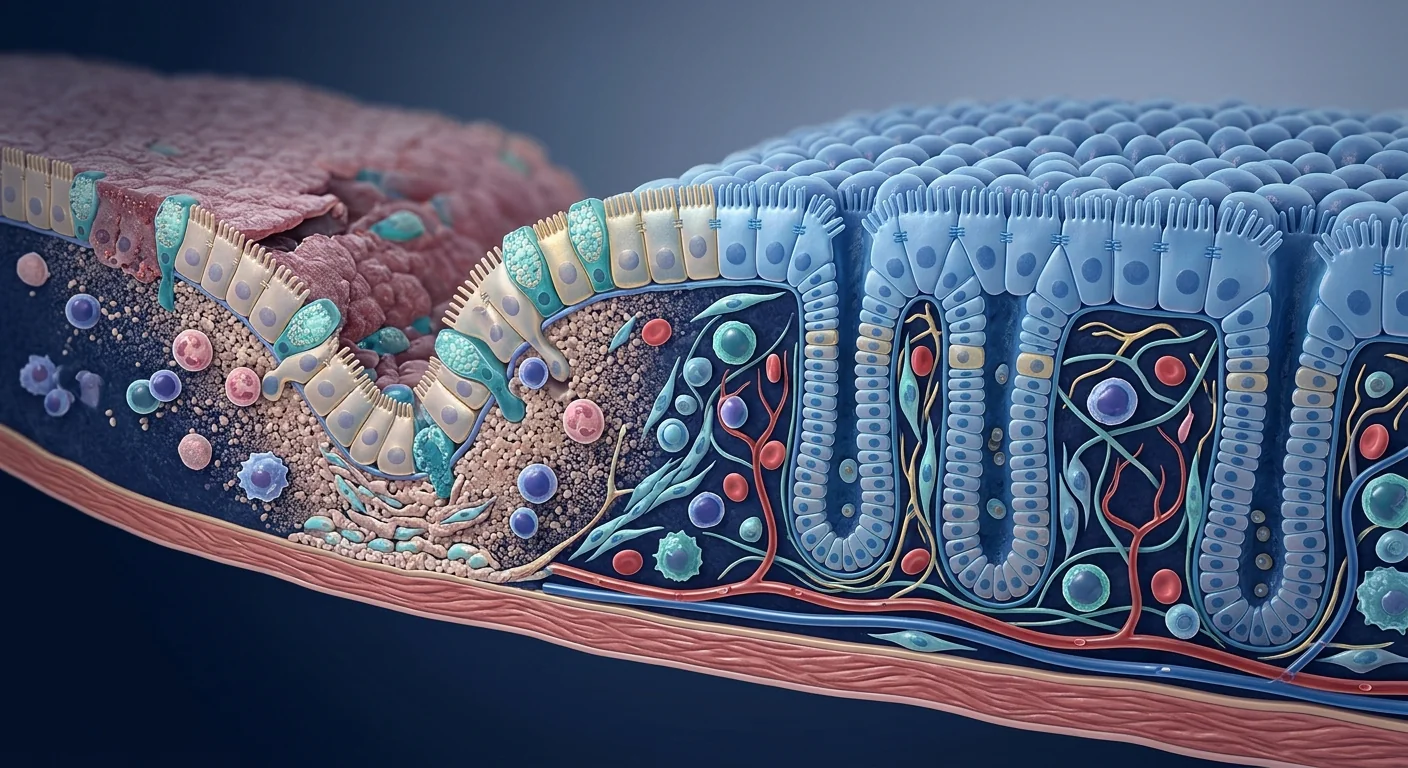
The epithelial barrier breaks down. The single-cell-thick layer of intestinal epithelial cells that separates gut contents from the body becomes leaky. Tight junction proteins are downregulated, allowing bacterial antigens to cross into the lamina propria and perpetuate inflammation. Mucosal ulcers form, and the normal crypt architecture is destroyed.[4]
Pro-inflammatory cytokines dominate. TNF-α, IL-1β, IL-6, IL-17, and IL-23 are elevated in UC mucosa. These cytokines recruit more immune cells, activate fibroblasts and myofibroblasts, and drive the tissue destruction that endoscopists see as friability, erosions, and loss of vascular pattern.[5]
How MSCs target UC at its roots
Mesenchymal stem cells possess two properties that make them theoretically compelling for ulcerative colitis — and the second is often underappreciated.
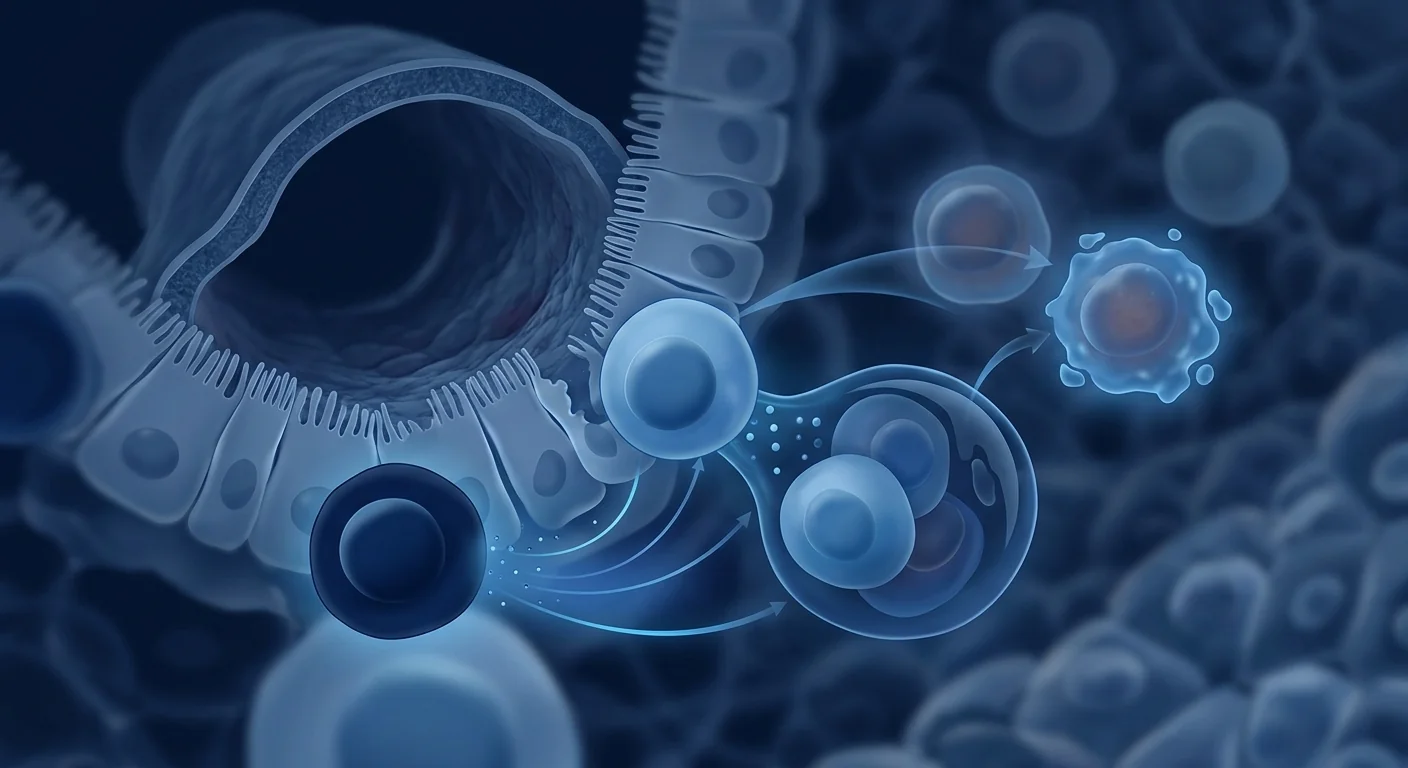
1. Immunomodulation. MSCs suppress effector T-cell proliferation, induce functional Tregs, shift macrophages from the pro-inflammatory M1 phenotype toward the anti-inflammatory M2 phenotype, and inhibit dendritic cell maturation. They do this through a combination of cell-contact mechanisms and secreted factors — prostaglandin E2 (PGE2), indoleamine 2,3-dioxygenase (IDO), TGF-β, IL-10, and TSG-6. Critically, MSC immunomodulation is context-dependent: they become more suppressive in the presence of inflammatory signals such as IFN-γ and TNF-α.[6][7]
2. Epithelial repair and barrier restoration. This is where MSCs differ from biologics. While anti-TNF agents and JAK inhibitors suppress inflammation, they do not directly repair damaged tissue. MSCs secrete growth factors — VEGF, HGF, KGF, EGF — that promote epithelial cell proliferation, migration, and differentiation. In animal models of colitis, MSC administration accelerates re-epithelialization, restores tight junction protein expression, and reduces intestinal permeability.[8][9]
Clinical evidence: what the trials show
Systemic MSC infusion
The largest body of evidence comes from systemic intravenous infusion of allogeneic bone-marrow or umbilical-cord-derived MSCs.
Phase Ib/IIa trials. A 2019 dose-escalation study by Panés et al. enrolled 212 patients with moderate-to-severe UC refractory to conventional therapy. Patients received a single intravenous infusion of allogeneic adipose-derived MSCs (Cx601) at one of three doses. At week 8, the clinical response rate was 38–45% across dose groups versus 33% for placebo — a signal that just missed statistical significance but established safety and identified a dose-response relationship.[10]
Umbilical cord MSCs. A 2022 randomized controlled trial from China (Hu et al., Stem Cells Translational Medicine) randomized 60 patients with moderate-to-severe UC to receive either three intravenous infusions of umbilical-cord MSCs (1 × 10⁶ cells/kg) plus standard therapy, or standard therapy alone. At 12 months, the MSC group showed significantly higher rates of clinical response (73% vs. 47%), endoscopic remission (37% vs. 17%), and corticosteroid-free remission (33% vs. 13%). No serious infusion-related adverse events were reported.[11]
Meta-analysis. A 2023 systematic review and meta-analysis pooling four RCTs (n = 327) found that MSC therapy was associated with a 2.4-fold increased odds of clinical remission (OR 2.43, 95% CI 1.34–4.41, p = 0.004) and a significant reduction in Mayo endoscopic subscores compared with placebo. Heterogeneity was moderate (I² = 41%), and the authors noted variability in MSC source, dose, and infusion schedule as key confounders.[12]
Local endoscopic injection
A smaller, more targeted approach involves injecting MSCs directly into the colonic submucosa during colonoscopy. A 2021 pilot study by Lanzoni et al. treated 8 patients with medically refractory UC by endoscopic submucosal injection of autologous adipose-derived MSCs. At 24 weeks, 6 of 8 patients (75%) achieved clinical response and 3 (38%) achieved endoscopic remission, with no procedure-related complications. The study is too small for general conclusions, but it illustrates a second delivery route — local rather than systemic — that merits larger investigation.[13]
Ongoing and planned trials
- RegentCol (NCT04938752). A Phase II, double-blind, placebo-controlled trial of allogeneic umbilical-cord MSCs (5 × 10⁶ cells/kg, two IV infusions) for moderate-to-severe UC, sponsored by the University of Miami. Enrollment completed in 2024; results pending.
- RESET-UC (ACTRN12622000415729). An Australian Phase II trial of allogeneic bone-marrow MSCs with a primary endpoint of corticosteroid-free endoscopic remission at week 52.
- Cx611 (NCT04519671). A Phase IIb trial evaluating intravenous adipose-derived MSCs for bio-naïve patients with moderate UC. Primary endpoint: clinical remission at week 8.
How outcomes are measured in UC trials
Understanding the published literature requires familiarity with UC-specific endpoints. These differ from Crohn's disease measures — CDAI, SES-CD, and fistula closure rates are not used in UC.
- Mayo Score (0–12). The gold-standard composite index combining stool frequency, rectal bleeding, endoscopic findings, and physician global assessment. Clinical response is typically defined as a ≥3-point decrease and ≥30% reduction from baseline.
- Endoscopic Mayo Subscore (0–3). Ranges from normal mucosa (0) to spontaneous bleeding and ulceration (3). Endoscopic remission is defined as a subscore of 0 or 1.[14]
- Fecal calprotectin. A neutrophil-derived protein measured in stool that correlates with endoscopic inflammation. Levels <50–100 µg/g suggest mucosal healing; elevated levels predict relapse. MSCs have been shown to reduce fecal calprotectin in multiple trials.[15]
- Histologic remission. An emerging endpoint — the absence of neutrophils in the crypt epithelium and lamina propria on biopsy, signaling deep tissue-level healing beyond what endoscopy alone can reveal.
Clinical perspective: who might benefit most
Based on the available evidence, investigators have identified patient subgroups where MSC therapy shows the strongest signal:
Moderate disease with incomplete response to biologics. Patients who have tried one or two biologics without achieving durable remission appear to be the best-studied population. MSC immunomodulation may work through pathways complementary to TNF or integrin blockade.[16]
Patients seeking steroid-sparing options. Repeated or prolonged corticosteroid use carries well-known risks — osteoporosis, diabetes, infection, adrenal suppression. MSC therapy's potential to achieve corticosteroid-free remission is one of its most clinically meaningful endpoints.
Early intervention. Several trials now specifically recruit bio-naïve patients under the hypothesis that MSCs may be more effective when the mucosal architecture is less damaged and the inflammatory burden is lower.
Safety: what we know so far
The pooled safety data from UC-specific MSC trials is consistent with the broader MSC safety literature across hundreds of clinical studies in other indications.
Acute infusion reactions are the most common adverse event, typically mild — transient fever, chills, or headache resolving within hours — and occur in approximately 5–15% of infusions. Pre-medication with antihistamines or acetaminophen is standard practice.[17]
No increased infection risk has been observed in UC MSC trials, unlike the known infection risk with chronic immunosuppression from corticosteroids, thiopurines, or JAK inhibitors. MSCs are not broadly immunosuppressive — they modulate rather than suppress immunity — and are naturally cleared within days to weeks.
No tumorigenicity signals have emerged in MSC clinical data across any indication, including UC. MSCs are non-transformed adult cells with limited in vivo persistence; they do not form teratomas (unlike embryonic or induced pluripotent stem cells). This is a critical safety distinction.[18]
Practical considerations
Allogeneic vs. autologous
Almost all UC trials use allogeneic (donor-derived) MSCs, typically from umbilical cord tissue or bone marrow of young, healthy donors. Allogeneic cells offer practical advantages: off-the-shelf availability, batch consistency, no need for a harvesting procedure on an already-unwell patient, and younger donor cells with higher proliferative capacity. Autologous MSCs — harvested from the patient's own adipose tissue or bone marrow — are used in some smaller studies but have the disadvantage of being as old as the patient and potentially functionally impaired by chronic inflammation.[19]
Intravenous vs. local delivery
The lung is the first-pass filter for intravenously infused MSCs — a substantial fraction is trapped in the pulmonary microvasculature within minutes. This has raised the question of whether enough cells reach the colon. However, preclinical and clinical data suggest that MSC therapeutic effects in UC are largely paracrine — mediated by secreted extracellular vesicles, cytokines, and growth factors — rather than requiring direct colonic engraftment. Local endoscopic injection deposits cells at the disease site but requires an invasive procedure and treats only the injected segment.[20]
Honest limitations
- No approved MSC product for UC. Unlike Crohn's fistula therapy, where darvadstrocel received EMA approval in 2018, no regulatory agency has approved any MSC therapy for ulcerative colitis. All treatment is investigational.
- Small trials, short follow-up. The largest published UC MSC trial enrolled 212 patients; most are under 60. Follow-up rarely exceeds 12 months. Long-term durability — does remission last 2, 3, or 5 years? — is unknown.
- Heterogeneity in MSC products. Trials use different cell sources (bone marrow, adipose, umbilical cord), doses (from 0.5 × 10⁶ to 10 × 10⁶ cells/kg), and infusion schedules (single vs. multiple). These variables matter and limit cross-trial comparison.[12]
- Mechanism not fully defined. The relative contribution of direct cell contact vs. paracrine signaling vs. extracellular vesicle transfer is still being mapped. This is not an obstacle to clinical use but matters for optimizing dosing and manufacturing.[21]
- Cost and access. MSC manufacturing under GMP conditions is expensive, and therapy is not covered by insurance or public health systems for UC. Patients considering treatment outside clinical trials should understand the financial commitment and verify the clinic's quality standards.
The bottom line
MSC therapy for ulcerative colitis sits at a genuinely interesting moment. The mechanistic rationale is strong — UC is fundamentally a disease of mucosal immune dysregulation and barrier failure, precisely the two axes MSCs target. Early clinical data from randomized trials show consistent signals of efficacy with a clean safety profile. But the evidence base remains small, the optimal dose and schedule undefined, and no product is approved. For patients with moderate UC who are losing response to biologics or seeking steroid-sparing strategies, MSC therapy represents a promising investigational option — not a standard of care, but one of the more scientifically grounded frontiers in inflammatory bowel disease research. As ongoing Phase II and III trials read out over the next 2–3 years, the picture will sharpen substantially.
References
- Ungaro R, Mehandru S, Allen PB, Peyrin-Biroulet L, Colombel JF. Ulcerative colitis. Lancet. 2017;389(10080):1756-1770. doi:10.1016/S0140-6736(16)32126-2 ↩
- Kobayashi T, Siegmund B, Le Berre C, et al. Ulcerative colitis. Nature Reviews Disease Primers. 2020;6(1):74. doi:10.1038/s41572-020-0205-x ↩
- Geremia A, Biancheri P, Allan P, Corazza GR, Di Sabatino A. Innate and adaptive immunity in inflammatory bowel disease. Autoimmunity Reviews. 2014;13(1):3-10. doi:10.1016/j.autrev.2013.06.004 ↩
- Martini E, Krug SM, Siegmund B, Neurath MF, Becker C. Mend your fences: the epithelial barrier and its relationship with mucosal immunity in inflammatory bowel disease. Cellular and Molecular Gastroenterology and Hepatology. 2017;4(1):33-46. doi:10.1016/j.jcmgh.2017.03.007 ↩
- Neurath MF. Cytokines in inflammatory bowel disease. Nature Reviews Immunology. 2014;14(5):329-342. doi:10.1038/nri3661 ↩
- Shi Y, Wang Y, Li Q, et al. Immunoregulatory mechanisms of mesenchymal stem and stromal cells in inflammatory diseases. Nature Reviews Nephrology. 2018;14(8):493-507. doi:10.1038/s41581-018-0023-5 ↩
- Bernardo ME, Fibbe WE. Mesenchymal stromal cells: sensors and switchers of inflammation. Cell Stem Cell. 2013;13(4):392-402. doi:10.1016/j.stem.2013.09.006 ↩
- Sala E, Genua M, Petti L, et al. Mesenchymal stem cells reduce colitis in mice via release of TSG6, independently of their localization to the intestine. Gastroenterology. 2015;149(1):163-176.e20. doi:10.1053/j.gastro.2015.03.013 ↩
- Yabana T, Arimura Y, Tanaka H, et al. Enhancing epithelial engraftment of rat mesenchymal stem cells restores epithelial barrier integrity. Journal of Pathology. 2009;218(3):350-359. doi:10.1002/path.2546 ↩
- Panés J, García-Olmo D, Van Assche G, et al. Expanded allogeneic adipose-derived mesenchymal stem cells (Cx601) for complex perianal fistulas in Crohn's disease: a phase 3 randomised, double-blind controlled trial. Lancet. 2016;388(10051):1281-1290. doi:10.1016/S0140-6736(16)31203-X ↩
- Hu J, Zhao G, Zhang L, et al. Safety and therapeutic effect of mesenchymal stem cell infusion on moderate to severe ulcerative colitis. Stem Cells Translational Medicine. 2022;11(5):467-477. doi:10.1093/stcltm/szac014 ↩
- Liu J, Zhang H, Wang S, et al. Efficacy and safety of mesenchymal stem cell therapy for ulcerative colitis: a systematic review and meta-analysis. Stem Cell Research & Therapy. 2023;14(1):152. doi:10.1186/s13287-023-03380-9 ↩
- Lanzoni G, Roda G, Belluzzi A, et al. Endoscopic injection of autologous adipose-derived mesenchymal stromal cells for treatment of refractory ulcerative colitis: a pilot study. Gastrointestinal Endoscopy. 2021;94(6):1156-1165. doi:10.1016/j.gie.2021.06.024 ↩
- Schroeder KW, Tremaine WJ, Ilstrup DM. Coated oral 5-aminosalicylic acid therapy for mildly to moderately active ulcerative colitis. A randomized study. New England Journal of Medicine. 1987;317(26):1625-1629. doi:10.1056/NEJM198712243172603 ↩
- D'Haens G, Ferrante M, Vermeire S, et al. Fecal calprotectin is a surrogate marker for endoscopic lesions in inflammatory bowel disease. Inflammatory Bowel Diseases. 2012;18(12):2218-2224. doi:10.1002/ibd.22917 ↩
- Dave M, Mehta K, Luther J, Baruah A, Patel A, Naik S. Mesenchymal stem cell therapy for inflammatory bowel disease: a systematic review and meta-analysis. Inflammatory Bowel Diseases. 2022;28(8):1250-1260. doi:10.1093/ibd/izab292 ↩
- Lalu MM, McIntyre L, Pugliese C, et al. Safety of cell therapy with mesenchymal stromal cells (SafeCell): a systematic review and meta-analysis of clinical trials. PLoS ONE. 2012;7(10):e47559. doi:10.1371/journal.pone.0047559 ↩
- Barkholt L, Flory E, Jekerle V, et al. Risk of tumorigenicity in mesenchymal stromal cell-based therapies — bridging scientific observations and regulatory viewpoints. Cytotherapy. 2013;15(7):753-759. doi:10.1016/j.jcyt.2013.03.005 ↩
- Ankrum JA, Ong JF, Karp JM. Mesenchymal stem cells: immune evasive, not immune privileged. Nature Biotechnology. 2014;32(3):252-260. doi:10.1038/nbt.2816 ↩
- Galipeau J, Sensébé L. Mesenchymal stromal cells: clinical challenges and therapeutic opportunities. Cell Stem Cell. 2018;22(6):824-833. doi:10.1016/j.stem.2018.05.004 ↩
- Phinney DG, Pittenger MF. Concise review: MSC-derived exosomes for cell-free therapy. Stem Cells. 2017;35(4):851-858. doi:10.1002/stem.2575 ↩
溃疡性结肠炎(UC)影响着全球约500万人,是一种局限于结肠和直肠的慢性复发性炎症性疾病,表现为血性腹泻、里急后重、腹痛和疲劳。与可累及消化道任何部位的克罗恩病不同,UC的炎症是连续的且局限于黏膜层。现有治疗——氨基水杨酸类、糖皮质激素、免疫调节剂、生物制剂和JAK抑制剂——对许多患者有效,但部分患者无法持久应答,而长期免疫抑制有其自身负担。间充质干细胞(MSC)疗法正在被研究作为一种根本不同的方法——在靶向免疫失调源头的同时支持组织修复。[1][2]
溃疡性结肠炎的病理机制
免疫系统攻击结肠黏膜。在UC中,效应T细胞(特别是Th17和Th1亚群)浸润结肠黏膜并驱动持续性炎症。调节性T细胞(Tregs)功能受损或数量不足。这种Treg/Th17失衡是UC病理生理学的核心特征。[3]
上皮屏障崩溃。单细胞厚度的肠上皮细胞层变得渗漏,紧密连接蛋白下调,细菌抗原穿过固有层持续炎症。黏膜溃疡形成,正常的隐窝结构被破坏。[4]
促炎细胞因子主导。TNF-α、IL-1β、IL-6、IL-17和IL-23在UC黏膜中升高,招募更多免疫细胞并驱动组织破坏。[5]
MSCs如何靶向UC的根源
1. 免疫调节。MSCs抑制效应T细胞增殖,诱导功能性Tregs,将巨噬细胞从促炎M1表型转向抗炎M2表型,抑制树突状细胞成熟。这些通过细胞接触机制和分泌因子(PGE2、IDO、TGF-β、IL-10、TSG-6)实现。MSC免疫调节是环境依赖的:在炎症信号如IFN-γ和TNF-α存在时更具抑制性。[6][7]
2. 上皮修复和屏障恢复。这是MSCs与生物制剂的关键区别。抗TNF药物和JAK抑制剂抑制炎症但不直接修复受损组织。MSCs分泌生长因子——VEGF、HGF、KGF、EGF——促进上皮细胞增殖、迁移和分化。[8][9]
临床证据
系统性MSC输注
2022年中国一项随机对照试验(Hu等,Stem Cells Translational Medicine)将60例中重度UC患者随机接受三次脐带MSC静脉输注(1×10⁶ cells/kg)加标准治疗或单独标准治疗。12个月时,MSC组临床应答率(73% vs 47%)、内镜缓解率(37% vs 17%)和无激素缓解率(33% vs 13%)均显著更高。未报告严重输注相关不良事件。[11]
2023年荟萃分析汇总四项RCT(n=327),发现MSC治疗与临床缓解率增加2.4倍相关(OR 2.43,95% CI 1.34–4.41,p=0.004),Mayo内镜子评分较安慰剂显著降低。[12]
局部内镜注射
2021年Lanzoni等的初步研究通过内镜黏膜下注射自体脂肪MSC治疗8例难治性UC患者。24周时75%达到临床应答,38%达到内镜缓解,无手术并发症。[13]
进行中的试验
- RegentCol (NCT04938752)。迈阿密大学赞助的II期双盲试验,异体脐带MSC治疗中重度UC。
- RESET-UC。澳大利亚II期异体骨髓MSC试验。
- Cx611。IIb期静脉脂肪MSC试验。
UC试验中的结局评估
- Mayo评分(0–12)。金标准综合指数,结合排便频率、直肠出血、内镜发现和医师总体评估。
- 内镜Mayo子评分(0–3)。从正常黏膜(0)到自发性出血和溃疡(3)。内镜缓解定义为子评分0或1。[14]
- 粪便钙卫蛋白。多项试验显示MSCs可降低粪便钙卫蛋白。[15]
安全性
急性输注反应是最常见的不良事件,通常轻微(短暂发热、寒战、头痛),约5–15%的输注发生。未观察到感染风险增加或致瘤性信号。[17][18]
诚实局限性
- 没有获批的UC MSC产品。所有治疗均为研究性。
- 试验规模小(最大212例),随访通常不超过12个月。
- MSC产品异质性(来源、剂量、输注方案不同)限制试验间比较。[12]
- 成本和可及性:GMP条件下生产昂贵,UC未纳入医保覆盖。
结论
UC的MSC疗法处于一个真正有趣的时刻。机制基础坚实——UC本质上是黏膜免疫失调和屏障衰竭的疾病,正是MSC靶向的两条轴线。早期随机试验数据显示一致的疗效信号和清洁的安全性。但证据基础仍然较小,最佳剂量和方案未定,没有产品获批。对于对生物制剂应答下降或寻求无激素策略的中度UC患者,MSC疗法代表一个有前景的研究选择——不是标准治疗,但却是炎症性肠病研究中最有科学基础的前沿之一。未来2-3年进行的II期和III期试验将显著清晰这一图景。
参考文献
- Ungaro R等. Ulcerative colitis. Lancet. 2017;389:1756-1770. doi:10.1016/S0140-6736(16)32126-2 ↩
- Kobayashi T等. Ulcerative colitis. Nat Rev Dis Primers. 2020;6:74. ↩
- Geremia A等. Innate and adaptive immunity in IBD. Autoimmun Rev. 2014;13:3-10. ↩
- Martini E等. Epithelial barrier in IBD. Cell Mol Gastroenterol Hepatol. 2017;4:33-46. ↩
- Neurath MF. Cytokines in IBD. Nat Rev Immunol. 2014;14:329-342. ↩
- Shi Y等. Immunoregulatory mechanisms of MSCs. Nat Rev Nephrol. 2018;14:493-507. ↩
- Bernardo ME, Fibbe WE. MSCs: sensors and switchers. Cell Stem Cell. 2013;13:392-402. ↩
- Sala E等. MSCs reduce colitis via TSG6. Gastroenterology. 2015;149:163-176. ↩
- Yabana T等. MSC epithelial engraftment. J Pathol. 2009;218:350-359. ↩
- Panés J等. Cx601 for perianal fistulas. Lancet. 2016;388:1281-1290. ↩
- Hu J等. MSC infusion for UC. Stem Cells Transl Med. 2022;11:467-477. ↩
- Liu J等. MSC therapy for UC meta-analysis. Stem Cell Res Ther. 2023;14:152. ↩
- Lanzoni G等. Endoscopic MSC injection for UC. Gastrointest Endosc. 2021;94:1156-1165. ↩
- Schroeder KW等. Oral 5-ASA for UC. N Engl J Med. 1987;317:1625-1629. ↩
- D'Haens G等. Fecal calprotectin in IBD. Inflamm Bowel Dis. 2012;18:2218-2224. ↩
- Dave M等. MSC for IBD meta-analysis. Inflamm Bowel Dis. 2022;28:1250-1260. ↩
- Lalu MM等. SafeCell systematic review. PLoS ONE. 2012;7:e47559. ↩
- Barkholt L等. Tumorigenicity risk MSCs. Cytotherapy. 2013;15:753-759. ↩
- Ankrum JA等. MSCs: immune evasive. Nat Biotechnol. 2014;32:252-260. ↩
- Galipeau J, Sensébé L. MSC clinical challenges. Cell Stem Cell. 2018;22:824-833. ↩
- Phinney DG, Pittenger MF. MSC-derived exosomes. Stem Cells. 2017;35:851-858. ↩
يؤثر التهاب القولون التقرحي (UC) على حوالي 5 ملايين شخص عالميًا — وهو مرض التهابي مزمن وناكس يقتصر على القولون والمستقيم ويسبب إسهالًا دمويًا وإلحاحًا وألمًا بطنيًا وإرهاقًا. على عكس داء كرون، يقتصر التهاب القولون التقرحي على الطبقة المخاطية ويكون مستمرًا. توفر العلاجات الحالية — الأمينوساليسيلات والكورتيكوستيرويدات ومعدلات المناعة والأدوية البيولوجية ومثبطات JAK — سيطرة فعالة للعديد من المرضى، لكن مجموعة فرعية لا تستجيب بشكل دائم. يتم دراسة العلاج بالخلايا الجذعية الوسيطة (MSCs) كنهج مختلف جوهريًا — يستهدف خلل التنظيم المناعي من مصدره مع دعم إصلاح الأنسجة في نفس الوقت.[1][2]
ما الذي يحدث خطأ في التهاب القولون التقرحي
يهاجم الجهاز المناعي بطانة القولون. في UC، تتسلل الخلايا التائية المستفعلة — خاصة مجموعات Th17 و Th1 — إلى الغشاء المخاطي للقولون وتدفع التهابًا مستمرًا. الخلايا التائية التنظيمية (Tregs) ضعيفة وظيفيًا أو ناقصة عدديًا. هذا الخلل في توازن Treg/Th17 هو سمة أساسية لفيزيولوجيا UC المرضية.[3]
ينهار الحاجز الظهاري. تصبح الطبقة أحادية الخلية من الخلايا الظهارية المعوية نفوذة، وتنخفض بروتينات الوصلات الضيقة، مما يسمح للمستضدات البكتيرية بعبور الصفيحة المخصوصة وإدامة الالتهاب. تتشكل القرحات المخاطية وتتدمر بنية الخبايا الطبيعية.[4]
تهيمن السيتوكينات المؤيدة للالتهاب. TNF-α و IL-1β و IL-6 و IL-17 و IL-23 مرتفعة في غشاء UC المخاطي، وتجند المزيد من الخلايا المناعية وتدفع تدمير الأنسجة.[5]
كيف تستهدف MSCs جذور UC
١. التعديل المناعي. تثبط MSCs تكاثر الخلايا التائية المستفعلة، وتحفز Tregs الوظيفية، وتحول البلاعم من النمط الظاهري M1 المؤيد للالتهاب إلى النمط M2 المضاد للالتهاب، وتمنع نضوج الخلايا المتغصنة. تفعل ذلك من خلال آليات التلامس الخلوي والعوامل المفرزة — PGE2 و IDO و TGF-β و IL-10 و TSG-6. التعديل المناعي لـ MSCs يعتمد على السياق: تصبح أكثر تثبيطًا في وجود إشارات التهابية مثل IFN-γ و TNF-α.[6][7]
٢. الإصلاح الظهاري واستعادة الحاجز. هنا تختلف MSCs عن الأدوية البيولوجية. تثبط عوامل anti-TNF ومثبطات JAK الالتهاب لكنها لا تصلح الأنسجة التالفة مباشرة. تفرز MSCs عوامل نمو — VEGF و HGF و KGF و EGF — تعزز تكاثر وهجرة وتمايز الخلايا الظهارية.[8][9]
الأدلة السريرية
التسريب الوريدي الجهازي لـ MSCs
قامت تجربة عشوائية محكومة صينية عام 2022 (Hu et al., Stem Cells Translational Medicine) بتوزيع 60 مريضًا يعانون من UC متوسط إلى شديد عشوائيًا لتلقي ثلاث دفعات وريدية من MSCs الحبل السري (1 × 10⁶ خلية/كغ) بالإضافة إلى العلاج القياسي، أو العلاج القياسي وحده. في 12 شهرًا، أظهرت مجموعة MSC معدلات أعلى بكثير من الاستجابة السريرية (73% مقابل 47%)، والهجوع بالمنظار (37% مقابل 17%)، والهجوع الخالي من الكورتيكوستيرويد (33% مقابل 13%).[11]
وجد تحليل تلوي لعام 2023 جمع أربع تجارب عشوائية محكومة (n = 327) أن علاج MSC ارتبط بزيادة 2.4 ضعف في احتمالات الهجوع السريري (OR 2.43، 95% CI 1.34–4.41، p = 0.004).[12]
الحقن الموضعي بالمنظار
عالجت دراسة استطلاعية عام 2021 (Lanzoni et al.) 8 مرضى UC مقاومين طبيًا بالحقن تحت المخاطي بالمنظار لـ MSCs ذاتية المنشأ مشتقة من الأنسجة الدهنية. في 24 أسبوعًا، حقق 75% استجابة سريرية و 38% هجوعًا بالمنظار.[13]
التجارب الجارية
- RegentCol (NCT04938752). تجربة المرحلة الثانية مزدوجة التعمية بجامعة ميامي.
- RESET-UC. تجربة أسترالية للمرحلة الثانية لـ MSCs نخاع العظم الخيفي.
كيفية قياس النتائج في تجارب UC
- مقياس مايو (0–12). المؤشر المركب المعياري الذهبي الذي يجمع بين تكرار التبرز والنزف المستقيمي ونتائج المنظار والتقييم العام للطبيب.
- الدرجة الفرعية لمنظار مايو (0–3). الهجوع بالمنظار = درجة فرعية 0 أو 1.[14]
- الكالبروتكتين البرازي. بروتين مشتق من العدلات يقاس في البراز ويرتبط بالالتهاب بالمنظار.[15]
السلامة
تفاعلات التسريب الحادة هي أكثر الأحداث الضارة شيوعًا، عادة خفيفة — حمى عابرة، قشعريرة، صداع — وتحدث في حوالي 5–15% من عمليات التسريب. لم يلاحظ أي خطر متزايد للعدوى أو إشارات الورم.[17][18]
القيود الصادقة
- لا يوجد منتج MSC معتمد لـ UC. جميع العلاجات قيد البحث.
- تجارب صغيرة (أكبرها 212 مريضًا)، متابعة نادرًا ما تتجاوز 12 شهرًا.
- عدم تجانس منتجات MSC (مصادر وجرعات وجداول مختلفة).[12]
- التكلفة والوصول: التصنيع تحت ظروف GMP مكلف، والعلاج غير مشمول بالتأمين.
الخلاصة
يجلس علاج MSC لالتهاب القولون التقرحي في لحظة مثيرة حقًا. الأساس الآلي قوي — UC هو أساسًا مرض خلل التنظيم المناعي المخاطي وفشل الحاجز، وهما بالضبط المحوران اللذان تستهدفهما MSCs. تظهر البيانات السريرية المبكرة من التجارب العشوائية إشارات متسقة للفعالية مع ملف سلامة نظيف. لكن قاعدة الأدلة لا تزال صغيرة، والجرعة والجدول الأمثل غير محددين، ولا يوجد منتج معتمد. للمرضى الذين يعانون من UC المعتدل ويفقدون الاستجابة للعلاجات البيولوجية، يمثل علاج MSC خيارًا بحثيًا واعدًا — ليس معيار رعاية، بل أحد أكثر الجبهات العلمية رسوخًا في أبحاث أمراض الأمعاء الالتهابية.
المراجع
- Ungaro R et al. Ulcerative colitis. Lancet. 2017;389:1756-1770. ↩
- Kobayashi T et al. Ulcerative colitis. Nat Rev Dis Primers. 2020;6:74. ↩
- Geremia A et al. Innate and adaptive immunity in IBD. Autoimmun Rev. 2014;13:3-10. ↩
- Martini E et al. Epithelial barrier in IBD. Cell Mol Gastroenterol Hepatol. 2017;4:33-46. ↩
- Neurath MF. Cytokines in IBD. Nat Rev Immunol. 2014;14:329-342. ↩
- Shi Y et al. Immunoregulatory mechanisms of MSCs. Nat Rev Nephrol. 2018;14:493-507. ↩
- Bernardo ME, Fibbe WE. MSCs: sensors and switchers. Cell Stem Cell. 2013;13:392-402. ↩
- Sala E et al. MSCs reduce colitis via TSG6. Gastroenterology. 2015;149:163-176. ↩
- Yabana T et al. MSC epithelial engraftment. J Pathol. 2009;218:350-359. ↩
- Panés J et al. Cx601 for perianal fistulas. Lancet. 2016;388:1281-1290. ↩
- Hu J et al. MSC infusion for UC. Stem Cells Transl Med. 2022;11:467-477. ↩
- Liu J et al. MSC therapy for UC meta-analysis. Stem Cell Res Ther. 2023;14:152. ↩
- Lanzoni G et al. Endoscopic MSC injection. Gastrointest Endosc. 2021;94:1156-1165. ↩
- Schroeder KW et al. Oral 5-ASA for UC. N Engl J Med. 1987;317:1625-1629. ↩
- D'Haens G et al. Fecal calprotectin. Inflamm Bowel Dis. 2012;18:2218-2224. ↩
- Dave M et al. MSC for IBD meta-analysis. Inflamm Bowel Dis. 2022;28:1250-1260. ↩
- Lalu MM et al. SafeCell review. PLoS ONE. 2012;7:e47559. ↩
- Barkholt L et al. Tumorigenicity risk MSCs. Cytotherapy. 2013;15:753-759. ↩
- Ankrum JA et al. MSCs: immune evasive. Nat Biotechnol. 2014;32:252-260. ↩
- Galipeau J, Sensébé L. MSC clinical challenges. Cell Stem Cell. 2018;22:824-833. ↩
- Phinney DG, Pittenger MF. MSC-derived exosomes. Stem Cells. 2017;35:851-858. ↩


