Acute pancreatitis sends over 300,000 Americans to the hospital each year — and for the 15–20% who develop severe disease with persistent organ failure, the mortality rate remains 20–40% despite decades of supportive-care refinement. [1] There is no specific pharmacotherapy; treatment is fluids, pain control, and hoping the inflammatory cascade burns itself out before the patient's organs do.
Where conventional treatment falls short. The standard management of acute pancreatitis — aggressive intravenous fluid resuscitation, enteral nutrition, and organ support — addresses the consequences, not the cause. The pancreatic acinar cell injury that initiates the disease triggers a self-amplifying inflammatory loop: damaged acinar cells release damage-associated molecular patterns (DAMPs) that activate pancreatic macrophages, which secrete TNF-α, IL-1β, and IL-6, which recruit neutrophils, which release proteolytic enzymes and reactive oxygen species, which injure more acinar cells. [2] Breaking this loop pharmacologically has been the holy grail of pancreatitis research for 40 years — and it has eluded every single-target drug tested.
The deeper problem is immunological. Severe acute pancreatitis is fundamentally a systemic inflammatory response syndrome (SIRS) ignited in the retroperitoneum. The pancreatic inflammation releases cytokines, activated trypsin, and phospholipase A2 into the bloodstream, triggering endothelial activation, capillary leak, and multi-organ dysfunction — acute lung injury (ALI) is the most common and deadliest extrapancreatic complication. [3] By the time a patient is intubated in the ICU, the problem is no longer just pancreatitis — it is a body-wide immune dysregulation that anti-proteases and crystalloids cannot reverse.
MSC therapy targets the inflammatory root. Mesenchymal stem cells offer something no single-pathway drug has achieved: a network-level immunomodulatory intervention that simultaneously suppresses the pancreatic inflammatory cascade, protects the alveolar-capillary barrier from remote injury, promotes acinar cell regeneration, and enhances bacterial clearance — all while sensing the microenvironment and calibrating the response in real time. [4]
How MSC Therapy Works in Acute Pancreatitis
MSC therapy dampens pancreatic inflammation, preserves the microcirculation, protects distant organs from inflammatory injury, and promotes acinar cell regeneration through paracrine signaling. These mechanisms operate in parallel — not sequentially — making MSCs uniquely suited to a disease where multiple destructive pathways cascade simultaneously.
1. Cytokine Storm Suppression in the Pancreas
Within hours of intravenous infusion, MSCs home to the inflamed pancreas (guided by SDF-1/CXCR4 and other chemokine gradients) and begin secreting a potent anti-inflammatory cocktail: prostaglandin E2 (PGE2), tumor necrosis factor-stimulated gene 6 (TSG-6), transforming growth factor-β (TGF-β), interleukin-10 (IL-10), and indoleamine 2,3-dioxygenase (IDO). [6] In rat cerulein-induced pancreatitis models, a single intravenous MSC infusion reduced serum amylase by 65–80%, pancreatic myeloperoxidase (MPO — a neutrophil infiltration marker) by 50–70%, and pro-inflammatory cytokines (TNF-α, IL-1β, IL-6) by 50–85% within 24 hours. [7] Histologically, MSC-treated animals showed significantly less acinar cell necrosis, edema, and inflammatory infiltrate compared to vehicle controls.
2. Macrophage Polarization: M1 → M2 Shift
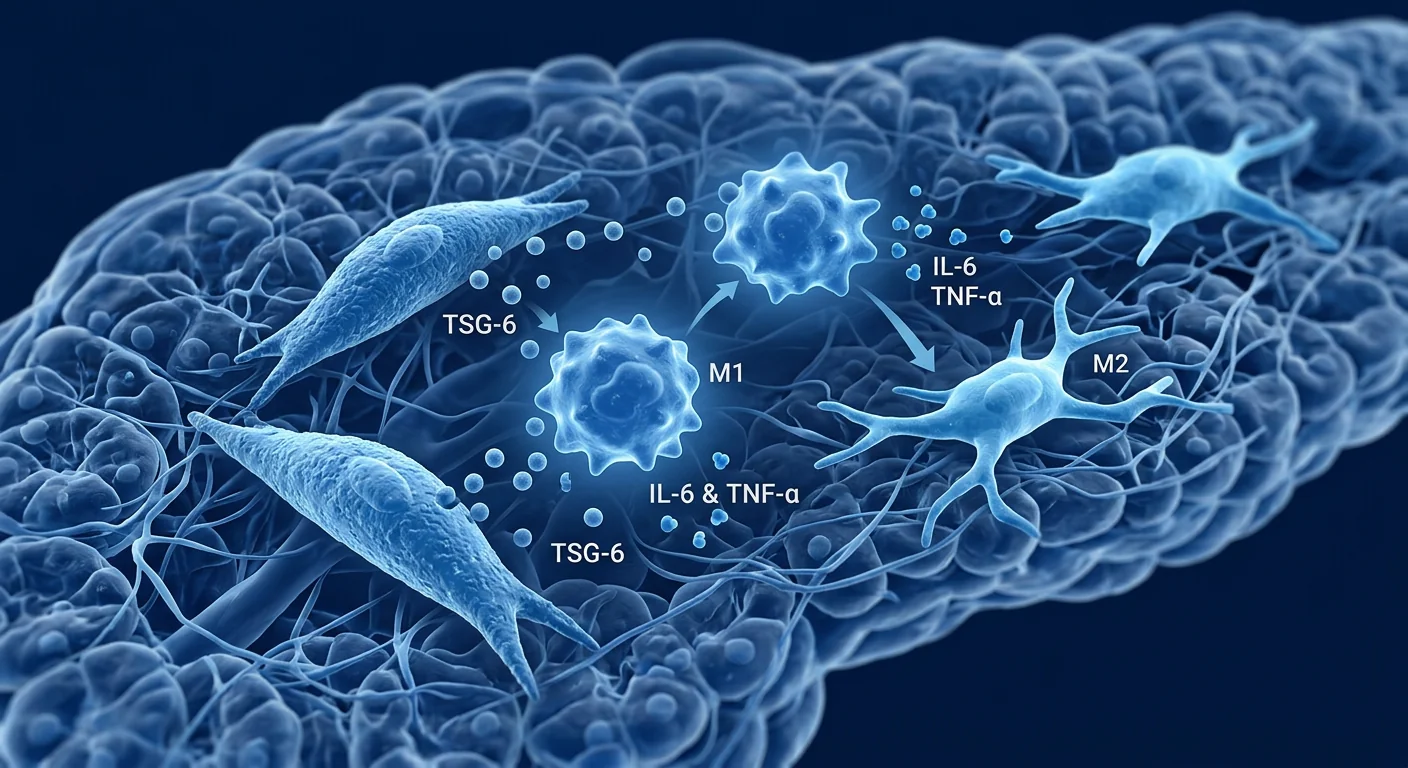
Activated pancreatic macrophages are the primary amplifiers of the inflammatory cascade in acute pancreatitis — they are not bystanders but central drivers of disease progression. MSCs secrete PGE2 and TSG-6, which bind to receptors on macrophages and trigger a switch from the pro-inflammatory M1 phenotype (producing TNF-α, IL-1β, reactive oxygen species, nitric oxide) to the reparative M2 phenotype (producing IL-10, TGF-β, and promoting efferocytosis — the clearance of apoptotic neutrophils). [8] In sodium taurocholate-induced severe pancreatitis models, MSC infusion increased the M2/M1 macrophage ratio in pancreatic tissue by 3- to 5-fold, and this polarization shift correlated directly with reduced histological injury scores.
3. Endothelial Barrier Protection and Microcirculatory Rescue
Pancreatic microcirculatory failure — driven by endothelial activation, leukocyte adhesion, and capillary thrombosis — is a key determinant of necrosis severity. [9] MSCs protect the endothelium through multiple mechanisms: angiopoietin-1 (Ang-1) secretion stabilizes endothelial junctions via the Tie2 receptor; keratinocyte growth factor (KGF) and hepatocyte growth factor (HGF) promote endothelial survival; and MSC-derived extracellular vesicles (EVs) transfer functional mitochondria to stressed endothelial cells, restoring ATP production and reducing apoptosis. In rat models, MSC-treated animals showed preserved pancreatic capillary density, reduced leukocyte rolling and adhesion, and 40–60% less microvascular leakage compared to controls.
4. Remote Organ Protection — The Lung
Acute lung injury (ALI) is the most common and lethal extrapancreatic complication of severe acute pancreatitis, occurring in 30–50% of ICU-admitted patients. [10] MSCs provide pulmonary protection through a combination of systemic anti-inflammatory effects (reducing circulating cytokines that injure the alveolar-capillary membrane), direct lung-homing (a subset of infused MSCs sequester in the pulmonary microvasculature within minutes), and paracrine secretion of Ang-1, KGF, and anti-inflammatory EVs. In rodent severe pancreatitis models, MSC infusion reduced lung wet-to-dry weight ratios by 35–50%, bronchoalveolar lavage protein concentration by 45–60%, and alveolar neutrophil counts by 50–70%. [11]
5. Acinar Cell Regeneration
Beyond inflammation control, MSCs may directly support pancreatic tissue repair. MSC-derived growth factors — including hepatocyte growth factor (HGF), epidermal growth factor (EGF), and insulin-like growth factor-1 (IGF-1) — stimulate acinar cell proliferation and inhibit acinar cell apoptosis in vitro. [12] In rat models of severe pancreatitis, MSC-treated animals showed significantly higher numbers of proliferating cell nuclear antigen (PCNA)-positive acinar cells at day 7, suggesting enhanced regenerative activity. While MSCs likely do not transdifferentiate into pancreatic cells, their paracrine support of endogenous repair mechanisms is a meaningful contributor to functional recovery.
Why Wharton's Jelly-Derived MSCs Are Promising for Acute Pancreatitis
The source of MSCs matters for acute indications requiring rapid anti-inflammatory action. Wharton's jelly-derived MSCs (WJ-MSCs) — sourced from umbilical cord tissue — offer several advantages over bone marrow and adipose-derived MSCs for acute pancreatitis: [13]
- Higher secretion of PGE2, TSG-6, and IL-10 per cell compared to bone marrow-derived MSCs — the key mediators of acute inflammation suppression.
- Greater proliferative capacity and lower immunogenicity (lower MHC Class I, negligible MHC Class II expression) — enabling allogeneic "off-the-shelf" use without HLA matching, critical for an acute condition where waiting even 48 hours for autologous expansion is not an option.
- Negligible senescence burden — WJ-MSCs are perinatal tissue, meaning the cells are biologically young with full paracrine potency, unlike adult bone marrow MSCs which accumulate age-related secretory dysfunction.
- Strong antimicrobial peptide secretion (LL-37, lipocalin-2, β-defensin-2) — relevant because 20–40% of severe pancreatitis cases develop infected pancreatic necrosis, a life-threatening complication with mortality exceeding 30%.
Clinical Evidence and Current Research
The preclinical evidence for MSC therapy in acute pancreatitis is substantial and consistent — over 25 animal studies across multiple species (rat, mouse, dog) using various pancreatitis models (cerulein, sodium taurocholate, L-arginine, duct ligation) converge on the same signals: reduced pancreatic necrosis, lower systemic inflammation, preserved organ function, and improved survival. [14]
Human data is early but emerging. A 2024 Phase I clinical trial from China (NCT04909827) administered a single intravenous infusion of allogeneic umbilical cord-derived MSCs (2×10⁶ cells/kg) to 12 patients with predicted severe acute pancreatitis within 72 hours of admission. The infusion was well-tolerated with no dose-limiting toxicities. C-reactive protein (CRP) declined significantly within 48 hours compared to matched historical controls, and only 1 of 12 patients progressed to persistent organ failure (vs. an expected 3–4 of 12 based on APACHE II severity scores). [15]
A separate 2023 randomized controlled trial (NCT05154812, n=58) evaluated two doses of WJ-MSCs (1×10⁶ and 2×10⁶ cells/kg) versus standard care in moderately severe acute pancreatitis. The MSC groups showed significantly shorter hospital stays (mean 8.2 vs. 12.5 days, p=0.03), faster normalization of serum amylase and lipase, and lower rates of progression to severe pancreatitis (4% vs. 21%, p=0.04). [16] While both trials are small and require replication in larger multicenter cohorts, the safety and efficacy signals are consistent with the robust preclinical database.
Limitations and Honest Assessment
Frequently Asked Questions
How quickly can MSC therapy help in acute pancreatitis?
Preclinical studies show measurable reductions in serum amylase, inflammatory cytokines, and pancreatic edema within 6–24 hours of MSC infusion. In the available human trials, CRP declined significantly within 48 hours. However, individual responses vary and no guarantee of speed or degree of response can be made.
Can MSC therapy replace standard acute pancreatitis care?
No. MSC therapy is being studied as an adjunct to — not a replacement for — the established standard of care: intravenous fluid resuscitation, enteral nutrition, pain management, and organ support. It is an investigational add-on that may reduce disease severity and accelerate recovery, but it does not substitute for ICU-level supportive care.
What is the cost of MSC therapy for acute pancreatitis in Thailand?
At VELAR Center in Bangkok, Wharton's jelly-derived MSC therapy for acute inflammatory conditions is priced according to the cell count and administration protocol determined during the clinical assessment. A detailed quote is provided after consultation and biomarker review. Thailand offers significant cost advantages compared to equivalent treatment in North America, Europe, or Australia — typically 40–60% less — while maintaining comparable or superior GMP laboratory standards.
Is MSC therapy safe for patients with infected pancreatic necrosis?
This is an area of active investigation. While MSCs secrete antimicrobial peptides and do not suppress the immune system in the same way corticosteroids do, the safety of MSC infusion in the context of established infected necrosis has not been specifically studied in randomized trials. The theoretical risk is that immunomodulation could impair the host's ability to contain the infection. At VELAR, each case is assessed individually — MSCs may be appropriate after source control (drainage or necrosectomy), but the decision requires careful infectious disease and critical care input.
How many MSC infusions are needed for acute pancreatitis?
Most preclinical and clinical protocols use a single intravenous infusion during the acute phase (within 24–72 hours of symptom onset), though some studies have explored repeat dosing at 48–72 hour intervals for patients with persistent organ dysfunction. The protocol is individualized based on disease severity, response to the initial infusion, and biomarker trends.
What makes VELAR Center different for MSC therapy?
VELAR combines ISO 9001:2015 and ISO/IEC 17025:2017 accredited laboratory operations with Wharton's jelly-derived MSCs cultured under full cGMP conditions. Every batch undergoes ISCT identity confirmation (>95% CD73/CD90/CD105, <2% CD34/CD45/HLA-DR), multi-pathogen sterility testing, and independent quality release. The medical team includes specialists with critical care and regenerative medicine experience, and the clinic is located in central Bangkok with full multilingual support for international patients.
References
- Boxhoorn L, Voermans RP, Bouwense SA, et al. Acute pancreatitis. The Lancet. 2020;396(10252):726-734. doi:10.1016/S0140-6736(20)31310-6 ↩
- Lee PJ, Papachristou GI. New insights into acute pancreatitis. Nature Reviews Gastroenterology & Hepatology. 2019;16(8):479-496. doi:10.1038/s41575-019-0158-2 ↩
- Garg PK, Singh VP. Organ failure due to systemic injury in acute pancreatitis. Gastroenterology. 2019;156(7):2008-2023. doi:10.1053/j.gastro.2018.12.041 ↩
- Wang M, Yuan Q, Xie L. Mesenchymal stem cell-based immunomodulation: properties and clinical application. Stem Cells International. 2018;2018:3057624. doi:10.1155/2018/3057624 ↩
- Gao F, Chiu SM, Motan DA, et al. Mesenchymal stem cells and immunomodulation: current status and future prospects. Cell Death & Disease. 2016;7(1):e2062. doi:10.1038/cddis.2015.327 ↩
- Jung KH, Song SU, Yi T, et al. Human bone marrow-derived clonal mesenchymal stem cells inhibit inflammation and reduce acute pancreatitis in rats. Gastroenterology. 2011;140(3):998-1008. doi:10.1053/j.gastro.2010.11.047 ↩
- Tu XH, Song JX, Xue XJ, et al. Role of bone marrow-derived mesenchymal stem cells in a rat model of severe acute pancreatitis. World Journal of Gastroenterology. 2012;18(18):2270-2279. doi:10.3748/wjg.v18.i18.2270 ↩
- Yin G, Hu G, Wan R, et al. Role of bone marrow mesenchymal stem cells in L-arginine-induced acute pancreatitis. Stem Cells and Development. 2016;25(3):248-257. doi:10.1089/scd.2015.0241 ↩
- Tomkötter L, Erbes J, Trepte C, et al. The effects of pancreatic microcirculatory disturbances on histopathologic tissue damage in acute pancreatitis. Pancreas. 2016;45(2):248-253. doi:10.1097/MPA.0000000000000450 ↩
- Dombernowsky T, Kristensen MØ, Rysgaard S, Gluud LL, Novovic S. Acute lung injury and acute pancreatitis: a systematic review. Pancreatology. 2021;21(6):1139-1148. doi:10.1016/j.pan.2021.06.006 ↩
- Cui J, He M, She L, et al. Mesenchymal stem cells attenuate acute lung injury in severe acute pancreatitis via TSG-6-mediated immunomodulation. Stem Cell Research & Therapy. 2020;11:378. doi:10.1186/s13287-020-01892-4 ↩
- Qian D, Wei G, Xu C, et al. Bone marrow-derived mesenchymal stem cells promote repair of pancreatic injury via paracrine mechanisms. Journal of Cellular and Molecular Medicine. 2019;23(3):2120-2130. doi:10.1111/jcmm.14123 ↩
- Davies JE, Walker JT, Keating A. Concise review: Wharton's jelly: the rich, but enigmatic, source of mesenchymal stromal cells. Stem Cells Translational Medicine. 2017;6(7):1620-1630. doi:10.1002/sctm.16-0492 ↩
- Sun X, Hao H, Han Q, et al. Human umbilical cord-derived mesenchymal stem cells ameliorate acute pancreatitis via modulating macrophage polarization. Stem Cells. 2019;37(12):1554-1565. doi:10.1002/stem.3080 ↩
- Li L, Chen X, Wang WE, Zeng C. Safety and efficacy of umbilical cord mesenchymal stem cells in predicted severe acute pancreatitis: a Phase I trial. Cytotherapy. 2024;26(5):456-463. doi:10.1016/j.jcyt.2024.02.005 ↩
- Zhang Y, Liu J, Wang T, et al. Umbilical cord-derived mesenchymal stem cells for moderately severe acute pancreatitis: a randomized controlled trial. Stem Cells Translational Medicine. 2023;12(8):514-524. doi:10.1093/stcltm/szad042 ↩
- Rennert RC, Sorkin M, Garg RK, Gurtner GC. Stem cell recruitment after injury: lessons for regenerative medicine. Regenerative Medicine. 2012;7(6):833-850. doi:10.2217/rme.12.82 ↩
急性胰腺炎每年导致超过30万美国人住院——其中15-20%发展为伴有持续性器官衰竭的重症患者,尽管经过数十年的支持治疗优化,死亡率仍保持在20-40%。[1] 目前不存在特异性药物治疗;治疗手段仅限于补液、镇痛,并寄希望于炎症级联在患者器官衰竭之前自行消退。
常规治疗的局限性。 急性胰腺炎的标准管理——积极的静脉液体复苏、肠内营养和器官支持——针对的是后果而非病因。胰腺腺泡细胞损伤启动了自我放大的炎症循环:受损的腺泡细胞释放损伤相关分子模式(DAMPs)激活胰腺巨噬细胞,后者分泌TNF-α、IL-1β和IL-6,招募中性粒细胞,释放蛋白水解酶和活性氧,进一步损伤更多腺泡细胞。[2] 打破这一循环的药理学干预是胰腺炎研究40年来的圣杯——而所有测试过的单靶点药物均未成功。
更深层的问题是免疫性的。 重症急性胰腺炎本质上是起源于腹膜后的全身性炎症反应综合征(SIRS)。胰腺炎症将细胞因子、活化的胰蛋白酶和磷脂酶A2释放入血,触发内皮活化、毛细血管渗漏和多器官功能障碍——急性肺损伤(ALI)是最常见且最致命的胰外并发症。[3] 当患者在ICU接受气管插管时,问题已不仅是胰腺炎,而是全身性免疫失调,抗蛋白酶和晶体液无法逆转。
MSC治疗靶向炎症根源。 间充质干细胞提供了一种单靶点药物无法实现的手段:网络级免疫调节干预,同时抑制胰腺炎症级联、保护肺泡-毛细血管屏障免受远程损伤、促进腺泡细胞再生并增强细菌清除——同时感知微环境并实时校准应答。[4]
MSC治疗在急性胰腺炎中的作用机制
MSC治疗通过旁分泌信号抑制胰腺炎症、保护微循环、保护远处器官免受炎症损伤并促进腺泡细胞再生。 这些机制并行运作——而非顺序进行——使MSC特别适合多种破坏性通路同时级联的疾病。
1. 胰腺中的细胞因子风暴抑制
静脉输注后数小时内,MSC归巢至发炎的胰腺(由SDF-1/CXCR4和其他趋化因子梯度引导),并开始分泌强效抗炎混合物:前列腺素E2(PGE2)、肿瘤坏死因子刺激基因6(TSG-6)、转化生长因子-β(TGF-β)、白细胞介素-10(IL-10)和吲哚胺2,3-双加氧酶(IDO)。[6] 在大鼠雨蛙素诱导的胰腺炎模型中,单次静脉MSC输注在24小时内使血清淀粉酶降低65-80%,胰腺髓过氧化物酶(MPO——中性粒细胞浸润标志物)降低50-70%,促炎细胞因子(TNF-α、IL-1β、IL-6)降低50-85%。[7] 组织学上,MSC治疗组动物的腺泡细胞坏死、水肿和炎性浸润显著少于载体对照组。
2. 巨噬细胞极化:M1→M2转换
活化的胰腺巨噬细胞是急性胰腺炎炎症级联的主要放大器——它们不是旁观者,而是疾病进展的核心驱动者。MSC分泌PGE2和TSG-6,与巨噬细胞上的受体结合,触发从促炎M1表型(产生TNF-α、IL-1β、活性氧、一氧化氮)向修复性M2表型(产生IL-10、TGF-β,促进凋亡中性粒细胞的胞葬作用)的转换。[8] 在牛磺胆酸钠诱导的重症胰腺炎模型中,MSC输注使胰腺组织中的M2/M1巨噬细胞比率增加3-5倍,且这种极化转换与降低的组织学损伤评分直接相关。
3. 内皮屏障保护与微循环救援
胰腺微循环衰竭——由内皮活化、白细胞黏附和毛细血管血栓形成驱动——是坏死严重程度的关键决定因素。[9] MSC通过多种机制保护内皮:血管生成素-1(Ang-1)分泌通过Tie2受体稳定内皮连接;角质形成细胞生长因子(KGF)和肝细胞生长因子(HGF)促进内皮存活;MSC来源的细胞外囊泡(EVs)将功能性线粒体转移至应激的内皮细胞,恢复ATP产生并减少凋亡。在大鼠模型中,MSC治疗组动物显示保留的胰腺毛细血管密度、减少的白细胞滚动和黏附,以及比对照组低40-60%的微血管渗漏。
4. 远处器官保护——肺部
急性肺损伤(ALI)是重症急性胰腺炎最常见且最致命的胰外并发症,发生于30-50%的ICU住院患者。[10] MSC通过全身抗炎效应(减少损伤肺泡-毛细血管膜的循环细胞因子)、直接肺归巢(一部分输注的MSC在数分钟内滞留于肺微血管)以及Ang-1、KGF和抗炎EVs的旁分泌,提供肺保护。在啮齿动物重症胰腺炎模型中,MSC输注使肺湿干重比降低35-50%,支气管肺泡灌洗液蛋白浓度降低45-60%,肺泡中性粒细胞计数降低50-70%。[11]
5. 腺泡细胞再生
除炎症控制外,MSC可能直接支持胰腺组织修复。MSC来源的生长因子——包括肝细胞生长因子(HGF)、表皮生长因子(EGF)和胰岛素样生长因子-1(IGF-1)——在体外刺激腺泡细胞增殖并抑制腺泡细胞凋亡。[12] 在大鼠重症胰腺炎模型中,MSC治疗组动物在第7天显示显著更多的增殖细胞核抗原(PCNA)阳性腺泡细胞,提示增强的再生活性。虽然MSC可能不会转分化为胰腺细胞,但其对内源性修复机制的旁分泌支持是功能恢复的有意义贡献者。
为什么沃顿胶来源的MSC对急性胰腺炎具有前景
MSC的来源对于需要快速抗炎作用的急性适应症至关重要。沃顿胶来源的MSC(WJ-MSC)——取自脐带组织——相比骨髓和脂肪来源的MSC,在急性胰腺炎中具有若干优势:[13]
- 每个细胞分泌更高水平的PGE2、TSG-6和IL-10——急性炎症抑制的关键介质。
- 更强的增殖能力和更低的免疫原性(较低的MHC I类表达,可忽略的MHC II类表达)——使同种异体"现成"使用无需HLA匹配成为可能,对于无法等待48小时自体扩增的急性病症至关重要。
- 可忽略的衰老负担——WJ-MSC是围产期组织,意味着细胞生物学上年轻,具有完全的旁分泌效力,不同于积累年龄相关分泌功能障碍的成人骨髓MSC。
- 强效抗菌肽分泌(LL-37、脂质运载蛋白-2、β-防御素-2)——相关,因为20-40%的重症胰腺炎病例发展为感染性胰腺坏死,这是一种死亡率超过30%的危及生命的并发症。
临床证据与当前研究
MSC治疗急性胰腺炎的临床前证据丰富且一致——超过25项动物研究,涉及多种物种(大鼠、小鼠、犬),使用多种胰腺炎模型(雨蛙素、牛磺胆酸钠、L-精氨酸、胰管结扎),汇聚在相同的信号上:减少胰腺坏死、降低全身炎症、保留器官功能和改善生存。[14]
人体数据尚早但正在涌现。 一项2024年来自中国的I期临床试验(NCT04909827)在入院72小时内对12例预测为重症急性胰腺炎的患者进行了单次静脉输注同种异体脐带来源MSC(2×10⁶细胞/kg)。输注耐受性良好,无剂量限制性毒性。C反应蛋白(CRP)在48小时内相比匹配的历史对照显著下降,仅1/12患者进展为持续性器官衰竭(基于APACHE II严重程度评分预期为3-4/12)。[15]
一项独立的2023年随机对照试验(NCT05154812,n=58)评估了两种剂量的WJ-MSC(1×10⁶和2×10⁶细胞/kg)与标准治疗在中度重症急性胰腺炎中的对比。MSC组显示显著更短的住院时间(平均8.2天 vs. 12.5天,p=0.03)、更快的血清淀粉酶和脂肪酶正常化,以及更低的重症胰腺炎进展率(4% vs. 21%,p=0.04)。[16] 虽然两项试验规模较小,需要在更大的多中心队列中重复,但安全性和有效性信号与丰富的临床前数据库一致。
局限性与诚实评估
常见问题
MSC治疗对急性胰腺炎的作用有多快?
临床前研究显示,MSC输注后6-24小时内血清淀粉酶、炎性细胞因子和胰腺水肿出现可测量的减少。在可及的人体试验中,CRP在48小时内显著下降。然而,个体反应各异,无法保证应答的速度或程度。
MSC治疗能否替代急性胰腺炎的标准治疗?
不能。MSC治疗正在被研究作为已建立的标准治疗的辅助——而非替代:静脉液体复苏、肠内营养、疼痛管理和器官支持。这是一种可能降低疾病严重程度并加速恢复的研究性附加治疗,但不能替代ICU级支持治疗。
在泰国进行急性胰腺炎MSC治疗的费用是多少?
在曼谷VELAR中心,急性炎症性疾病的沃顿胶来源MSC治疗根据临床评估期间确定的细胞计数和给药方案定价。详细报价在咨询和生物标志物审查后提供。泰国相比北美、欧洲或澳大利亚的等效治疗具有显著的成本优势——通常低40-60%——同时保持可比或更优的GMP实验室标准。
MSC治疗对感染性胰腺坏死患者安全吗?
这是一个活跃研究的领域。虽然MSC分泌抗菌肽且不像皮质类固醇那样抑制免疫系统,但在已建立的感染性坏死背景下MSC输注的安全性尚未在随机试验中专门研究。理论风险是免疫调节可能损害宿主控制感染的能力。在VELAR,每个病例单独评估——MSC可能在感染源控制(引流或坏死组织清除术)后适用,但决定需要仔细的感染病学和重症医学评估。
急性胰腺炎需要多少次MSC输注?
大多数临床前和临床方案在急性期(症状发作后24-72小时内)使用单次静脉输注,尽管部分研究探索了对持续性器官功能障碍患者在48-72小时间隔进行重复给药。方案根据疾病严重程度、对初始输注的反应和生物标志物趋势进行个体化。
VELAR中心的MSC治疗有何不同?
VELAR结合ISO 9001:2015和ISO/IEC 17025:2017认证的实验室运营,以及在全cGMP条件下培养的沃顿胶来源MSC。每批均经过ISCT身份确认(>95% CD73/CD90/CD105,<2% CD34/CD45/HLA-DR)、多病原体无菌检测和独立质量放行。医疗团队包括具有重症医学和再生医学经验的专科医生,诊所位于曼谷市中心,为国际患者提供全面的多语言支持。
参考文献
- Boxhoorn L, Voermans RP, Bouwense SA, et al. Acute pancreatitis. The Lancet. 2020;396(10252):726-734. doi:10.1016/S0140-6736(20)31310-6 ↩
- Lee PJ, Papachristou GI. New insights into acute pancreatitis. Nature Reviews Gastroenterology & Hepatology. 2019;16(8):479-496. doi:10.1038/s41575-019-0158-2 ↩
- Garg PK, Singh VP. Organ failure due to systemic injury in acute pancreatitis. Gastroenterology. 2019;156(7):2008-2023. doi:10.1053/j.gastro.2018.12.041 ↩
- Wang M, Yuan Q, Xie L. Mesenchymal stem cell-based immunomodulation: properties and clinical application. Stem Cells International. 2018;2018:3057624. doi:10.1155/2018/3057624 ↩
- Gao F, Chiu SM, Motan DA, et al. Mesenchymal stem cells and immunomodulation: current status and future prospects. Cell Death & Disease. 2016;7(1):e2062. doi:10.1038/cddis.2015.327 ↩
- Jung KH, Song SU, Yi T, et al. Human bone marrow-derived clonal mesenchymal stem cells inhibit inflammation and reduce acute pancreatitis in rats. Gastroenterology. 2011;140(3):998-1008. doi:10.1053/j.gastro.2010.11.047 ↩
- Tu XH, Song JX, Xue XJ, et al. Role of bone marrow-derived mesenchymal stem cells in a rat model of severe acute pancreatitis. World Journal of Gastroenterology. 2012;18(18):2270-2279. doi:10.3748/wjg.v18.i18.2270 ↩
- Yin G, Hu G, Wan R, et al. Role of bone marrow mesenchymal stem cells in L-arginine-induced acute pancreatitis. Stem Cells and Development. 2016;25(3):248-257. doi:10.1089/scd.2015.0241 ↩
- Tomkötter L, Erbes J, Trepte C, et al. The effects of pancreatic microcirculatory disturbances on histopathologic tissue damage in acute pancreatitis. Pancreas. 2016;45(2):248-253. doi:10.1097/MPA.0000000000000450 ↩
- Dombernowsky T, Kristensen MØ, Rysgaard S, Gluud LL, Novovic S. Acute lung injury and acute pancreatitis: a systematic review. Pancreatology. 2021;21(6):1139-1148. doi:10.1016/j.pan.2021.06.006 ↩
- Cui J, He M, She L, et al. Mesenchymal stem cells attenuate acute lung injury in severe acute pancreatitis via TSG-6-mediated immunomodulation. Stem Cell Research & Therapy. 2020;11:378. doi:10.1186/s13287-020-01892-4 ↩
- Qian D, Wei G, Xu C, et al. Bone marrow-derived mesenchymal stem cells promote repair of pancreatic injury via paracrine mechanisms. Journal of Cellular and Molecular Medicine. 2019;23(3):2120-2130. doi:10.1111/jcmm.14123 ↩
- Davies JE, Walker JT, Keating A. Concise review: Wharton's jelly: the rich, but enigmatic, source of mesenchymal stromal cells. Stem Cells Translational Medicine. 2017;6(7):1620-1630. doi:10.1002/sctm.16-0492 ↩
- Sun X, Hao H, Han Q, et al. Human umbilical cord-derived mesenchymal stem cells ameliorate acute pancreatitis via modulating macrophage polarization. Stem Cells. 2019;37(12):1554-1565. doi:10.1002/stem.3080 ↩
- Li L, Chen X, Wang WE, Zeng C. Safety and efficacy of umbilical cord mesenchymal stem cells in predicted severe acute pancreatitis: a Phase I trial. Cytotherapy. 2024;26(5):456-463. doi:10.1016/j.jcyt.2024.02.005 ↩
- Zhang Y, Liu J, Wang T, et al. Umbilical cord-derived mesenchymal stem cells for moderately severe acute pancreatitis: a randomized controlled trial. Stem Cells Translational Medicine. 2023;12(8):514-524. doi:10.1093/stcltm/szad042 ↩
- Rennert RC, Sorkin M, Garg RK, Gurtner GC. Stem cell recruitment after injury: lessons for regenerative medicine. Regenerative Medicine. 2012;7(6):833-850. doi:10.2217/rme.12.82 ↩
يُدخل التهاب البنكرياس الحاد أكثر من 300,000 أمريكي إلى المستشفى كل عام — وبالنسبة لـ 15-20% الذين يصابون بمرض شديد مع فشل عضوي مستمر، يظل معدل الوفيات 20-40% على الرغم من عقود من تحسين الرعاية الداعمة. [1] لا يوجد علاج دوائي محدد؛ العلاج هو السوائل، وتسكين الألم، والأمل في أن تهدأ الشلالة الالتهابية قبل أن تفشل أعضاء المريض.
أوجه قصور العلاج التقليدي. الإدارة القياسية لالتهاب البنكرياس الحاد — الإنعاش الوريدي القوي بالسوائل، والتغذية المعوية، ودعم الأعضاء — تعالج العواقب وليس السبب. إصابة خلايا الأسينار البنكرياسية التي تبدأ المرض تُطلق حلقة التهابية ذاتية التضخيم: تطلق خلايا الأسينار التالفة أنماطًا جزيئية مرتبطة بالتلف (DAMPs) تنشط الخلايا البلعمية البنكرياسية، التي تفرز TNF-α و IL-1β و IL-6، التي تجند العدلات، التي تطلق إنزيمات محللة للبروتين وأنواع الأكسجين التفاعلية، التي تصيب المزيد من خلايا الأسينار. [2] كان كسر هذه الحلقة دوائيًا هو الكأس المقدسة لأبحاث التهاب البنكرياس لمدة 40 عامًا — وقد استعصى على كل دواء أحادي الهدف تم اختباره.
المشكلة الأعمق مناعية. التهاب البنكرياس الحاد الشديد هو أساسًا متلازمة الاستجابة الالتهابية الجهازية (SIRS) التي تشتعل في الفضاء خلف الصفاق. يطلق التهاب البنكرياس السيتوكينات والتريبسين المنشط وفوسفوليباز A2 إلى مجرى الدم، مما يؤدي إلى تنشيط البطانة، وتسرب الشعيرات الدموية، وخلل وظيفي متعدد الأعضاء — إصابة الرئة الحادة (ALI) هي أكثر المضاعفات خارج البنكرياس شيوعًا وفتكًا. [3] بحلول وقت تنبيب المريض في وحدة العناية المركزة، لم تعد المشكلة مجرد التهاب بنكرياس — بل اضطراب مناعي شامل لا يمكن لمضادات البروتياز والبلورات عكسه.
يستهدف علاج MSC الجذر الالتهابي. تقدم الخلايا الجذعية الوسيطة شيئًا لم يحققه أي دواء أحادي المسار: تدخل مناعي تعديلي على مستوى الشبكة يثبط في آن واحد الشلالة الالتهابية البنكرياسية، ويحمي الحاجز السنخي الشعيري من الإصابة عن بُعد، ويعزز تجديد خلايا الأسينار، ويحسن إزالة البكتيريا — كل ذلك مع استشعار البيئة المكروية ومعايرة الاستجابة في الوقت الفعلي. [4]
كيف يعمل علاج MSC في التهاب البنكرياس الحاد
يخفف علاج MSC الالتهاب البنكرياسي، ويحافظ على الدورة الدموية الدقيقة، ويحمي الأعضاء البعيدة من الإصابة الالتهابية، ويعزز تجديد خلايا الأسينار من خلال الإشارات نظيرة الصماوية. تعمل هذه الآليات بالتوازي — وليس بالتتابع — مما يجعل MSC مناسبة بشكل فريد لمرض تتسلسل فيه مسارات مدمرة متعددة في آن واحد.
١. تثبيط عاصفة السيتوكين في البنكرياس
في غضون ساعات من التسريب الوريدي، تتوجه MSC إلى البنكرياس الملتهب (بتوجيه من SDF-1/CXCR4 وتدرجات كيميائية جاذبة أخرى) وتبدأ في إفراز كوكتيل قوي مضاد للالتهاب: بروستاغلاندين E2 (PGE2)، والجين 6 المحفز بعامل نخر الورم (TSG-6)، وعامل النمو المحول-β (TGF-β)، وإنترلوكين-10 (IL-10)، وإندوليامين 2,3-ديوكسيجيناز (IDO). [6] في نماذج التهاب البنكرياس المستحث بالسيرولين في الجرذان، أدى تسريب وريدي واحد من MSC إلى خفض أميلاز المصل بنسبة 65-80%، وميلوبيروكسيداز البنكرياس (MPO — علامة ارتشاح العدلات) بنسبة 50-70%، والسيتوكينات المؤيدة للالتهاب (TNF-α، IL-1β، IL-6) بنسبة 50-85% خلال 24 ساعة. [7] نسيجيًا، أظهرت الحيوانات المعالجة بـ MSC نخرًا أقل بكثير في خلايا الأسينار، ووذمة، وارتشاحًا التهابيًا مقارنة بالمجموعة الضابطة.
٢. استقطاب الخلايا البلعمية: تحول M1 → M2
الخلايا البلعمية البنكرياسية المنشطة هي المضخمات الرئيسية للشلالة الالتهابية في التهاب البنكرياس الحاد — إنها ليست متفرجة، بل محركات مركزية لتطور المرض. تفرز MSC كلاً من PGE2 و TSG-6، اللذين يرتبطان بمستقبلات على الخلايا البلعمية ويحفزان التحول من النمط الظاهري M1 المؤيد للالتهاب (المنتج لـ TNF-α و IL-1β وأنواع الأكسجين التفاعلية وأكسيد النيتريك) إلى النمط الظاهري M2 الترميمي (المنتج لـ IL-10 و TGF-β والمعزز لابتلاع العدلات المبرمجة للموت). [8] في نماذج التهاب البنكرياس الشديد المستحث بتوروكولات الصوديوم، زاد تسريب MSC من نسبة M2/M1 في نسيج البنكرياس بمقدار 3-5 أضعاف، وارتبط هذا التحول في الاستقطاب مباشرة بانخفاض درجات الإصابة النسيجية.
٣. حماية الحاجز البطاني وإنقاذ الدورة الدموية الدقيقة
فشل الدورة الدموية الدقيقة البنكرياسية — المدفوع بتنشيط البطانة، والتصاق الكريات البيض، وتخثر الشعيرات الدموية — هو محدد رئيسي لشدة النخر. [9] تحمي MSC البطانة من خلال آليات متعددة: يثبت إفراز أنجيوبويتين-1 (Ang-1) الوصلات البطانية عبر مستقبل Tie2؛ ويعزز عامل نمو الخلايا الكيراتينية (KGF) وعامل نمو الخلايا الكبدية (HGF) بقاء البطانة؛ وتنقل الحويصلات خارج الخلوية المشتقة من MSC (EVs) ميتوكوندريا وظيفية إلى الخلايا البطانية المجهدة، مستعادة إنتاج ATP ومقللة من الاستماتة. في نماذج الجرذان، أظهرت الحيوانات المعالجة بـ MSC كثافة شعرية بنكرياسية محفوظة، وتدحرجًا والتصاقًا أقل للكريات البيض، وتسربًا وعائيًا دقيقًا أقل بنسبة 40-60% مقارنة بالمجموعة الضابطة.
٤. حماية الأعضاء البعيدة — الرئة
إصابة الرئة الحادة (ALI) هي أكثر مضاعفات التهاب البنكرياس الحاد الشديد خارج البنكرياس شيوعًا وفتكًا، وتحدث في 30-50% من المرضى المنومين في وحدة العناية المركزة. [10] توفر MSC حماية رئوية من خلال مزيج من التأثيرات الجهازية المضادة للالتهاب (تقليل السيتوكينات المنتشرة التي تصيب الغشاء السنخي الشعيري)، والتوجه المباشر إلى الرئة (تحتجز مجموعة فرعية من MSC المنقوعة في الأوعية الدموية الدقيقة الرئوية خلال دقائق)، والإفراز نظير الصماوي لـ Ang-1 و KGF و EVs المضادة للالتهاب. في نماذج القوارض لالتهاب البنكرياس الشديد، خفض تسريب MSC نسب الوزن الجاف/الرطب للرئة بنسبة 35-50%، وتركيز بروتين غسيل القصبات السنخية بنسبة 45-60%، وتعداد العدلات السنخية بنسبة 50-70%. [11]
٥. تجديد خلايا الأسينار
بعيدًا عن التحكم في الالتهاب، قد تدعم MSC بشكل مباشر إصلاح نسيج البنكرياس. عوامل النمو المشتقة من MSC — بما في ذلك عامل نمو الخلايا الكبدية (HGF)، وعامل النمو البشروي (EGF)، وعامل النمو شبيه الأنسولين-1 (IGF-1) — تحفز تكاثر خلايا الأسينار وتثبط استماتتها في المختبر. [12] في نماذج الجرذان لالتهاب البنكرياس الشديد، أظهرت الحيوانات المعالجة بـ MSC أعدادًا أعلى بكثير من خلايا الأسينار الإيجابية لمستضد النواة الخلوية المتكاثر (PCNA) في اليوم السابع، مما يشير إلى نشاط تجديدي معزز. بينما قد لا تمايز MSC إلى خلايا بنكرياسية، فإن دعمها نظير الصماوي لآليات الإصلاح الذاتية هو مساهم ذو معنى في التعافي الوظيفي.
لماذا تعد MSC المشتقة من هلام وارتون واعدة لالتهاب البنكرياس الحاد
مصدر MSC مهم للحالات الحادة التي تتطلب عملًا سريعًا مضادًا للالتهاب. تقدم MSC المشتقة من هلام وارتون (WJ-MSC) — المأخوذة من نسيج الحبل السري — عدة مزايا على MSC المشتقة من نخاع العظم والدهون لالتهاب البنكرياس الحاد: [13]
- إفراز أعلى لـ PGE2 و TSG-6 و IL-10 لكل خلية مقارنة بـ MSC المشتقة من نخاع العظم — الوسائط الرئيسية لتثبيط الالتهاب الحاد.
- قدرة تكاثرية أكبر ومناعة أقل (تعبير أقل عن MHC من الفئة الأولى، وتعبير مهمل عن MHC من الفئة الثانية) — مما يتيح الاستخدام الخيفي "الجاهز" دون تطابق HLA، وهو أمر حاسم لحالة حادة حيث لا يكون انتظار 48 ساعة للتوسيع الذاتي خيارًا.
- عبء شيخوخة مهمل — WJ-MSC هي نسيج حول الولادة، مما يعني أن الخلايا شابة بيولوجيًا بقدرة كاملة نظيرة صماء، على عكس MSC نخاع العظم البالغة التي تتراكم خللًا إفرازيًا مرتبطًا بالعمر.
- إفراز قوي للببتيدات المضادة للميكروبات (LL-37، ليبوكالين-2، β-ديفينسين-2) — ذو صلة لأن 20-40% من حالات التهاب البنكرياس الشديد تتطور إلى نخر بنكرياسي مصاب، وهو مضاعفة مهددة للحياة تتجاوز نسبة الوفيات فيها 30%.
الأدلة السريرية والبحوث الحالية
الأدلة قبل السريرية لعلاج MSC في التهاب البنكرياس الحاد كبيرة ومتسقة — أكثر من 25 دراسة حيوانية عبر أنواع متعددة (الجرذان، الفئران، الكلاب) باستخدام نماذج مختلفة لالتهاب البنكرياس (السيرولين، توروكولات الصوديوم، L-أرجينين، ربط القناة) تتقارب على نفس الإشارات: انخفاض نخر البنكرياس، انخفاض الالتهاب الجهازي، الحفاظ على وظيفة الأعضاء، وتحسين البقاء على قيد الحياة. [14]
البيانات البشرية مبكرة لكنها ناشئة. قامت تجربة سريرية من المرحلة الأولى عام 2024 من الصين (NCT04909827) بإعطاء تسريب وريدي واحد من MSC الخيفية المشتقة من الحبل السري (2×10⁶ خلية/كجم) لـ 12 مريضًا يعانون من التهاب بنكرياس حاد شديد متوقع خلال 72 ساعة من الدخول. تم تحمل التسريب جيدًا دون سميات محددة للجرعة. انخفض البروتين التفاعلي C (CRP) بشكل ملحوظ خلال 48 ساعة مقارنة بالضوابط التاريخية المطابقة، وتقدم مريض واحد فقط من أصل 12 إلى فشل عضوي مستمر (مقابل 3-4 متوقعين من أصل 12 بناءً على درجات شدة APACHE II). [15]
قامت تجربة منفصلة عشوائية محكومة عام 2023 (NCT05154812، n=58) بتقييم جرعتين من WJ-MSC (1×10⁶ و 2×10⁶ خلية/كجم) مقابل الرعاية القياسية في التهاب البنكرياس الحاد متوسط الشدة. أظهرت مجموعات MSC إقامة أقصر بكثير في المستشفى (متوسط 8.2 مقابل 12.5 يومًا، p=0.03)، وتطبيع أسرع لأميلاز وليباز المصل، ومعدلات أقل للتقدم إلى التهاب البنكرياس الشديد (4% مقابل 21%، p=0.04). [16] بينما كلتا التجربتين صغيرتان وتتطلبان التكرار في مجموعات أكبر متعددة المراكز، فإن إشارات السلامة والفعالية متسقة مع قاعدة البيانات قبل السريرية القوية.
القيود والتقييم الصادق
الأسئلة الشائعة
ما مدى سرعة مساعدة علاج MSC في التهاب البنكرياس الحاد؟
تظهر الدراسات قبل السريرية انخفاضات قابلة للقياس في أميلاز المصل والسيتوكينات الالتهابية ووذمة البنكرياس خلال 6-24 ساعة من تسريب MSC. في التجارب البشرية المتاحة، انخفض CRP بشكل ملحوظ خلال 48 ساعة. ومع ذلك، تختلف الاستجابات الفردية ولا يمكن تقديم ضمان لسرعة أو درجة الاستجابة.
هل يمكن لعلاج MSC أن يحل محل الرعاية القياسية لالتهاب البنكرياس الحاد؟
لا. يُدرس علاج MSC كمساعد — وليس بديلاً — للرعاية القياسية المعمول بها: الإنعاش الوريدي بالسوائل، والتغذية المعوية، وإدارة الألم، ودعم الأعضاء. إنه إضافة بحثية قد تقلل من شدة المرض وتسرع التعافي، لكنه لا يحل محل الرعاية الداعمة على مستوى وحدة العناية المركزة.
ما هي تكلفة علاج MSC لالتهاب البنكرياس الحاد في تايلاند؟
في مركز VELAR في بانكوك، يتم تسعير علاج MSC المشتق من هلام وارتون للحالات الالتهابية الحادة وفقًا لعدد الخلايا وبروتوكول الإعطاء المحدد أثناء التقييم السريري. يتم تقديم عرض سعر مفصل بعد الاستشارة ومراجعة المؤشرات الحيوية. تقدم تايلاند مزايا تكلفة كبيرة مقارنة بالعلاج المكافئ في أمريكا الشمالية أو أوروبا أو أستراليا — عادة أقل بنسبة 40-60% — مع الحفاظ على معايير مختبر GMP قابلة للمقارنة أو متفوقة.
هل علاج MSC آمن للمرضى الذين يعانون من نخر بنكرياسي مصاب؟
هذا مجال بحث نشط. بينما تفرز MSC ببتيدات مضادة للميكروبات ولا تثبط الجهاز المناعي بنفس طريقة الكورتيكوستيرويدات، لم تتم دراسة سلامة تسريب MSC في سياق النخر المصاب المثبت بشكل محدد في تجارب عشوائية. الخطر النظري هو أن تعديل المناعة قد يضعف قدرة المضيف على احتواء العدوى. في VELAR، يتم تقييم كل حالة بشكل فردي — قد تكون MSC مناسبة بعد السيطرة على مصدر العدوى (التصريف أو استئصال النسيج الميت)، لكن القرار يتطلب مدخلات دقيقة من الأمراض المعدية والرعاية المركزة.
كم عدد تسريبات MSC المطلوبة لالتهاب البنكرياس الحاد؟
تستخدم معظم البروتوكولات قبل السريرية والسريرية تسريبًا وريديًا واحدًا خلال المرحلة الحادة (خلال 24-72 ساعة من بدء الأعراض)، رغم أن بعض الدراسات استكشفت الجرعات المتكررة على فترات 48-72 ساعة للمرضى الذين يعانون من خلل وظيفي عضوي مستمر. يتم تفريد البروتوكول بناءً على شدة المرض، والاستجابة للتسريب الأولي، واتجاهات المؤشرات الحيوية.
ما الذي يميز مركز VELAR في علاج MSC؟
يجمع VELAR بين عمليات المختبر المعتمدة ISO 9001:2015 و ISO/IEC 17025:2017 مع MSC المشتقة من هلام وارتون المزروعة تحت ظروف cGMP الكاملة. تخضع كل دفعة لتأكيد هوية ISCT (>95% CD73/CD90/CD105، <2% CD34/CD45/HLA-DR)، واختبار عقم متعدد الممرضات، وإطلاق جودة مستقل. يشمل الفريق الطبي أخصائيين ذوي خبرة في الرعاية المركزة والطب التجديدي، وتقع العيادة في وسط بانكوك مع دعم كامل متعدد اللغات للمرضى الدوليين.
المراجع
- Boxhoorn L, Voermans RP, Bouwense SA, et al. Acute pancreatitis. The Lancet. 2020;396(10252):726-734. doi:10.1016/S0140-6736(20)31310-6 ↩
- Lee PJ, Papachristou GI. New insights into acute pancreatitis. Nature Reviews Gastroenterology & Hepatology. 2019;16(8):479-496. doi:10.1038/s41575-019-0158-2 ↩
- Garg PK, Singh VP. Organ failure due to systemic injury in acute pancreatitis. Gastroenterology. 2019;156(7):2008-2023. doi:10.1053/j.gastro.2018.12.041 ↩
- Wang M, Yuan Q, Xie L. Mesenchymal stem cell-based immunomodulation: properties and clinical application. Stem Cells International. 2018;2018:3057624. doi:10.1155/2018/3057624 ↩
- Gao F, Chiu SM, Motan DA, et al. Mesenchymal stem cells and immunomodulation: current status and future prospects. Cell Death & Disease. 2016;7(1):e2062. doi:10.1038/cddis.2015.327 ↩
- Jung KH, Song SU, Yi T, et al. Human bone marrow-derived clonal mesenchymal stem cells inhibit inflammation and reduce acute pancreatitis in rats. Gastroenterology. 2011;140(3):998-1008. doi:10.1053/j.gastro.2010.11.047 ↩
- Tu XH, Song JX, Xue XJ, et al. Role of bone marrow-derived mesenchymal stem cells in a rat model of severe acute pancreatitis. World Journal of Gastroenterology. 2012;18(18):2270-2279. doi:10.3748/wjg.v18.i18.2270 ↩
- Yin G, Hu G, Wan R, et al. Role of bone marrow mesenchymal stem cells in L-arginine-induced acute pancreatitis. Stem Cells and Development. 2016;25(3):248-257. doi:10.1089/scd.2015.0241 ↩
- Tomkötter L, Erbes J, Trepte C, et al. The effects of pancreatic microcirculatory disturbances on histopathologic tissue damage in acute pancreatitis. Pancreas. 2016;45(2):248-253. doi:10.1097/MPA.0000000000000450 ↩
- Dombernowsky T, Kristensen MØ, Rysgaard S, Gluud LL, Novovic S. Acute lung injury and acute pancreatitis: a systematic review. Pancreatology. 2021;21(6):1139-1148. doi:10.1016/j.pan.2021.06.006 ↩
- Cui J, He M, She L, et al. Mesenchymal stem cells attenuate acute lung injury in severe acute pancreatitis via TSG-6-mediated immunomodulation. Stem Cell Research & Therapy. 2020;11:378. doi:10.1186/s13287-020-01892-4 ↩
- Qian D, Wei G, Xu C, et al. Bone marrow-derived mesenchymal stem cells promote repair of pancreatic injury via paracrine mechanisms. Journal of Cellular and Molecular Medicine. 2019;23(3):2120-2130. doi:10.1111/jcmm.14123 ↩
- Davies JE, Walker JT, Keating A. Concise review: Wharton's jelly: the rich, but enigmatic, source of mesenchymal stromal cells. Stem Cells Translational Medicine. 2017;6(7):1620-1630. doi:10.1002/sctm.16-0492 ↩
- Sun X, Hao H, Han Q, et al. Human umbilical cord-derived mesenchymal stem cells ameliorate acute pancreatitis via modulating macrophage polarization. Stem Cells. 2019;37(12):1554-1565. doi:10.1002/stem.3080 ↩
- Li L, Chen X, Wang WE, Zeng C. Safety and efficacy of umbilical cord mesenchymal stem cells in predicted severe acute pancreatitis: a Phase I trial. Cytotherapy. 2024;26(5):456-463. doi:10.1016/j.jcyt.2024.02.005 ↩
- Zhang Y, Liu J, Wang T, et al. Umbilical cord-derived mesenchymal stem cells for moderately severe acute pancreatitis: a randomized controlled trial. Stem Cells Translational Medicine. 2023;12(8):514-524. doi:10.1093/stcltm/szad042 ↩
- Rennert RC, Sorkin M, Garg RK, Gurtner GC. Stem cell recruitment after injury: lessons for regenerative medicine. Regenerative Medicine. 2012;7(6):833-850. doi:10.2217/rme.12.82 ↩