Bronchopulmonary Dysplasia (BPD) affects approximately 10,000–15,000 preterm infants annually in the United States alone, with incidence rising as neonatal intensive care saves increasingly premature babies. BPD is a chronic lung disease that develops when extremely preterm infants — born before 28 weeks gestation — receive prolonged mechanical ventilation and oxygen therapy. The immature lung, exposed to hyperoxia, volutrauma, and inflammation, arrests its development: alveolar septation halts, capillary networks fail to form, and the lung becomes a simplified, fibrotic, poorly gas-exchanging organ. Current management — gentle ventilation strategies, postnatal steroids, surfactant, and diuretics — supports survival but does not reverse the structural damage. A significant proportion of BPD survivors face lifelong pulmonary morbidity: recurrent respiratory infections, asthma-like symptoms, exercise intolerance, and pulmonary hypertension. MSC therapy is being studied as a regenerative approach that targets the underlying biology — not just managing symptoms, but restoring the cellular architecture the preterm lung failed to build.[1]
What happens in the BPD lung
BPD is fundamentally a disease of arrested lung development. In the normal third trimester, the fetal lung undergoes a critical phase of alveolarization — the formation of millions of tiny air sacs (alveoli) from terminal saccules — alongside the parallel development of a dense capillary network for gas exchange. When a preterm infant is born at 24–27 weeks, this program is barely underway. The mechanical ventilation and supplemental oxygen that sustain life simultaneously unleash a triad of damage: oxidative stress from hyperoxia, barotrauma from positive-pressure ventilation, and a robust inflammatory cascade involving neutrophils, macrophages, and pro-inflammatory cytokines (IL-1β, IL-6, IL-8, TNF-α).[2]
The result is a lung with fewer and larger alveoli. On histology, the BPD lung shows alveolar simplification — fewer septa, reduced internal surface area, dysmorphic pulmonary vasculature, and variable interstitial fibrosis. This is not scarred, normal lung; it is developmentally frozen lung. The clinical consequences — tachypnea, oxygen dependence, CO₂ retention, pulmonary hypertension — all trace back to this structural deficit.
The therapeutic gap is clear. Postnatal dexamethasone can reduce BPD severity but carries significant neurodevelopmental risk. Caffeine, vitamin A, and gentle ventilation help at the margins. None of these interventions regenerate lost alveoli or restore the pulmonary capillary bed. This is where MSC therapy enters the conversation — not as a replacement for current care, but as a regenerative adjunct that addresses what current care cannot.
How MSC therapy works in the BPD lung
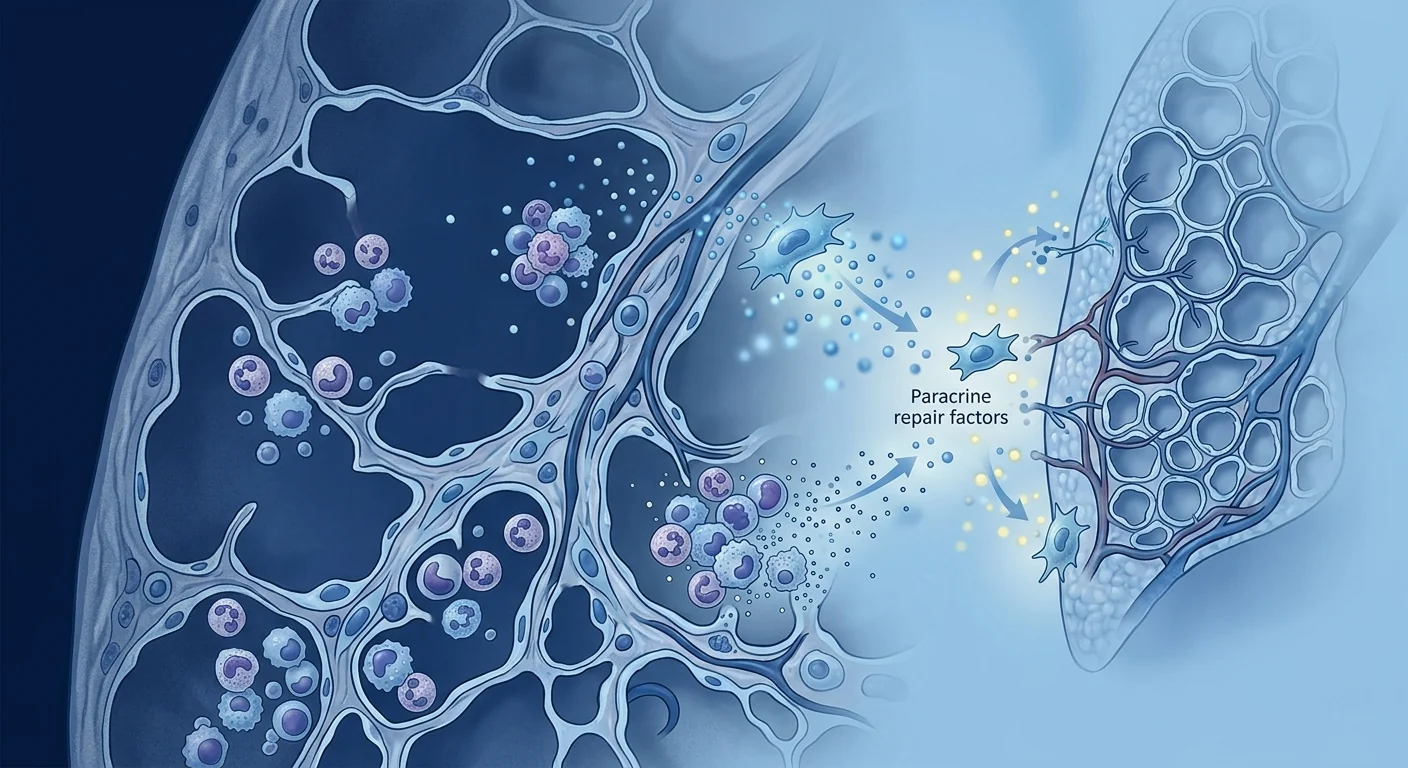
When clinical-grade Mesenchymal Stem Cells are delivered intravenously or intratracheally in the neonatal period, they do not engraft long-term as replacement lung cells. Their protective and regenerative effects are paracrine — mediated by a secretome of bioactive molecules that signal the injured lung to stop inflaming and start repairing. The evidence from preclinical models (rodent and lamb hyperoxia models) and early-phase human trials points to several complementary mechanisms:[3]
1. Anti-inflammatory protection
MSCs are exquisitely sensitive to inflammatory cues. In the hyperoxic BPD lung, they respond by secreting TSG-6 (TNF-stimulated gene 6), PGE2, and IL-10 — potent anti-inflammatory mediators that suppress alveolar macrophage activation, reduce neutrophil infiltration, and dampen the IL-1β/IL-6/TNF-α cytokine storm that drives tissue destruction. This is arguably the best-characterized mechanism and the primary rationale for early MSC administration.[4]
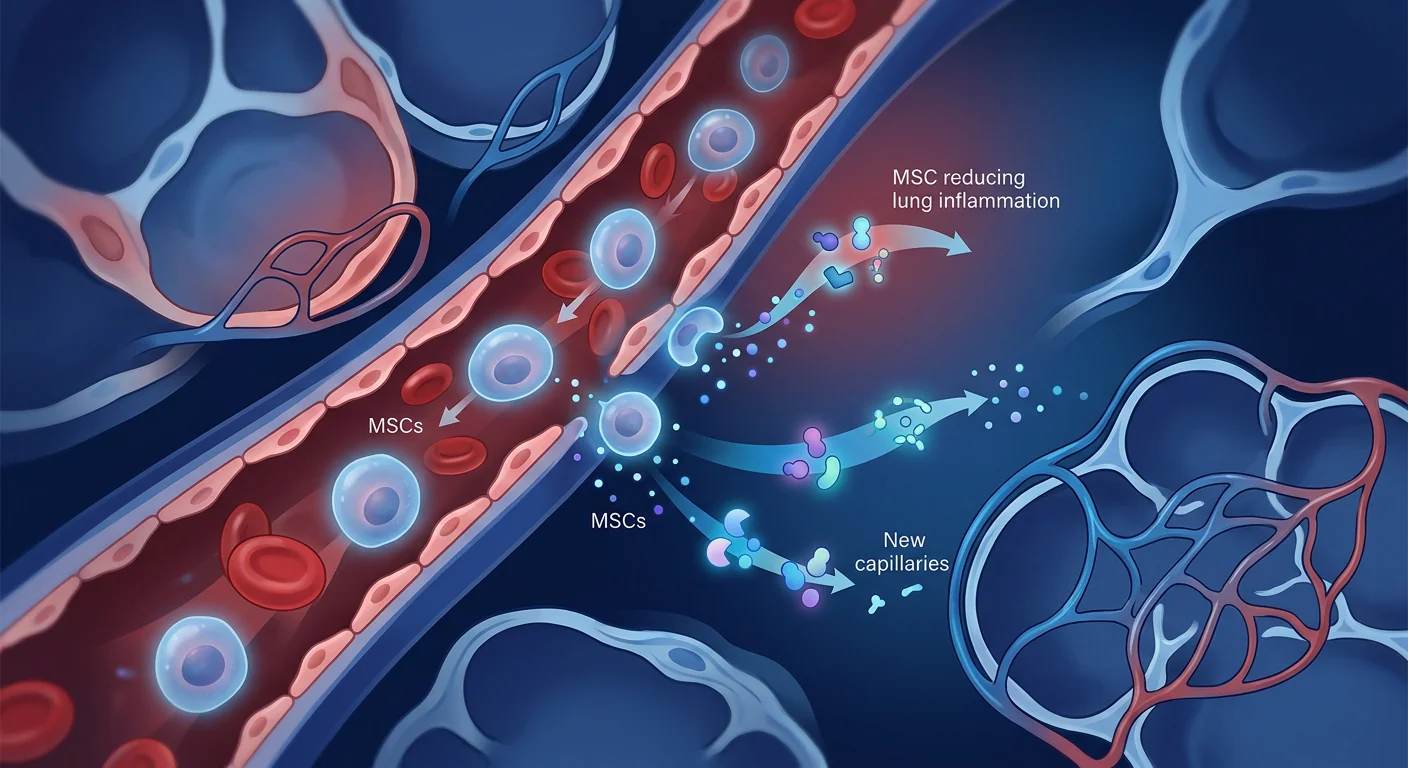
2. Alveolar and vascular regeneration
MSC-derived growth factors — VEGF (vascular endothelial growth factor), HGF (hepatocyte growth factor), and KGF (keratinocyte growth factor) — stimulate both alveolar epithelial type II cell proliferation and pulmonary capillary angiogenesis. In hyperoxia-exposed rodent pups, MSC treatment increases radial alveolar counts (the histological measure of alveolarization), restores septal thickness toward normal, and rebuilds the pulmonary microvasculature that had been obliterated by hyperoxia.[5]
3. Anti-fibrotic effects
The BPD lung has variable interstitial fibrosis that further limits gas exchange. MSC-derived factors — particularly HGF and TSG-6 — suppress TGF-β1 signaling, inhibit myofibroblast differentiation, and promote matrix metalloproteinase-mediated remodeling of existing fibrotic tissue. The net effect is a shift from fibrosis toward normal alveolar septation.[6]
4. Mitochondrial transfer
One of the more remarkable discoveries in MSC biology is the direct transfer of healthy mitochondria from MSCs to injured alveolar epithelial cells via tunneling nanotubes and extracellular vesicles. Hyperoxia damages mitochondrial DNA and impairs oxidative phosphorylation in the alveolar epithelium. Restoring mitochondrial function rescues cellular energy metabolism, reduces apoptosis, and supports surfactant production — functions that are critically impaired in the BPD lung.[7]
5. Immunomodulation and infection defense
Preterm infants with BPD are exquisitely vulnerable to respiratory infections, which trigger exacerbations and further lung injury. MSC therapy enhances the lung's antimicrobial defenses through secretion of LL-37 (cathelicidin) and β-defensins, while simultaneously suppressing the excessive inflammation that infection provokes — a dual action that conventional anti-inflammatory drugs cannot achieve.[8]
Preclinical evidence: what animal models tell us
The preclinical case for MSC therapy in BPD is robust and built on multiple animal species — primarily neonatal rodents exposed to hyperoxia (the standard BPD model) and preterm lambs (which better recapitulate the human preterm lung architecture). Key findings from the literature include:[9]
- Improved alveolarization. MSC-treated hyperoxic rat pups consistently show higher radial alveolar counts, increased mean linear intercept (smaller, more numerous alveoli), and restoration of septal thickness to near-normoxic control levels.
- Reduced pulmonary hypertension. In rodent and lamb models, MSC treatment reduces right ventricular systolic pressure, decreases medial wall thickness of pulmonary arterioles, and improves right ventricular hypertrophy indices — addressing the pulmonary hypertension that is a major source of mortality in severe BPD.
- Decreased inflammation. Bronchoalveolar lavage fluid from MSC-treated animals shows significantly lower total cell counts, neutrophil percentages, and concentrations of IL-1β, IL-6, TNF-α, and MCP-1 compared to vehicle-treated hyperoxia controls.
- Sustained benefit. Effects persist weeks after a single MSC dose, consistent with a reprogramming of the lung's inflammatory and regenerative environment rather than a transient pharmacological effect.
Key insight from preclinical work. Conditioned medium from MSCs — the growth factors and cytokines the cells secrete, without the cells themselves — reproduces most of the therapeutic benefit in hyperoxia models. This strongly supports the paracrine hypothesis and has spurred interest in cell-free products (exosomes, conditioned medium) as future BPD therapies that avoid the logistical complexity of live-cell administration.
Clinical evidence: what the human trials show
The translation of MSC therapy from bench to BPD bedside has been one of the more successful stories in neonatal regenerative medicine. Multiple phase I and phase II clinical trials have been conducted, primarily in South Korea and the United States, using umbilical cord blood-derived or umbilical cord tissue-derived MSCs:[10]
- Ahn et al. (2018) — Phase II randomized controlled trial (South Korea). Preterm infants at high risk for BPD (23–28 weeks gestation, on ventilator support at day 5–14) received a single intratracheal dose of 1×10⁷/kg human umbilical cord blood-derived MSCs or placebo. At 36 weeks corrected age, the MSC group showed significantly lower BPD severity. Secondary outcomes, including duration of ventilation and length of NICU stay, trended favorably. Long-term follow-up at 2–5 years showed no excess adverse events, no tumor formation, and comparable neurodevelopmental outcomes to controls.
- Chang et al. (2014) — Phase I dose-escalation trial. Intratracheal MSCs in preterm infants were feasible and safe, with no dose-limiting toxicities. Cytokine analysis of tracheal aspirates confirmed the anti-inflammatory mechanism — IL-6, IL-8, and TNF-α levels decreased in tracheal fluid within days of MSC administration.
- Powell et al. (2021) — Phase I safety trial (USA). Intravenous delivery of bone marrow-derived MSCs in preterm infants showed a favorable safety profile with no infusion-related adverse events, no deterioration in respiratory status, and encouraging signals in cytokine profiles.
- Ongoing and planned trials. Larger multicenter phase II/III trials are in various stages of planning and recruitment, including trials of repeated dosing (multiple MSC administrations over the first weeks of life) and trials combining MSC therapy with other interventions like caffeine and vitamin A.
An important caveat. The published trials to date are small (typically 9–30 patients) and designed to establish safety and feasibility, not efficacy. They are encouraging but do not yet constitute proof that MSC therapy reduces BPD incidence or severity in a statistically definitive way. Larger randomized controlled trials are needed before MSC therapy can be considered a standard-of-care intervention for BPD.
Practical considerations: timing, route, and dosing
Based on the available preclinical and clinical data, the following treatment parameters are emerging as the most plausible for clinical translation:
Timing. The therapeutic window for BPD is broader than for acute neonatal brain injury. While earlier intervention — during the inflammatory phase of evolving BPD (typically days 5–14 of life in high-risk preterm infants) — is theoretically preferable, the MSC mechanism (paracrine, anti-inflammatory, regenerative) may provide benefit even in established BPD. The ideal timing likely depends on the specific goal: inflammation suppression (early) versus alveolar regeneration (later).
Route of administration. Two routes have been studied in human trials: intratracheal (direct instillation into the airways) and intravenous. Intratracheal delivery achieves higher local pulmonary concentrations and may be more efficient for lung-targeted effects, but it is invasive and requires the infant to be intubated. Intravenous delivery is less invasive, allows multiple doses, and capitalizes on the well-documented pulmonary first-pass effect — MSCs administered IV are transiently trapped in the pulmonary capillary bed, achieving high lung exposure before redistributing systemically.
Dosing. Published trials have used doses of 1×10⁷ to 2×10⁷ cells/kg, administered as a single dose. Whether repeated dosing (weekly or biweekly during the NICU stay) provides additional benefit is an open question being addressed in ongoing trials. The remarkable safety record of neonatal MSC therapy to date — no tumor formation, no infusion reactions, no excess adverse events — makes higher doses and repeated dosing intervals plausible for investigation.
Safety in the neonatal population
The safety profile of MSC therapy in preterm neonates deserves particular attention because this is one of the most vulnerable patient populations in medicine. Reassuringly, the safety data from published neonatal trials — in BPD, HIE, and other neonatal indications — are consistently benign:[11]
- No tumorigenicity. Despite theoretical concerns about MSC engraftment and transformation, no cases of tumor formation have been reported in any neonatal MSC trial with multi-year follow-up.
- No infusion reactions. Unlike some cell therapies that provoke immediate hypersensitivity, neonatal MSC infusions have been well tolerated with no acute respiratory or hemodynamic compromise.
- No excess infection. MSC therapy does not appear to increase infection risk — indeed, preclinical data suggest enhanced antimicrobial peptide production may reduce infection susceptibility.
- Neurodevelopmental outcomes. Long-term follow-up (2–5 years) of infants treated in the Korean BPD trials has shown no excess neurodevelopmental impairment compared to matched controls. This is critical because any new therapy in the NICU must pass the neurodevelopmental bar.
Limitations and realistic expectations
It is essential to state plainly what MSC therapy for BPD is and is not. It is an investigational therapy supported by strong preclinical rationale and encouraging phase I/II safety data. It is not a cure, and it does not replace current NICU management — gentle ventilation, optimal nutrition, infection prevention, and careful oxygen targeting remain the bedrock of BPD care.
Several important unknowns remain:
- Efficacy in large randomized trials has not yet been demonstrated.
- The optimal cell source (umbilical cord blood, umbilical cord tissue, bone marrow, or allogeneic versus autologous), dose, route, timing, and dosing interval all require further investigation.
- Whether cell-free products (MSC-derived exosomes or conditioned medium) can replicate the benefits of live cells is an active area of research with significant commercial implications.
- The durability of benefit — whether improved alveolarization at 36 weeks translates to normal lung function in childhood and adulthood — is unknown.
Families considering MSC therapy for a preterm infant with or at risk for BPD should engage with a clinical team experienced in both neonatal intensive care and cell therapy. The decision involves weighing the encouraging safety record and preclinical data against the absence of large-scale efficacy trials and the significant logistical demands of accessing cell therapy in the NICU setting.[12]
Frequently Asked Questions
What is bronchopulmonary dysplasia (BPD)?
BPD is a chronic lung disease that affects extremely preterm infants who require mechanical ventilation and oxygen therapy after birth. The immature lung arrests its development — alveolar septation stops, capillaries fail to form, and the lung develops a simplified, fibrotic architecture that impairs gas exchange. Approximately 40% of infants born before 28 weeks develop some degree of BPD.
How can stem cells help repair BPD lung damage?
MSCs work through paracrine signaling — they secrete anti-inflammatory molecules (TSG-6, IL-10), growth factors (VEGF, HGF, KGF) that stimulate alveolar and vascular regeneration, and anti-fibrotic factors that suppress scar formation. They do not need to become lung cells; they signal the infant's own lung to repair itself.
What evidence supports MSC therapy for BPD?
Preclinical studies in hyperoxic rodent and lamb models consistently show improved alveolarization, reduced inflammation, and decreased pulmonary hypertension after MSC treatment. Phase I and II human trials in South Korea and the United States have demonstrated safety and feasibility, with encouraging signals in BPD severity reduction. Larger confirmatory trials are ongoing.
Is MSC therapy safe for preterm babies?
Safety data from published neonatal MSC trials are reassuring: no tumor formation, no acute infusion reactions, no excess infections, and normal neurodevelopmental outcomes at 2–5 year follow-up. However, the total number of treated neonates remains small (under 200 in published trials), and continued vigilance in larger studies is necessary.
When is the best time to give MSCs for BPD?
The optimal timing is not yet established. Early administration (days 5–14 of life) during the inflammatory phase of evolving BPD is the approach used in most published trials and makes theoretical sense for suppressing the inflammatory cascade. However, the paracrine mechanism may also benefit infants with established BPD by stimulating alveolar regeneration, though this is less well studied.
How much does MSC therapy for BPD cost?
MSC therapy for BPD remains investigational and is not yet a standard-of-care treatment — costs vary by provider and country. At VELAR Center in Bangkok, comprehensive consultation includes candidacy evaluation, treatment protocol design, and an honest discussion of evidence, expected outcomes, and limitations based on the most current published data.
References
- Thébaud B, Goss KN, Laughon M, et al. Bronchopulmonary dysplasia. Nature Reviews Disease Primers. 2019;5(1):78. doi:10.1038/s41572-019-0127-7 ↩
- Jobe AH, Bancalari E. Bronchopulmonary dysplasia. American Journal of Respiratory and Critical Care Medicine. 2001;163(7):1723-1729. doi:10.1164/ajrccm.163.7.2011060 ↩
- Ahn SY, Chang YS, Park WS. Mesenchymal stem cells for bronchopulmonary dysplasia: a comprehensive review of preclinical and clinical studies. Stem Cells Translational Medicine. 2021;10(2):198-210. doi:10.1002/sctm.20-0296 ↩
- Willis GR, Fernandez-Gonzalez A, Reis M, Mitsialis SA, Kourembanas S. Mesenchymal stromal cell exosomes improve alveolarization and pulmonary vascular development in experimental BPD. American Journal of Respiratory and Critical Care Medicine. 2018;197(1):104-116. doi:10.1164/rccm.201705-0921OC ↩
- Chang YS, Ahn SY, Yoo HS, et al. Mesenchymal stem cells for bronchopulmonary dysplasia: phase 1 dose-escalation clinical trial. Journal of Pediatrics. 2014;164(5):966-972.e6. doi:10.1016/j.jpeds.2013.12.011 ↩
- Aslam M, Baveja R, Liang OD, et al. Bone marrow stromal cells attenuate lung injury in a murine model of neonatal chronic lung disease. American Journal of Respiratory and Critical Care Medicine. 2009;180(11):1122-1130. doi:10.1164/rccm.200902-0242OC ↩
- Islam MN, Das SR, Emin MT, et al. Mitochondrial transfer from bone-marrow-derived stromal cells to pulmonary alveoli protects against acute lung injury. Nature Medicine. 2012;18(5):759-765. doi:10.1038/nm.2736 ↩
- Krasnodembskaya A, Song Y, Fang X, et al. Antibacterial effect of human mesenchymal stem cells is mediated in part from secretion of the antimicrobial peptide LL-37. Stem Cells. 2010;28(12):2229-2238. doi:10.1002/stem.544 ↩
- Fung ME, Thébaud B. Stem cell-based therapy for neonatal lung disease. Cell and Tissue Research. 2014;356(1):161-169. doi:10.1007/s00441-013-1785-5 ↩
- Ahn SY, Chang YS, Sung SI, Park WS. Mesenchymal stem cells for severe intraventricular hemorrhage in preterm infants: phase I dose-escalation clinical trial. Stem Cells Translational Medicine. 2018;7(12):847-856. doi:10.1002/sctm.17-0218 ↩
- Namba F, Kitagawa H, Go S, et al. Mesenchymal stem cells for the prevention of bronchopulmonary dysplasia. Pediatrics International. 2020;62(9):1061-1067. doi:10.1111/ped.14271 ↩
- Pierro M, Thébaud B. Mesenchymal stem cells and the treatment of neonatal lung disease. Seminars in Fetal and Neonatal Medicine. 2021;26(6):101311. doi:10.1016/j.siny.2021.101311 ↩
在美国,每年约有 10,000–15,000 名早产儿 患上支气管肺发育不良(BPD),随着新生儿重症监护技术挽救了越来越多的极早早产儿,这一发病率仍在上升。BPD 是一种慢性肺病,当极早早产儿(妊娠不足 28 周出生)接受长时间的机械通气和氧疗时发生。未成熟的肺部暴露于高氧、气压伤和炎症中,其发育被阻断:肺泡隔化停止,毛细血管网络无法形成,肺变成一个简化、纤维化、气体交换不良的器官。目前的管理手段——温和通气策略、产后类固醇、表面活性物质和利尿剂——能维持生命但无法逆转结构性损伤。相当比例的 BPD 幸存者面临终生肺部疾病:反复呼吸道感染、哮喘样症状、运动不耐受和肺动脉高压。MSC 疗法正在被研究作为一种再生方法,针对根本的生物学机制——不仅仅是管理症状,而是恢复早产肺未能构建的细胞结构。[1]
BPD 肺部发生了什么
BPD 本质上是一种 肺发育停滞 的疾病。在正常妊娠晚期,胎儿肺经历一个关键的肺泡化阶段——从终末囊泡形成数百万个微小气囊(肺泡)——同时并行发展致密的毛细血管网络以进行气体交换。当早产儿在 24–27 周出生时,这一程序才刚刚开始。维持生命的机械通气和补充氧气同时释放三重损伤:高氧引起的氧化应激、正压通气造成的气压伤,以及涉及中性粒细胞、巨噬细胞和促炎细胞因子(IL-1β、IL-6、IL-8、TNF-α)的强烈炎症级联反应。[2]
结果是肺泡数量减少且体积增大。 在组织学上,BPD 肺显示肺泡简化——间隔更少、内部表面积减少、肺血管形态异常和不同程度的间质纤维化。这不是疤痕化的正常肺;这是发育冻结的肺。临床后果——呼吸急促、氧依赖、CO₂潴留、肺动脉高压——都可追溯到这一结构性缺陷。
治疗缺口很明显。 产后地塞米松可以降低 BPD 严重程度,但具有显著的神经发育风险。咖啡因、维生素 A 和温和通气在边缘上有所帮助。这些干预措施中没有一个能再生丧失的肺泡或恢复肺毛细血管床。这就是 MSC 疗法进入讨论的地方——不是替代现有治疗,而是作为一种再生辅助手段,解决现有治疗无法解决的问题。
MSC 疗法在 BPD 肺中如何起作用
当临床级间充质干细胞在新生儿期通过静脉或气管内递送时,它们并不作为替代肺细胞长期植入。它们的保护和再生效应是旁分泌的——由一组生物活性分子介导,这些分子信号受损肺部停止炎症并开始修复。来自临床前模型(啮齿动物和羔羊高氧模型)和早期人体试验的证据指向几种互补机制:[3]
1. 抗炎保护
MSC 对炎症信号极为敏感。在高氧 BPD 肺中,它们通过分泌 TSG-6(TNF 刺激基因 6)、PGE2 和 IL-10 作出反应——这些强效抗炎介质抑制肺泡巨噬细胞活化、减少中性粒细胞浸润,并抑制驱动组织破坏的 IL-1β/IL-6/TNF-α 细胞因子风暴。这是文献记录最充分的机制,也是早期 MSC 给药的主要理论依据。[4]
2. 肺泡和血管再生
MSC 来源的生长因子——VEGF(血管内皮生长因子)、HGF(肝细胞生长因子)和 KGF(角质形成细胞生长因子)——同时刺激肺泡 II 型上皮细胞增殖和肺毛细血管血管生成。在暴露于高氧的啮齿动物幼崽中,MSC 治疗增加径向肺泡计数(肺泡化的组织学指标),将间隔厚度恢复到正常水平,并重建被高氧破坏的肺微血管系统。[5]
3. 抗纤维化效应
BPD 肺存在不同程度的间质纤维化,进一步限制气体交换。MSC 来源的因子——特别是 HGF 和 TSG-6——抑制 TGF-β1 信号传导,抑制肌成纤维细胞分化,并促进基质金属蛋白酶介导的现有纤维化组织重塑。净效应是从纤维化转向正常肺泡间隔形成。[6]
4. 线粒体转移
MSC 生物学中更引人注目的发现之一是通过隧道纳米管和细胞外囊泡将健康线粒体从 MSC 直接转移到受损的肺泡上皮细胞。高氧损伤肺泡上皮中的线粒体 DNA 并损害氧化磷酸化。恢复线粒体功能可拯救细胞能量代谢、减少凋亡并支持表面活性物质产生——这些功能在 BPD 肺中严重受损。[7]
5. 免疫调节和感染防御
患有 BPD 的早产儿极易受到呼吸道感染,感染会触发病情加重和进一步的肺损伤。MSC 疗法通过分泌 LL-37(cathelicidin)和 β-防御素增强肺部的抗菌防御能力,同时抑制感染引发的过度炎症——这是传统抗炎药物无法实现的双重作用。[8]
临床前证据:动物模型告诉我们什么
MSC 疗法在 BPD 中的临床前案例是坚实的,基于多种动物物种——主要是暴露于高氧的新生啮齿动物(标准 BPD 模型)和早产羔羊(更好地再现人类早产肺结构)。文献中的关键发现包括:[9]
- 改善肺泡化。 MSC 处理的高氧大鼠幼崽一致显示更高的径向肺泡计数、增加的平均线性截距(更小、更多的肺泡),以及间隔厚度恢复到接近正常氧对照水平。
- 降低肺动脉高压。 在啮齿动物和羔羊模型中,MSC 治疗降低右心室收缩压、减小肺小动脉中膜壁厚度,并改善右心室肥厚指数——解决肺动脉高压这一重症 BPD 的主要死亡原因。
- 减轻炎症。 MSC 处理动物的支气管肺泡灌洗液显示总细胞计数、中性粒细胞百分比和 IL-1β、IL-6、TNF-α、MCP-1 浓度较赋形剂处理的高氧对照显著降低。
- 持续获益。 单次 MSC 剂量后效应持续数周,与肺的炎症和再生环境重编程一致,而非短暂的药理学效应。
临床前工作的关键见解。 MSC 的条件培养基——细胞分泌的生长因子和细胞因子,不含细胞本身——在高氧模型中再现了大部分治疗效果。这强烈支持旁分泌假说,并激发了对无细胞产品(外泌体、条件培养基)作为未来 BPD 疗法的兴趣,这些产品避免了活细胞给药的后勤复杂性。
临床证据:人体试验显示什么
MSC 疗法从实验室到 BPD 临床的转化已成为新生儿再生医学中较为成功的故事之一。多项 I 期和 II 期临床试验已经进行,主要在韩国和美国,使用脐带血来源或脐带组织来源的 MSC:[10]
- Ahn 等(2018)— II 期随机对照试验(韩国)。 高 BPD 风险的早产儿(23–28 周妊娠,第 5–14 天仍需呼吸机支持)接受单次气管内剂量的 1×10⁷/kg 人脐带血来源 MSC 或安慰剂。在矫正年龄 36 周时,MSC 组显示显著较低的 BPD 严重程度。次要结局(包括通气持续时间和 NICU 住院时间)趋势良好。2–5 年的长期随访显示无额外不良事件、无肿瘤形成,且神经发育结局与对照组相当。
- Chang 等(2014)— I 期剂量递增试验。 早产儿气管内 MSC 给药可行且安全,无剂量限制性毒性。气管吸出物的细胞因子分析证实了抗炎机制——MSC 给药后数日内气管液中 IL-6、IL-8 和 TNF-α 水平下降。
- Powell 等(2021)— I 期安全性试验(美国)。 早产儿静脉输注骨髓来源 MSC 显示良好的安全性,无输注相关不良事件,无呼吸状态恶化,细胞因子谱中出现令人鼓舞的信号。
- 正在进行和计划中的试验。 更大规模的多中心 II/III 期试验处于不同的计划和招募阶段,包括重复给药试验(在出生后首周多次 MSC 给药)以及 MSC 疗法与其他干预措施(如咖啡因和维生素 A)联合使用的试验。
重要注意事项。 迄今为止已发表的试验规模较小(通常 9–30 名患者),设计用于建立安全性和可行性,而非有效性。它们令人鼓舞,但尚未构成 MSC 疗法以统计学确定性降低 BPD 发病率或严重程度的证据。在 MSC 疗法被视为 BPD 的标准治疗干预之前,需要更大规模的随机对照试验。
实际考虑:时机、途径和剂量
基于现有的临床前和临床数据,以下治疗参数正在成为临床转化最合理的参数:
时机。 BPD 的治疗窗口比急性新生儿脑损伤更广。虽然早期干预——在进展性 BPD 的炎症阶段(通常是高危早产儿的第 5–14 天)——在理论上更为可取,但 MSC 机制(旁分泌、抗炎、再生)即使在已确诊的 BPD 中也可能提供获益。理想时机可能取决于具体目标:抑制炎症(早期)还是肺泡再生(后期)。
给药途径。 两种途径已在人体试验中研究:气管内(直接滴入气道)和静脉内。气管内递送达到更高的局部肺浓度,可能对肺靶向效应更有效,但它是侵入性的,需要婴儿插管。静脉内递送侵入性较小,允许多次给药,并利用文献充分记录的肺首过效应——静脉给药的 MSC 暂时滞留在肺毛细血管床中,在重新分布到全身之前达到高肺暴露。
剂量。 已发表的试验使用 1×10⁷ 至 2×10⁷ 细胞/kg 的剂量,单次给药。重复给药(在 NICU 住院期间每周或每两周给药)是否提供额外获益是一个开放性问题,正在进行的试验正在解决。新生儿 MSC 疗法迄今为止显著的安全性记录——无肿瘤形成、无输注反应、无额外不良事件——使更高剂量和重复给药间隔成为合理的研究方向。
新生儿人群中的安全性
MSC 疗法在早产新生儿中的安全性值得特别关注,因为这是医学中最脆弱的患者人群之一。令人放心的是,已发表的新生儿试验——在 BPD、HIE 和其他新生儿适应症中——的安全性数据一致良好:[11]
- 无致瘤性。 尽管存在 MSC 植入和转化的理论担忧,但在任何新生儿 MSC 试验中,经过多年随访,均未报告肿瘤形成病例。
- 无输注反应。 与某些可能引发即时超敏反应的细胞疗法不同,新生儿 MSC 输注耐受良好,无急性呼吸或血流动力学损害。
- 无额外感染。 MSC 疗法似乎不增加感染风险——事实上,临床前数据表明增强的抗菌肽产生可能降低感染易感性。
- 神经发育结局。 韩国 BPD 试验中治疗婴儿的长期随访(2–5 年)显示,与匹配对照相比,无额外的神经发育障碍。这至关重要,因为 NICU 中任何新疗法都必须通过神经发育关。
局限性和现实的期望
有必要明确说明 MSC 疗法对 BPD 是什么和不是什么。它是一种受强临床前理论基础和令人鼓舞的 I/II 期安全性数据支持的研究性疗法。它不是治愈方法,也不取代当前的 NICU 管理——温和通气、最佳营养、感染预防和仔细的氧目标仍然是 BPD 治疗的基础。
几个重要的未知因素仍然存在:
- 大规模随机试验中的有效性尚未得到证明。
- 最佳细胞来源(脐带血、脐带组织、骨髓,或同种异体与自体)、剂量、途径、时机和给药间隔都需要进一步研究。
- 无细胞产品(MSC 来源的外泌体或条件培养基)是否能复制活细胞的获益是一个活跃的研究领域,具有重要的商业意义。
- 获益的持久性——36 周时改善的肺泡化是否转化为儿童期和成年期的正常肺功能——尚不清楚。
考虑为患有或有 BPD 风险的早产儿进行 MSC 治疗的家庭应与在新生儿重症监护和细胞疗法方面均有经验的临床团队进行沟通。这一决定涉及在令人鼓舞的安全性记录和临床前数据与缺乏大规模有效性试验以及 NICU 环境中获取细胞疗法的显著后勤需求之间进行权衡。[12]
常见问题
什么是支气管肺发育不良(BPD)?
BPD 是一种慢性肺病,影响出生后需要机械通气和氧疗的极早早产儿。未成熟的肺部发育停滞——肺泡隔化停止,毛细血管无法形成,肺发展出简化的纤维化结构,损害气体交换。约 40% 在 28 周前出生的婴儿会出现某种程度的 BPD。
干细胞如何帮助修复 BPD 肺损伤?
MSC 通过旁分泌信号起作用——它们分泌抗炎分子(TSG-6、IL-10)、刺激肺泡和血管再生的生长因子(VEGF、HGF、KGF),以及抑制疤痕形成的抗纤维化因子。它们不需要成为肺细胞;它们信号婴儿自身的肺进行自我修复。
有什么证据支持 MSC 疗法治疗 BPD?
高氧啮齿动物和羔羊模型的临床前研究一致显示 MSC 治疗后肺泡化改善、炎症减轻和肺动脉高压降低。韩国和美国的 I 期和 II 期人体试验已证明安全性和可行性,在 BPD 严重程度降低方面出现了令人鼓舞的信号。更大规模的验证性试验正在进行中。
MSC 疗法对早产儿安全吗?
已发表的新生儿 MSC 试验的安全性数据令人放心:无肿瘤形成、无急性输注反应、无额外感染,2–5 年随访的神经发育结局正常。然而,治疗的新生儿总数仍然较小(已发表试验中不到 200 例),需要在更大规模的研究中继续保持警惕。
MSC 治疗 BPD 的最佳时机是什么?
最佳时机尚未确定。早期给药(出生后第 5–14 天)在进展性 BPD 的炎症阶段是大多数已发表试验中使用的方法,在理论上对抑制炎症级联反应有意义。然而,旁分泌机制也可能通过刺激肺泡再生使已确诊 BPD 的婴儿受益,尽管这方面的研究较少。
MSC 疗法治疗 BPD 的费用是多少?
BPD 的 MSC 疗法仍然是研究性的,尚未成为标准治疗——费用因提供者和国家而异。在曼谷 VELAR 中心,综合咨询包括候选资格评估、治疗方案设计,以及基于最新发表数据的关于证据、预期结局和局限性的诚实讨论。
参考文献
- Thébaud B, Goss KN, Laughon M, et al. Bronchopulmonary dysplasia. Nature Reviews Disease Primers. 2019;5(1):78. doi:10.1038/s41572-019-0127-7 ↩
- Jobe AH, Bancalari E. Bronchopulmonary dysplasia. American Journal of Respiratory and Critical Care Medicine. 2001;163(7):1723-1729. doi:10.1164/ajrccm.163.7.2011060 ↩
- Ahn SY, Chang YS, Park WS. Mesenchymal stem cells for bronchopulmonary dysplasia: a comprehensive review of preclinical and clinical studies. Stem Cells Translational Medicine. 2021;10(2):198-210. doi:10.1002/sctm.20-0296 ↩
- Willis GR, Fernandez-Gonzalez A, Reis M, Mitsialis SA, Kourembanas S. Mesenchymal stromal cell exosomes improve alveolarization and pulmonary vascular development in experimental BPD. American Journal of Respiratory and Critical Care Medicine. 2018;197(1):104-116. doi:10.1164/rccm.201705-0921OC ↩
- Chang YS, Ahn SY, Yoo HS, et al. Mesenchymal stem cells for bronchopulmonary dysplasia: phase 1 dose-escalation clinical trial. Journal of Pediatrics. 2014;164(5):966-972.e6. doi:10.1016/j.jpeds.2013.12.011 ↩
- Aslam M, Baveja R, Liang OD, et al. Bone marrow stromal cells attenuate lung injury in a murine model of neonatal chronic lung disease. American Journal of Respiratory and Critical Care Medicine. 2009;180(11):1122-1130. doi:10.1164/rccm.200902-0242OC ↩
- Islam MN, Das SR, Emin MT, et al. Mitochondrial transfer from bone-marrow-derived stromal cells to pulmonary alveoli protects against acute lung injury. Nature Medicine. 2012;18(5):759-765. doi:10.1038/nm.2736 ↩
- Krasnodembskaya A, Song Y, Fang X, et al. Antibacterial effect of human mesenchymal stem cells is mediated in part from secretion of the antimicrobial peptide LL-37. Stem Cells. 2010;28(12):2229-2238. doi:10.1002/stem.544 ↩
- Fung ME, Thébaud B. Stem cell-based therapy for neonatal lung disease. Cell and Tissue Research. 2014;356(1):161-169. doi:10.1007/s00441-013-1785-5 ↩
- Ahn SY, Chang YS, Sung SI, Park WS. Mesenchymal stem cells for severe intraventricular hemorrhage in preterm infants: phase I dose-escalation clinical trial. Stem Cells Translational Medicine. 2018;7(12):847-856. doi:10.1002/sctm.17-0218 ↩
- Namba F, Kitagawa H, Go S, et al. Mesenchymal stem cells for the prevention of bronchopulmonary dysplasia. Pediatrics International. 2020;62(9):1061-1067. doi:10.1111/ped.14271 ↩
- Pierro M, Thébaud B. Mesenchymal stem cells and the treatment of neonatal lung disease. Seminars in Fetal and Neonatal Medicine. 2021;26(6):101311. doi:10.1016/j.siny.2021.101311 ↩
يُصيب خلل التنسج القصبي الرئوي (BPD) حوالي 10,000–15,000 طفل خديج سنويًا في الولايات المتحدة وحدها، مع ارتفاع معدل الإصابة مع إنقاذ العناية المركزة لحديثي الولادة لأطفال خدج بشكل متزايد. BPD هو مرض رئوي مزمن يتطور عندما يتلقى الأطفال الخدج للغاية (المولودون قبل 28 أسبوعًا من الحمل) تهوية ميكانيكية مطولة وعلاجًا بالأكسجين. تتعرض الرئة غير الناضجة، المعرضة لفرط الأكسجين ورضح الحجم والالتهاب، لتوقف في تطورها: يتوقف تشكل الحويصلات الهوائية، وتفشل الشبكات الشعرية في التشكل، وتصبح الرئة عضوًا مبسطًا ومتليفًا وضعيف التبادل الغازي. تدعم الإدارة الحالية — استراتيجيات التهوية اللطيفة، والستيرويدات بعد الولادة، والمواد الخافضة للتوتر السطحي، ومدرات البول — البقاء على قيد الحياة لكنها لا تعكس الضرر الهيكلي. تواجه نسبة كبيرة من الناجين من BPD أمراضًا رئوية مدى الحياة: عدوى تنفسية متكررة، وأعراض تشبه الربو، وعدم تحمل التمارين، وارتفاع ضغط الدم الرئوي. يُدرس علاج MSC كنهج تجديدي يستهدف البيولوجيا الأساسية — ليس فقط إدارة الأعراض، بل استعادة البنية الخلوية التي فشلت رئة الطفل الخديج في بنائها.[1]
ما يحدث في رئة BPD
BPD هو في الأساس مرض توقف تطور الرئة. في الثلث الثالث الطبيعي من الحمل، تمر رئة الجنين بمرحلة حرجة من تشكل الحويصلات الهوائية — تكوين ملايين الأكياس الهوائية الدقيقة (الحويصلات) من الأكياس الطرفية — إلى جانب التطور الموازي لشبكة شعرية كثيفة لتبادل الغازات. عندما يولد طفل خديج في الأسبوع 24–27، يكون هذا البرنامج قد بدأ بالكاد. تطلق التهوية الميكانيكية والأكسجين الإضافي اللذان يدعمان الحياة في الوقت نفسه ثلاثية من الضرر: الإجهاد التأكسدي من فرط الأكسجين، ورضح الضغط من التهوية بالضغط الإيجابي، وسلسلة التهابية قوية تشمل العدلات والبلاعم والسيتوكينات المؤيدة للالتهاب (IL-1β، IL-6، IL-8، TNF-α).[2]
النتيجة هي رئة بعدد أقل من الحويصلات وأكبر حجمًا. من الناحية النسيجية، تُظهر رئة BPD تبسيطًا حويصليًا — حواجز أقل، مساحة سطح داخلية منخفضة، أوعية دموية رئوية مشوهة، وتليف خلالي متغير. هذه ليست رئة طبيعية متندبة؛ إنها رئة مجمدة تطوريًا. تعود العواقب السريرية — تسرع التنفس، والاعتماد على الأكسجين، واحتباس CO₂، وارتفاع ضغط الدم الرئوي — كلها إلى هذا العجز الهيكلي.
الفجوة العلاجية واضحة. يمكن للديكساميثازون بعد الولادة أن يقلل من شدة BPD لكنه يحمل خطرًا كبيرًا على النمو العصبي. يساعد الكافيين وفيتامين A والتهوية اللطيفة عند الهوامش. لا شيء من هذه التدخلات يجدد الحويصلات المفقودة أو يستعيد السرير الشعري الرئوي. هنا يدخل علاج MSC في المحادثة — ليس كبديل للرعاية الحالية، بل كمساعد تجديدي يعالج ما لا تستطيع الرعاية الحالية معالجته.
كيف يعمل علاج MSC في رئة BPD
عندما تُعطى الخلايا الجذعية الوسيطة من الدرجة السريرية عن طريق الوريد أو داخل الرغامى في فترة حديثي الولادة، فإنها لا تنغرس طويلًا كخلايا رئوية بديلة. تأثيراتها الوقائية والتجديدية هي باراكرينية — بوساطة سيكريتوم من الجزيئات النشطة بيولوجيًا التي تشير إلى الرئة المصابة لإيقاف الالتهاب وبدء الإصلاح. تشير الأدلة من النماذج قبل السريرية (نماذج فرط الأكسجين في القوارض والحملان) والتجارب البشرية المبكرة إلى عدة آليات متكاملة:[3]
١. الحماية المضادة للالتهاب
الخلايا الجذعية الوسيطة حساسة بشكل رائع للإشارات الالتهابية. في رئة BPD مفرطة الأكسجين، تستجيب بإفراز TSG-6 (الجين 6 المحفز بـ TNF)، وPGE2، وIL-10 — وسائط قوية مضادة للالتهاب تثبط تنشيط البلاعم السنخية، وتقلل من تسلل العدلات، وتخمد عاصفة السيتوكينات IL-1β/IL-6/TNF-α التي تدفع تدمير الأنسجة. هذه هي الآلية الأكثر توثيقًا والأساس المنطقي الرئيسي لإعطاء MSC المبكر.[4]
٢. التجديد الحويصلي والوعائي
عوامل النمو المشتقة من MSC — VEGF (عامل نمو بطانة الأوعية الدموية)، وHGF (عامل نمو الخلايا الكبدية)، وKGF (عامل نمو الخلايا الكيراتينية) — تحفز في الوقت نفسه تكاثر الخلايا الظهارية السنخية من النوع الثاني وتكون الأوعية الدموية الشعرية الرئوية. في صغار القوارض المعرضة لفرط الأكسجين، يزيد علاج MSC من تعداد الحويصلات الشعاعي (المقياس النسيجي للتشكل الحويصلي)، ويعيد سمك الحاجز نحو المستوى الطبيعي، ويعيد بناء الأوعية الدموية الدقيقة الرئوية التي طُمست بفعل فرط الأكسجين.[5]
٣. التأثيرات المضادة للتليف
تحتوي رئة BPD على تليف خلالي متغير يزيد من تقييد تبادل الغازات. عوامل MSC المشتقة — خاصة HGF وTSG-6 — تثبط إشارات TGF-β1، وتمنع تمايز الخلايا الليفية العضلية، وتعزز إعادة تشكيل النسيج الليفي الموجود بوساطة الميتالوبروتينازات المصفوفية. التأثير الصافي هو التحول من التليف نحو تشكل حاجز سنخي طبيعي.[6]
٤. نقل الميتوكوندريا
أحد أكثر الاكتشافات لفتًا في بيولوجيا MSC هو النقل المباشر للميتوكوندريا السليمة من MSC إلى الخلايا الظهارية السنخية المصابة عبر أنابيب النانو النفقية والحويصلات خارج الخلوية. يدمر فرط الأكسجين الحمض النووي للميتوكوندريا ويضعف الفسفرة التأكسدية في ظهارة السنخ. استعادة وظيفة الميتوكوندريا تنقذ استقلاب الطاقة الخلوي، وتقلل من الاستماتة، وتدعم إنتاج المواد الخافضة للتوتر السطحي — وهي وظائف معطلة بشكل حرج في رئة BPD.[7]
٥. التعديل المناعي والدفاع ضد العدوى
الأطفال الخدج المصابون بـ BPD معرضون بشكل كبير للعدوى التنفسية، التي تؤدي إلى نوبات تفاقم وإصابة رئوية إضافية. يعزز علاج MSC دفاعات الرئة المضادة للميكروبات من خلال إفراز LL-37 (كاثليسيدين) وβ-ديفينسينات، مع تثبيط الالتهاب المفرط الذي تثيره العدوى في الوقت نفسه — عمل مزدوج لا يمكن للأدوية التقليدية المضادة للالتهاب تحقيقه.[8]
الأدلة قبل السريرية: ما تخبرنا به النماذج الحيوانية
الحالة قبل السريرية لعلاج MSC في BPD قوية ومبنية على أنواع حيوانية متعددة — بشكل أساسي القوارض حديثة الولادة المعرضة لفرط الأكسجين (نموذج BPD القياسي) والحملان الخدج (التي تعيد تمثيل بنية الرئة البشرية الخدجة بشكل أفضل). تشمل النتائج الرئيسية من الأدبيات:[9]
- تحسين التشكل الحويصلي. تُظهر صغار الجرذان مفرطة الأكسجين المعالجة بـ MSC باستمرار تعدادات حويصلات شعاعية أعلى، وزيادة في متوسط الاعتراض الخطي (حويصلات أصغر وأكثر عددًا)، واستعادة سمك الحاجز إلى مستويات قريبة من مجموعة التحكم الطبيعية الأكسجين.
- انخفاض ارتفاع ضغط الدم الرئوي. في نماذج القوارض والحملان، يقلل علاج MSC من ضغط البطين الأيمن الانقباضي، ويقلل من سمك جدار الغلالة الوسطى للشرايين الرئوية، ويحسن مؤشرات تضخم البطين الأيمن — معالجًا ارتفاع ضغط الدم الرئوي الذي يعد مصدرًا رئيسيًا للوفيات في BPD الشديد.
- انخفاض الالتهاب. يُظهر سائل الغسيل القصبي السنخي من الحيوانات المعالجة بـ MSC تعدادات خلوية كلية أقل بكثير، ونسب عدلات أقل، وتركيزات أقل من IL-1β، IL-6، TNF-α، وMCP-1 مقارنة بمجموعات التحكم مفرطة الأكسجين المعالجة بالمركبة.
- فائدة مستدامة. تستمر التأثيرات لأسابيع بعد جرعة واحدة من MSC، بما يتوافق مع إعادة برمجة بيئة الرئة الالتهابية والتجديدية بدلاً من تأثير دوائي عابر.
رؤية رئيسية من العمل قبل السريري. الوسط المكيف من MSC — عوامل النمو والسيتوكينات التي تفرزها الخلايا، بدون الخلايا نفسها — يعيد إنتاج معظم الفائدة العلاجية في نماذج فرط الأكسجين. هذا يدعم بقوة فرضية الباراكرين وقد حفز الاهتمام بالمنتجات الخالية من الخلايا (الإكسوسومات، الوسط المكيف) كعلاجات مستقبلية لـ BPD تتجنب التعقيد اللوجستي لإعطاء الخلايا الحية.
الأدلة السريرية: ما تظهره التجارب البشرية
كانت ترجمة علاج MSC من المختبر إلى سرير BPD واحدة من أكثر القصص نجاحًا في الطب التجديدي لحديثي الولادة. أُجريت تجارب سريرية متعددة من المرحلة الأولى والثانية، بشكل أساسي في كوريا الجنوبية والولايات المتحدة، باستخدام MSC مشتقة من دم الحبل السري أو أنسجة الحبل السري:[10]
- Ahn وآخرون (2018) — تجربة معشاة مضبوطة من المرحلة الثانية (كوريا الجنوبية). تلقى أطفال خدج معرضون لخطر مرتفع من BPD (حمل 23–28 أسبوعًا، على دعم جهاز التنفس الصناعي في اليوم 5–14) جرعة واحدة داخل الرغامى من 1×10⁷/كجم من MSC دم الحبل السري البشري أو دواء وهمي. في عمر 36 أسبوعًا مصححًا، أظهرت مجموعة MSC شدة BPD أقل بشكل ملحوظ. كانت النتائج الثانوية، بما في ذلك مدة التهوية ومدة الإقامة في NICU، متجهة بشكل إيجابي. أظهرت المتابعة طويلة المدى عند 2–5 سنوات عدم وجود أحداث سلبية زائدة، وعدم تشكل أورام، ونتائج نمو عصبي مماثلة لمجموعة التحكم.
- Chang وآخرون (2014) — تجربة تصعيد الجرعة من المرحلة الأولى. كان إعطاء MSC داخل الرغامى للأطفال الخدج ممكنًا وآمنًا، بدون سميات محددة للجرعة. أكد تحليل السيتوكينات للرشف الرغامي الآلية المضادة للالتهاب — انخفضت مستويات IL-6 وIL-8 وTNF-α في سائل الرغامى في غضون أيام من إعطاء MSC.
- Powell وآخرون (2021) — تجربة السلامة من المرحلة الأولى (الولايات المتحدة). أظهر التسريب الوريدي لـ MSC المشتقة من نخاع العظم في الأطفال الخدج ملف سلامة مواتيًا بدون أحداث سلبية متعلقة بالتسريب، وبدون تدهور في الحالة التنفسية، وإشارات مشجعة في ملفات السيتوكينات.
- التجارب الجارية والمخطط لها. تجارب أكبر متعددة المراكز من المرحلة الثانية/الثالثة في مراحل مختلفة من التخطيط والتجنيد، بما في ذلك تجارب الجرعات المتكررة (إعطاءات MSC متعددة خلال الأسابيع الأولى من الحياة) وتجارب تجمع بين علاج MSC وتدخلات أخرى مثل الكافيين وفيتامين A.
تحفظ مهم. التجارب المنشورة حتى الآن صغيرة (عادة 9–30 مريضًا) ومصممة لإثبات السلامة والجدوى، وليس الفعالية. إنها مشجعة لكنها لا تشكل بعد دليلاً على أن علاج MSC يقلل من حدوث أو شدة BPD بطريقة محددة إحصائيًا. هناك حاجة إلى تجارب معشاة مضبوطة أكبر قبل اعتبار علاج MSC تدخلاً قياسيًا لـ BPD.
اعتبارات عملية: التوقيت والطريق والجرعة
استنادًا إلى البيانات قبل السريرية والسريرية المتاحة، تبرز معايير العلاج التالية كالأكثر منطقية للترجمة السريرية:
التوقيت. النافذة العلاجية لـ BPD أوسع من إصابة الدماغ الحادة عند حديثي الولادة. بينما يكون التدخل المبكر — خلال المرحلة الالتهابية لـ BPD المتطور (عادة الأيام 5–14 من الحياة لدى الأطفال الخدج المعرضين لخطر مرتفع) — مفضلاً نظريًا، قد توفر آلية MSC (باراكرينية، مضادة للالتهاب، تجديدية) فائدة حتى في BPD المثبت. يعتمد التوقيت المثالي على الأرجح على الهدف المحدد: تثبيط الالتهاب (مبكرًا) مقابل التجديد الحويصلي (لاحقًا).
طريق الإعطاء. تمت دراسة طريقين في التجارب البشرية: داخل الرغامى (تقطير مباشر في المجاري الهوائية) وعن طريق الوريد. يحقق التسريب داخل الرغامى تركيزات رئوية محلية أعلى وقد يكون أكثر كفاءة للتأثيرات المستهدفة للرئة، لكنه غازٍ ويتطلب تنبيب الرضيع. التسريب الوريدي أقل غزوًا، ويسمح بجرعات متعددة، ويستفيد من تأثير المرور الرئوي الأول الموثق جيدًا — MSC المعطاة وريديًا تُحتجز مؤقتًا في السرير الشعري الرئوي، محققة تعرضًا رئويًا عاليًا قبل إعادة التوزيع جهازيًا.
الجرعة. استخدمت التجارب المنشورة جرعات من 1×10⁷ إلى 2×10⁷ خلية/كجم، معطاة كجرعة واحدة. ما إذا كانت الجرعات المتكررة (أسبوعيًا أو كل أسبوعين خلال الإقامة في NICU) توفر فائدة إضافية هو سؤال مفتوح تعالجه التجارب الجارية. سجل السلامة الملحوظ لعلاج MSC عند حديثي الولادة حتى الآن — عدم تشكل أورام، وعدم وجود تفاعلات تسريب، وعدم وجود أحداث سلبية زائدة — يجعل الجرعات الأعلى وفترات الجرعات المتكررة معقولة للتحقيق.
السلامة في فئة حديثي الولادة
يستحق ملف سلامة علاج MSC لدى الخدج حديثي الولادة اهتمامًا خاصًا لأن هذه واحدة من أكثر فئات المرضى ضعفًا في الطب. بشكل مطمئن، بيانات السلامة من تجارب حديثي الولادة المنشورة — في BPD وHIE ومؤشرات حديثي الولادة الأخرى — حميدة باستمرار:[11]
- عدم وجود قدرة على تشكل الأورام. على الرغم من المخاوف النظرية حول انغراس MSC وتحولها، لم تُبلغ أي حالات لتشكل الأورام في أي تجربة MSC لحديثي الولادة مع متابعة متعددة السنوات.
- عدم وجود تفاعلات تسريب. على عكس بعض العلاجات الخلوية التي تثير فرط حساسية فوري، تم تحمل تسريبات MSC لحديثي الولادة بشكل جيد بدون تدهور تنفسي أو ديناميكي دموي حاد.
- عدم وجود عدوى زائدة. لا يبدو أن علاج MSC يزيد من خطر العدوى — في الواقع، تشير البيانات قبل السريرية إلى أن إنتاج الببتيدات المضادة للميكروبات المعزز قد يقلل من قابلية العدوى.
- نتائج النمو العصبي. أظهرت المتابعة طويلة المدى (2–5 سنوات) للأطفال المعالجين في التجارب الكورية لـ BPD عدم وجود ضعف في النمو العصبي زائد مقارنة بمجموعات التحكم المطابقة. هذا أمر بالغ الأهمية لأن أي علاج جديد في NICU يجب أن يجتاز معيار النمو العصبي.
القيود والتوقعات الواقعية
من الضروري أن نذكر بوضوح ما هو علاج MSC لـ BPD وما ليس هو. إنه علاج قيد البحث مدعوم بأساس قوي قبل سريري وبيانات سلامة مشجعة من المرحلة الأولى/الثانية. إنه ليس علاجًا شافيًا، ولا يحل محل إدارة NICU الحالية — التهوية اللطيفة، والتغذية المثلى، والوقاية من العدوى، واستهداف الأكسجين الدقيق تظل حجر الأساس لرعاية BPD.
تبقى عدة أمور مجهولة مهمة:
- لم تثبت الفعالية في التجارب العشوائية الكبيرة بعد.
- المصدر الخلوي الأمثل (دم الحبل السري، أنسجة الحبل السري، نخاع العظم، أو خيفي مقابل ذاتي)، والجرعة، والطريق، والتوقيت، وفاصل الجرعات كلها تتطلب مزيدًا من التحقيق.
- ما إذا كانت المنتجات الخالية من الخلايا (إكسوسومات مشتقة من MSC أو وسط مكيف) يمكنها تكرار فوائد الخلايا الحية هو مجال بحث نشط له آثار تجارية كبيرة.
- استدامة الفائدة — ما إذا كان تحسين التشكل الحويصلي عند 36 أسبوعًا يترجم إلى وظيفة رئوية طبيعية في الطفولة والبلوغ — غير معروف.
يجب على العائلات التي تفكر في علاج MSC لطفل خديج مصاب أو معرض لخطر BPD التواصل مع فريق سريري ذي خبرة في كل من العناية المركزة لحديثي الولادة والعلاج الخلوي. يتضمن القرار موازنة سجل السلامة المشجع والبيانات قبل السريرية مقابل غياب تجارب فعالية واسعة النطاق والمتطلبات اللوجستية الكبيرة للوصول إلى العلاج الخلوي في بيئة NICU.[12]
الأسئلة المتكررة
ما هو خلل التنسج القصبي الرئوي (BPD)؟
BPD هو مرض رئوي مزمن يصيب الأطفال الخدج للغاية الذين يحتاجون إلى تهوية ميكانيكية وعلاج بالأكسجين بعد الولادة. تتوقف الرئة غير الناضجة عن التطور — يتوقف تشكل الحويصلات الهوائية، وتفشل الشعيرات الدموية في التشكل، وتطور الرئة بنية مبسطة ومتليفة تضعف تبادل الغازات. حوالي 40% من الأطفال المولودين قبل 28 أسبوعًا يصابون بدرجة ما من BPD.
كيف يمكن للخلايا الجذعية المساعدة في إصلاح ضرر رئة BPD؟
تعمل MSC من خلال الإشارات الباراكرينية — تفرز جزيئات مضادة للالتهاب (TSG-6، IL-10)، وعوامل نمو (VEGF، HGF، KGF) تحفز التجديد الحويصلي والوعائي، وعوامل مضادة للتليف تثبط تشكل الندوب. لا تحتاج لأن تصبح خلايا رئوية؛ إنها تشير إلى رئة الرضيع لإصلاح نفسها.
ما الأدلة التي تدعم علاج MSC لـ BPD؟
تُظهر الدراسات قبل السريرية في نماذج القوارض والحملان مفرطة الأكسجين باستمرار تحسن التشكل الحويصلي، وانخفاض الالتهاب، وانخفاض ارتفاع ضغط الدم الرئوي بعد علاج MSC. أثبتت التجارب البشرية من المرحلة الأولى والثانية في كوريا الجنوبية والولايات المتحدة السلامة والجدوى، مع إشارات مشجعة في تقليل شدة BPD. التجارب التأكيدية الأكبر جارية.
هل علاج MSC آمن للأطفال الخدج؟
بيانات السلامة من تجارب MSC المنشورة لحديثي الولادة مطمئنة: عدم تشكل أورام، وعدم وجود تفاعلات تسريب حادة، وعدم وجود عدوى زائدة، ونتائج نمو عصبي طبيعية عند متابعة 2–5 سنوات. ومع ذلك، يبقى العدد الإجمالي لحديثي الولادة المعالجين صغيرًا (أقل من 200 في التجارب المنشورة)، واليقظة المستمرة في الدراسات الأكبر ضرورية.
ما هو أفضل وقت لإعطاء MSC لـ BPD؟
التوقيت الأمثل لم يثبت بعد. الإعطاء المبكر (الأيام 5–14 من الحياة) خلال المرحلة الالتهابية لـ BPD المتطور هو النهج المستخدم في معظم التجارب المنشورة وهو منطقي نظريًا لتثبيط السلسلة الالتهابية. ومع ذلك، قد تفيد الآلية الباراكرينية أيضًا الرضع المصابين بـ BPD المثبت عن طريق تحفيز التجديد الحويصلي، رغم أن هذا أقل دراسة.
كم تكلفة علاج MSC لـ BPD؟
يبقى علاج MSC لـ BPD قيد البحث وليس بعد علاجًا قياسيًا — تختلف التكاليف حسب المزود والبلد. في مركز VELAR في بانكوك، تشمل الاستشارة الشاملة تقييم الأهلية، وتصميم بروتوكول العلاج، ومناقشة صادقة للأدلة والنتائج المتوقعة والقيود بناءً على أحدث البيانات المنشورة.
المراجع
- Thébaud B, Goss KN, Laughon M, et al. Bronchopulmonary dysplasia. Nature Reviews Disease Primers. 2019;5(1):78. doi:10.1038/s41572-019-0127-7 ↩
- Jobe AH, Bancalari E. Bronchopulmonary dysplasia. American Journal of Respiratory and Critical Care Medicine. 2001;163(7):1723-1729. doi:10.1164/ajrccm.163.7.2011060 ↩
- Ahn SY, Chang YS, Park WS. Mesenchymal stem cells for bronchopulmonary dysplasia: a comprehensive review of preclinical and clinical studies. Stem Cells Translational Medicine. 2021;10(2):198-210. doi:10.1002/sctm.20-0296 ↩
- Willis GR, Fernandez-Gonzalez A, Reis M, Mitsialis SA, Kourembanas S. Mesenchymal stromal cell exosomes improve alveolarization and pulmonary vascular development in experimental BPD. American Journal of Respiratory and Critical Care Medicine. 2018;197(1):104-116. doi:10.1164/rccm.201705-0921OC ↩
- Chang YS, Ahn SY, Yoo HS, et al. Mesenchymal stem cells for bronchopulmonary dysplasia: phase 1 dose-escalation clinical trial. Journal of Pediatrics. 2014;164(5):966-972.e6. doi:10.1016/j.jpeds.2013.12.011 ↩
- Aslam M, Baveja R, Liang OD, et al. Bone marrow stromal cells attenuate lung injury in a murine model of neonatal chronic lung disease. American Journal of Respiratory and Critical Care Medicine. 2009;180(11):1122-1130. doi:10.1164/rccm.200902-0242OC ↩
- Islam MN, Das SR, Emin MT, et al. Mitochondrial transfer from bone-marrow-derived stromal cells to pulmonary alveoli protects against acute lung injury. Nature Medicine. 2012;18(5):759-765. doi:10.1038/nm.2736 ↩
- Krasnodembskaya A, Song Y, Fang X, et al. Antibacterial effect of human mesenchymal stem cells is mediated in part from secretion of the antimicrobial peptide LL-37. Stem Cells. 2010;28(12):2229-2238. doi:10.1002/stem.544 ↩
- Fung ME, Thébaud B. Stem cell-based therapy for neonatal lung disease. Cell and Tissue Research. 2014;356(1):161-169. doi:10.1007/s00441-013-1785-5 ↩
- Ahn SY, Chang YS, Sung SI, Park WS. Mesenchymal stem cells for severe intraventricular hemorrhage in preterm infants: phase I dose-escalation clinical trial. Stem Cells Translational Medicine. 2018;7(12):847-856. doi:10.1002/sctm.17-0218 ↩
- Namba F, Kitagawa H, Go S, et al. Mesenchymal stem cells for the prevention of bronchopulmonary dysplasia. Pediatrics International. 2020;62(9):1061-1067. doi:10.1111/ped.14271 ↩
- Pierro M, Thébaud B. Mesenchymal stem cells and the treatment of neonatal lung disease. Seminars in Fetal and Neonatal Medicine. 2021;26(6):101311. doi:10.1016/j.siny.2021.101311 ↩