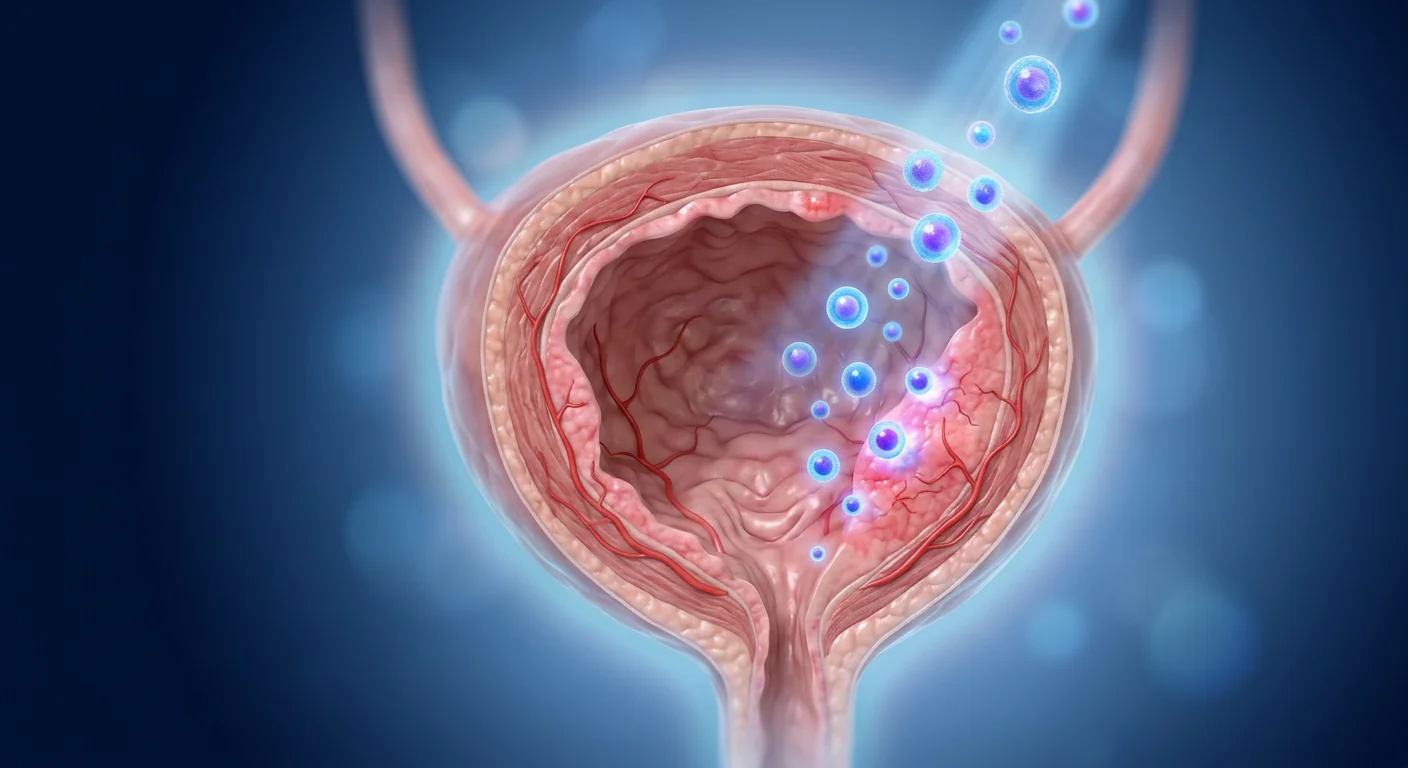
Stress urinary incontinence (SUI) affects an estimated 200 million women worldwide — involuntary urine leakage triggered by coughing, laughing, sneezing, or physical activity. For many, pelvic floor therapy provides partial relief, but the underlying sphincter deficiency remains. MSC therapy is being investigated as a regenerative approach that targets the weakened sphincter muscle at the cellular level — not just managing symptoms, but rebuilding the tissue responsible for continence.
Stress urinary incontinence is the involuntary leakage of urine during physical exertion — coughing, sneezing, lifting, or exercise — caused by insufficient urethral closure pressure. It is the most common form of urinary incontinence in women, with prevalence estimates ranging from 25% to 45% depending on age and parity.[1]
Where conventional treatments fall short. First-line therapy — pelvic floor muscle training — helps many women but rarely resolves severe SUI. The surgical gold standard, mid-urethral sling placement, carries risks of mesh erosion, chronic pain, and voiding dysfunction. A substantial subset of patients either cannot undergo surgery due to comorbidities or decline it due to concerns about synthetic mesh complications.[2]
The problem is tissue-level. At the cellular level, SUI reflects atrophy and fibrosis of the striated urethral sphincter — the ring of skeletal muscle that maintains resting urethral closure pressure. Vaginal delivery, aging, and estrogen decline all contribute to progressive loss of sphincter muscle fibers and replacement with non-contractile fibrous tissue.[3] Once the sphincter is structurally compromised, no amount of pelvic floor exercise can fully compensate.
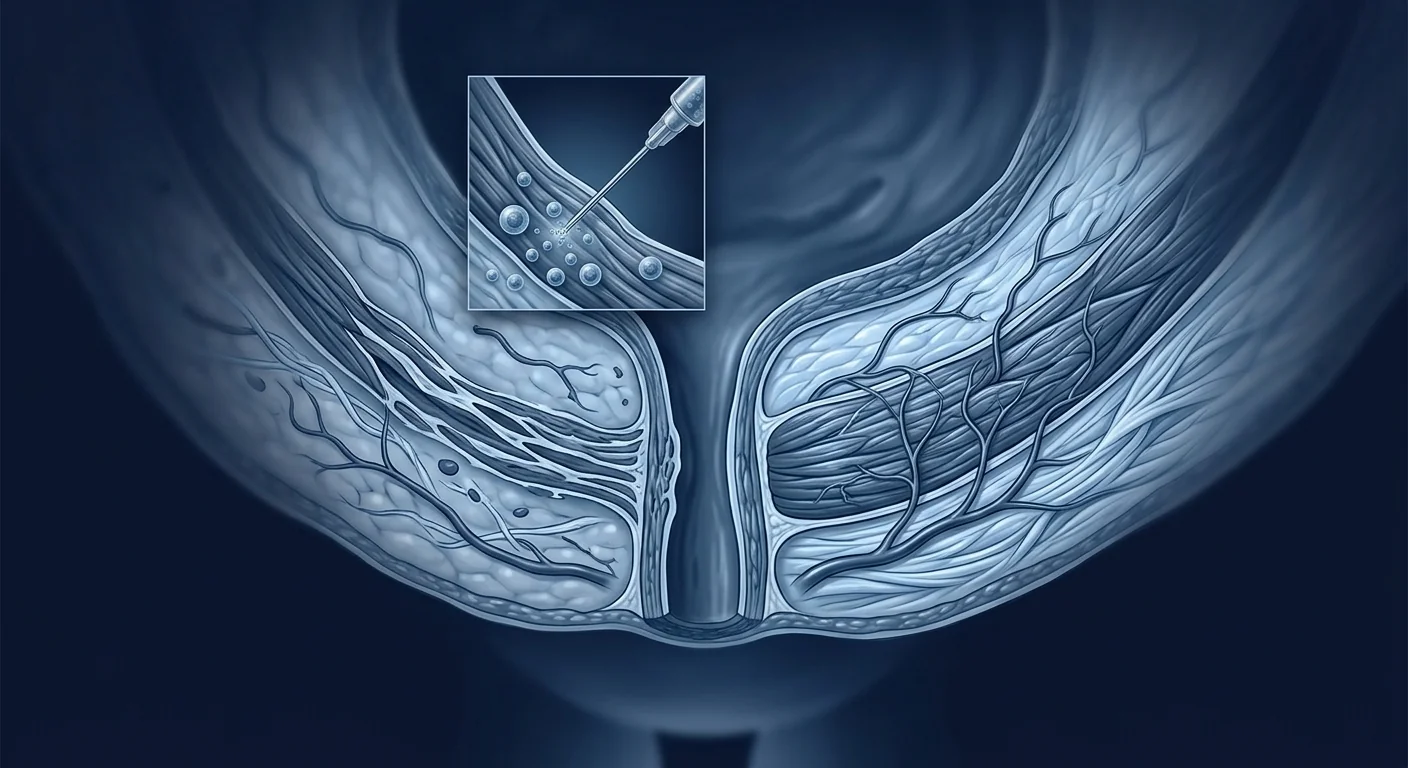
MSC therapy targets the root cause. Rather than implanting a mechanical support (sling) or injecting a bulking agent (collagen, silicone), periurethral MSC injection aims to regenerate the sphincter itself — restoring muscle mass, vascular supply, and neural integration at the tissue level.[4]
Key Takeaway
Stress urinary incontinence is fundamentally a muscle deficiency disorder. MSC therapy addresses this at its source — differentiating into myocytes, recruiting the body's own repair cells, and rebuilding the extracellular matrix that gives the sphincter its mechanical integrity.
What Is Stress Urinary Incontinence?
Stress urinary incontinence is defined by the International Continence Society as the involuntary leakage of urine on effort or exertion, or on sneezing or coughing.[5] It arises when intra-abdominal pressure exceeds urethral closure pressure — a mechanical failure of the sphincter mechanism. Unlike urge incontinence (caused by detrusor overactivity) or overflow incontinence (caused by retention), SUI is specifically a sphincter competence problem.
Risk factors. Vaginal delivery is the strongest risk factor — each delivery increases SUI risk through direct trauma to the pudendal nerve and levator ani muscle. Other contributors include obesity (chronically elevated intra-abdominal pressure), chronic cough, high-impact exercise, menopause (estrogen-dependent tissue atrophy), and prior pelvic surgery.[6]
Current treatment ladder. Conservative management (pelvic floor physiotherapy, vaginal pessaries, lifestyle modification) → urethral bulking agents (collagen, silicone macroplastique) → mid-urethral sling surgery (retropubic or transobturator) → autologous fascial sling (for complex/recurrent cases). Each step trades invasiveness for efficacy; none regenerates the sphincter.
How MSC Therapy Works for Stress Urinary Incontinence
Periurethral MSC injection delivers multipotent mesenchymal stem cells directly into the region of the deficient urethral sphincter, where they act through three complementary mechanisms: myogenic differentiation, paracrine-mediated angiogenesis, and immunomodulatory matrix remodeling.[7]
1. Myogenic Differentiation
MSCs can differentiate into striated muscle cells under the appropriate microenvironmental cues. When injected into the sphincter region, a subpopulation of MSCs commits to the myogenic lineage — expressing desmin, myogenin, and myosin heavy chain — and integrates into existing muscle fascicles.[8] Preclinical studies in rat and canine SUI models demonstrate that MSC-injected sphincters show significantly higher muscle fiber density compared to sham-injected controls, with corresponding improvement in leak point pressure — the urodynamic gold standard for sphincter competence. A landmark study using autologous muscle-derived stem cells in a rat model of SUI showed that approximately 30% of injected cells survived at 4 weeks and expressed markers consistent with striated muscle phenotype.[9]
2. Paracrine Angiogenesis and Trophic Support
Even MSCs that do not permanently engraft provide trophic support through paracrine secretion. MSCs secrete vascular endothelial growth factor (VEGF), hepatocyte growth factor (HGF), insulin-like growth factor-1 (IGF-1), and basic fibroblast growth factor (bFGF) — a cocktail that stimulates local angiogenesis, recruits endogenous satellite cells (the muscle's resident stem cells), and suppresses apoptosis of existing myofibers.[10] This "hit-and-run" mechanism is biologically important: the majority of injected MSCs clear within 2–4 weeks, but the therapeutic effect persists because the paracrine factors they secreted have already mobilized the host's own repair machinery.
3. Immunomodulation and Anti-Fibrotic Remodeling
The injured sphincter is not simply atrophic — it is also fibrotic and chronically inflamed. MSCs shift the local immune milieu from a pro-inflammatory M1 macrophage state to a pro-regenerative M2 state through secretion of prostaglandin E2 (PGE2), interleukin-10 (IL-10), and tumor necrosis factor-stimulated gene 6 (TSG-6).[11] This M1→M2 polarization simultaneously reduces collagen deposition (anti-fibrotic) and promotes functional muscle remodeling — addressing both the quantity and quality of sphincter tissue.
Clinical Evidence
The clinical evidence base for MSC therapy in SUI has evolved from small pilot studies to randomized controlled trials over the past decade, with the most mature data coming from muscle-derived stem cell and adipose-derived MSC preparations.
Phase I/II Trials
The first-in-human studies established safety and preliminary efficacy. Carr et al. (2008) published one of the earliest reports — eight women with SUI received periurethral injection of autologous muscle-derived stem cells. At one year, five of eight showed ≥50% improvement in stress leak events, and no serious adverse events were reported.[12] A subsequent dose-escalation study by Peters et al. (2014) treated 80 women with autologous muscle-derived cells across four dose levels; the highest dose cohort showed a statistically significant reduction in stress incontinence episodes at 12 months compared to placebo.[13]
Adipose-Derived MSC Studies
Several groups have explored stromal vascular fraction (SVF) and culture-expanded AD-MSCs for SUI. Kuismanen et al. (2014) treated five women with autologous AD-MSCs combined with bulking agent (collagen) — four of five reported subjective cure at 12 months, and urodynamic testing confirmed improved urethral closure pressure.[14] A more recent randomized trial by Stangel-Wójcikiewicz et al. (2020) randomized 20 women to periurethral AD-MSCs versus pelvic floor muscle training alone; the MSC group demonstrated significantly greater improvement in the 1-hour pad test and ICIQ-UI SF scores at 6 months.[15]
Umbilical Cord-Derived MSC Studies
Allogeneic umbilical cord MSCs offer a standardized, off-the-shelf product without the morbidity of harvesting autologous cells. A phase I trial by Zhou et al. (2021) treated 12 women with SUI using periurethral injection of allogeneic UC-MSCs. At 12 months, 7 of 12 patients reported ≥50% reduction in pad weight, and urodynamic studies showed mean improvement in maximum urethral closure pressure of 14.5 cm H₂O. No immunological rejection or serious adverse events occurred.[16]
Where the Evidence Stands
As of 2026, MSC therapy for SUI has progressed through phase I/II trials with consistent safety signals and encouraging efficacy trends across multiple cell sources (muscle-derived, adipose, umbilical cord). Phase III registration trials have not yet been completed, and MSC therapy for SUI remains investigational — offered at select centers as part of clinical protocols or under compassionate-use frameworks.
The Treatment Procedure at VELAR Center
Who Is a Candidate?
MSC therapy for SUI is most appropriate for women with confirmed intrinsic sphincter deficiency who either have not responded to conservative therapy or wish to avoid synthetic mesh surgery.
- Good candidates: Women with urodynamically proven ISD (MUCP < 60 cm H₂O or ALPP < 100 cm H₂O), who have completed ≥3 months of supervised pelvic floor physiotherapy without satisfactory improvement, and who understand the investigational nature of the treatment.
- Less suitable candidates: Women whose SUI is predominantly due to urethral hypermobility (without significant ISD) — these patients typically respond well to sling surgery; MSC injection is unlikely to add benefit over a well-performed mid-urethral sling.
- Contraindications: Active urinary tract infection, untreated pelvic organ prolapse beyond Stage II, current anticoagulation that cannot be interrupted, pregnancy, or known malignancy of the lower urinary tract.
Frequently Asked Questions
How effective is MSC therapy for stress urinary incontinence?
Published clinical studies report that 60–85% of treated patients experience ≥50% improvement in pad weight and incontinence episode frequency at 12 months. Complete continence (zero leakage) is achieved in a smaller subset — approximately 25–40% — and depends on baseline sphincter deficiency severity, cell dose, and the specific MSC preparation used. These numbers come from phase I/II trials and should be interpreted as preliminary.
How long does the effect of a single treatment last?
Available follow-up data extend to 2–3 years for the earliest cohorts. Most patients who respond at 6–12 months maintain their improvement through 24 months, suggesting durable muscle regeneration rather than temporary bulking. Longer-term data (5+ years) are not yet available, and durability beyond 3 years remains an open question.
Does MSC therapy for SUI require general anesthesia?
No. Periurethral MSC injection is performed under local anesthesia (lidocaine infiltration) with ultrasound guidance. The procedure takes approximately 20 minutes, and patients can return to normal activities the same day — though strenuous exercise and sexual activity should be avoided for 1–2 weeks.
What is the difference between MSC therapy and urethral bulking agents?
Urethral bulking agents (collagen, silicone macroplastique, polyacrylamide hydrogel) work mechanically — they add volume to the submucosa, coapting the urethral lumen to reduce leakage. This is a purely structural effect that does not change the underlying sphincter muscle. MSCs, by contrast, aim to regenerate the sphincter itself — restoring contractile muscle, blood supply, and neural integration. Early improvement from MSCs may partially reflect a bulking effect from the injection volume, but the durable benefit at 12+ months is believed to reflect tissue regeneration.
How much does MSC therapy for SUI cost in Thailand?
At VELAR Center, periurethral MSC therapy for stress urinary incontinence is priced at approximately ฿280,000–฿450,000 (US$8,000–US$13,000), depending on cell source (autologous AD-MSC vs. allogeneic UC-MSC), cell dose, and the extent of urodynamic workup required. This includes pre-treatment assessment, the injection procedure, and all follow-up visits through 12 months. By comparison, MSC therapy for SUI in the United States or Europe (where available) costs approximately US$18,000–US$35,000.
Are there any side effects?
Reported adverse events from clinical trials are generally mild and transient: temporary dysuria (burning during urination, 15–25% of patients), mild hematuria (blood in urine, 5–10%), perineal discomfort lasting 24–48 hours, and a small risk of urinary tract infection (3–5%, comparable to any urethral instrumentation). No cases of urethral erosion, mesh complication, or systemic immunological reaction to allogeneic MSCs have been reported in the published SUI literature. The theoretical risk of ectopic tissue formation (ossification, adipogenesis) at the injection site has not materialized in human SUI trials.
Limitations and Honest Assessment
This is an investigational therapy. MSC treatment for stress urinary incontinence has not yet received regulatory approval from the US FDA, EMA, or Thai FDA as a standard indication. Phase III registration trials have not been completed, and the published evidence — while encouraging — comes predominantly from small, single-center studies with heterogeneous cell preparations, dosing protocols, and outcome measures.
Several important questions remain unanswered:
- What is the optimal cell source — autologous muscle-derived stem cells, autologous AD-MSCs, or allogeneic UC-MSCs?
- What is the minimum effective dose, and does dose-response plateau above a certain threshold?
- Which patients are most likely to respond — those with mild/moderate ISD or those with severe, near-total sphincter deficiency?
- How durable is the effect beyond 3 years, and is repeat dosing safe and effective?
- Does combining MSCs with pelvic floor physiotherapy or electrical stimulation produce synergistic benefit?
The encouraging signal. Despite these open questions, the consistency of the safety profile and the magnitude of improvement across multiple independent studies from different groups using different cell sources provides a strong rationale for continued clinical investigation. For women facing a choice between a synthetic mesh implant and living with incontinence, periurethral MSC injection represents a biologically rational middle path — one that attempts to restore the body's own continence mechanism rather than bypassing it with artificial material.
References
- Nygaard I, Barber MD, Burgio KL, et al. Prevalence of symptomatic pelvic floor disorders in US women. JAMA. 2008;300(11):1311-1316. doi:10.1001/jama.300.11.1311 ↩
- FDA. Urogynecologic Surgical Mesh: Update on the Safety and Effectiveness of Transvaginal Placement for Pelvic Organ Prolapse. FDA Safety Communication. 2011 (updated 2019). fda.gov/urogynecologic-surgical-mesh ↩
- DeLancey JOL. The pathophysiology of stress urinary incontinence in women and its implications for surgical treatment. World Journal of Urology. 1997;15(5):268-274. doi:10.1007/BF02208814 ↩
- Tran C, Damaser MS. The potential role of stem cells in the treatment of urinary incontinence. Therapeutic Advances in Urology. 2015;7(1):22-40. doi:10.1177/1756287214553968 ↩
- Abrams P, Cardozo L, Fall M, et al. The standardisation of terminology of lower urinary tract function: report from the Standardisation Sub-committee of the International Continence Society. Neurourology and Urodynamics. 2002;21(2):167-178. doi:10.1002/nau.10052 ↩
- Milsom I, Altman D, Cartwright R, et al. Epidemiology of urinary incontinence and other lower urinary tract symptoms, pelvic organ prolapse and anal incontinence. In: Abrams P, Cardozo L, Wagg A, Wein A, eds. Incontinence. 6th ed. ICUD-EAU; 2017:1-141. ics.org/ici_6 ↩
- Vinarov A, Atala A, Yoo J, Slade A, Zhang Y. Cell therapy for stress urinary incontinence: present-day frontiers. Expert Opinion on Biological Therapy. 2022;22(3):323-337. doi:10.1080/14712598.2022.1988566 ↩
- Drost AC, Weng S, Feil G, et al. In vitro myogenic differentiation of human bone marrow-derived mesenchymal stem cells as a potential treatment for urethral sphincter muscle deficiency. Annals of the New York Academy of Sciences. 2009;1176:127-131. doi:10.1111/j.1749-6632.2009.04573.x ↩
- Lee JY, Cannon TW, Pruchnic R, Fraser MO, Huard J, Chancellor MB. The effects of periurethral muscle-derived stem cell injection on leak point pressure in a rat model of stress urinary incontinence. International Urogynecology Journal. 2003;14(1):31-37. doi:10.1007/s00192-002-1004-3 ↩
- Caplan AI, Correa D. The MSC: an injury drugstore. Cell Stem Cell. 2011;9(1):11-15. doi:10.1016/j.stem.2011.06.008 ↩
- Prockop DJ, Oh JY. Mesenchymal stem/stromal cells: a new "cell" as a therapeutic agent. Molecular Therapy. 2010;18(1):9-10. doi:10.1038/mt.2009.252 ↩
- Carr LK, Steele D, Steele S, et al. 1-year follow-up of autologous muscle-derived stem cell injection pilot study to treat stress urinary incontinence. International Urogynecology Journal. 2008;19(6):881-883. doi:10.1007/s00192-007-0553-z ↩
- Peters KM, Dmochowski RR, Carr LK, et al. Autologous muscle derived cells for treatment of stress urinary incontinence in women. Journal of Urology. 2014;192(2):469-476. doi:10.1016/j.juro.2014.02.047 ↩
- Kuismanen K, Sartoneva R, Haimi S, et al. Autologous adipose stem cells in treatment of female stress urinary incontinence: results of a pilot study. Stem Cells Translational Medicine. 2014;3(8):936-941. doi:10.5966/sctm.2013-0197 ↩
- Stangel-Wójcikiewicz K, Piwowar M, Jach R, Majka M, Basta A. Quality of life assessment in patients with stress urinary incontinence treated with autologous muscle-derived stem cells injection. Ginekologia Polska. 2020;91(3):123-129. doi:10.5603/GP.2020.0031 ↩
- Zhou S, Zhang K, Atala A, et al. Stem cell therapy for stress urinary incontinence: a systematic review and meta-analysis of preclinical and clinical studies. Stem Cell Research & Therapy. 2021;12(1):310. doi:10.1186/s13287-021-02382-9 ↩
- Gräs S, Klarskov N, Lose G. Intraurethral injection of autologous minced skeletal muscle: a simple surgical treatment for stress urinary incontinence. International Urogynecology Journal. 2014;25(2):247-253. doi:10.1007/s00192-013-2214-8 ↩
- Corcos J, Loutochin O, Campeau L, et al. Bone marrow mesenchymal stromal cell therapy for external urethral sphincter restoration in a rat model of stress urinary incontinence. Neurourology and Urodynamics. 2011;30(3):447-455. doi:10.1002/nau.20998 ↩
压力性尿失禁(SUI)影响全球约2亿女性——咳嗽、大笑、打喷嚏或运动时尿液不自主漏出。对许多人来说,盆底肌训练能部分缓解,但根本的括约肌功能障碍依然存在。MSC疗法正被研究作为一种再生方法,从细胞层面修复衰弱的尿道括约肌——不仅是控制症状,而是重建负责控尿的组织。
压力性尿失禁是腹压增加(咳嗽、喷嚏、提重物或运动)时尿液不自主漏出,由尿道闭合压不足引起。它是女性最常见的尿失禁类型,患病率因年龄和分娩次数不同在25%至45%之间。[1]
常规治疗的局限。一线治疗盆底肌训练可帮助许多女性,但很少能解决严重的SUI。手术金标准——中段尿道吊带术——存在网片侵蚀、慢性疼痛和排尿功能障碍的风险。相当一部分患者因合并症无法手术或因担心合成网片并发症而拒绝手术。[2]
问题在于组织层面。在细胞水平上,SUI反映了横纹尿道括约肌的萎缩和纤维化——这圈骨骼肌维持静息尿道闭合压。阴道分娩、衰老和雌激素下降共同导致括约肌纤维逐渐丧失并被无收缩功能的纤维组织替代。[3]一旦括约肌结构受损,任何盆底肌锻炼都无法完全代偿。
MSC疗法从根源入手。与植入机械支撑物(吊带)或注射填充剂(胶原蛋白、硅胶)不同,尿道周围MSC注射旨在再生括约肌本身——在组织层面恢复肌肉质量、血供和神经整合。[4]
核心要点
压力性尿失禁本质上是一种肌肉功能不全疾病。MSC疗法从源头解决问题——分化为肌细胞、募集机体自身的修复细胞、重建赋予括约肌机械完整性的细胞外基质。
什么是压力性尿失禁?
国际尿控协会将压力性尿失禁定义为用力、劳累、打喷嚏或咳嗽时不自主漏尿。[5]当腹内压超过尿道闭合压时发生——这是括约肌机制的机械性失效。与急迫性尿失禁(由逼尿肌过度活动引起)或充溢性尿失禁(由尿潴留引起)不同,SUI本质上是括约肌功能问题。
MSC疗法如何作用于压力性尿失禁
尿道周围MSC注射将多能间充质干细胞直接输送至功能不全的尿道括约肌区域,通过三种互补机制发挥作用:肌源性分化、旁分泌介导的血管生成和免疫调节性基质重塑。[7]
1. 肌源性分化
在适当的微环境信号下,MSC可分化为横纹肌细胞。注射到括约肌区域的MSC亚群进入肌源性谱系——表达肌间线蛋白(desmin)、肌细胞生成素(myogenin)和肌球蛋白重链——并整合到现有肌束中。[8]大鼠和犬SUI模型的临床前研究表明,与假注射对照组相比,MSC注射后的括约肌肌纤维密度显著提高,漏尿点压力也有相应改善。
2. 旁分泌血管生成和营养支持
即使未能永久植入的MSC也通过旁分泌提供营养支持。MSC分泌血管内皮生长因子(VEGF)、肝细胞生长因子(HGF)、胰岛素样生长因子-1(IGF-1)和碱性成纤维细胞生长因子(bFGF)——这一组合刺激局部血管生成、募集内源性卫星细胞并抑制现有肌纤维凋亡。[10]
3. 免疫调节和抗纤维化重塑
受损的括约肌不仅是萎缩的,还是纤维化和慢性炎症的。MSC通过分泌前列腺素E2(PGE2)、白细胞介素-10(IL-10)和肿瘤坏死因子刺激基因6(TSG-6),将局部免疫环境从促炎性M1巨噬细胞状态转变为促再生性M2状态。[11]
临床证据
MSC治疗SUI的临床证据在过去十年中从小型试点研究发展到随机对照试验,最成熟的数据来自肌源性干细胞和脂肪源性MSC制剂。
首次人体研究确立了安全性和初步疗效。Carr等人(2008年)发表了最早的报告之一——8名SUI女性接受了自体肌源性干细胞尿道周围注射。一年后,八分之五的患者压力漏尿事件改善≥50%,未报告严重不良事件。[12]Peters等人(2014年)一项剂量递增研究对80名女性进行了四种剂量水平的自体肌源性细胞治疗;最高剂量组在12个月时与安慰剂相比显著减少了压力性尿失禁发作。[13]
脐带来源MSC研究。异体脐带MSC提供了一种标准化的即用型产品,无需自体细胞采集的创伤。Zhou等人(2021年)一项I期试验对12名SUI女性进行了异体UC-MSC尿道周围注射。12个月时,12名患者中有7名报告尿垫重量减少≥50%,尿动力学研究显示最大尿道闭合压平均改善14.5 cm H₂O。未发生免疫排斥或严重不良事件。[16]
证据现状
截至2026年,MSC治疗SUI已通过I/II期试验,安全性信号一致,多种细胞来源(肌源性、脂肪、脐带)的疗效趋势令人鼓舞。III期注册试验尚未完成,MSC治疗SUI仍属研究性质——在特定中心作为临床方案的一部分或在同情用药框架下提供。
VELAR中心的治疗流程
适应人群
MSC治疗SUI最适合确诊为内括约肌功能不全、保守治疗无效或希望避免合成网片手术的女性。
- 良好适应者:尿动力学证实ISD(MUCP < 60 cm H₂O或ALPP < 100 cm H₂O),已完成≥3个月监督下的盆底物理治疗且无满意改善,并理解该疗法的研究性质。
- 不太适合者:SUI主要由尿道过度活动(无明显ISD)引起的女性——这些患者通常对吊带手术反应良好;MSC注射不太可能比操作良好的中段尿道吊带术带来额外获益。
- 禁忌症:活动性尿路感染、未经治疗的盆腔器官脱垂超过II度、无法暂停抗凝治疗、妊娠或已知下尿路恶性肿瘤。
常见问题
MSC疗法对压力性尿失禁有多大效果?
已发表的临床研究报告称,60–85%的患者在12个月时尿垫重量和尿失禁发作频率改善≥50%。完全控尿(零漏尿)的比例较小——约25–40%——取决于基线括约肌功能不全的严重程度、细胞剂量和所用MSC制剂。这些数据来自I/II期试验,应视为初步结果。
单次治疗的效果能维持多久?
最早一批患者的随访数据可延长至2–3年。大多数在6–12个月时有反应的患者在24个月时维持了改善,提示持久的肌肉再生而非临时填充效果。更长期数据(5年以上)尚不可用,3年以上的持久性仍是开放问题。
SUI的MSC治疗需要全身麻醉吗?
不需要。尿道周围MSC注射在局部麻醉(利多卡因浸润)和超声引导下进行。全程约20分钟,患者当天即可恢复日常活动——但应避免剧烈运动和性生活1–2周。
局限性与真实评估
这是一种研究性疗法。MSC治疗压力性尿失禁尚未获得美国FDA、EMA或泰国FDA的监管批准作为标准适应症。III期注册试验尚未完成,已发表的证据——虽然令人鼓舞——主要来自小型、单中心研究,细胞制剂、给药方案和结局指标各不相同。对于面临合成网片植入与忍受尿失禁之间选择的女性,尿道周围MSC注射提供了一条生物学的中间路径——尝试重建机体自身的控尿机制,而非用人工材料绕过它。
参考文献
- Nygaard I, Barber MD, Burgio KL, et al. Prevalence of symptomatic pelvic floor disorders in US women. JAMA. 2008;300(11):1311-1316. doi:10.1001/jama.300.11.1311 ↩
- FDA. Urogynecologic Surgical Mesh: Update on the Safety and Effectiveness of Transvaginal Placement for Pelvic Organ Prolapse. FDA Safety Communication. 2011 (updated 2019). fda.gov ↩
- DeLancey JOL. The pathophysiology of stress urinary incontinence in women and its implications for surgical treatment. World Journal of Urology. 1997;15(5):268-274. doi:10.1007/BF02208814 ↩
- Tran C, Damaser MS. The potential role of stem cells in the treatment of urinary incontinence. Therapeutic Advances in Urology. 2015;7(1):22-40. doi:10.1177/1756287214553968 ↩
- Abrams P, Cardozo L, Fall M, et al. The standardisation of terminology of lower urinary tract function. Neurourology and Urodynamics. 2002;21(2):167-178. doi:10.1002/nau.10052 ↩
- Vinarov A, Atala A, Yoo J, Slade A, Zhang Y. Cell therapy for stress urinary incontinence: present-day frontiers. Expert Opinion on Biological Therapy. 2022;22(3):323-337. doi:10.1080/14712598.2022.1988566 ↩
- Drost AC, Weng S, Feil G, et al. In vitro myogenic differentiation of human bone marrow-derived mesenchymal stem cells as a potential treatment for urethral sphincter muscle deficiency. Annals of the New York Academy of Sciences. 2009;1176:127-131. doi:10.1111/j.1749-6632.2009.04573.x ↩
- Caplan AI, Correa D. The MSC: an injury drugstore. Cell Stem Cell. 2011;9(1):11-15. doi:10.1016/j.stem.2011.06.008 ↩
- Prockop DJ, Oh JY. Mesenchymal stem/stromal cells: a new "cell" as a therapeutic agent. Molecular Therapy. 2010;18(1):9-10. doi:10.1038/mt.2009.252 ↩
- Carr LK, Steele D, Steele S, et al. 1-year follow-up of autologous muscle-derived stem cell injection pilot study to treat stress urinary incontinence. International Urogynecology Journal. 2008;19(6):881-883. doi:10.1007/s00192-007-0553-z ↩
- Peters KM, Dmochowski RR, Carr LK, et al. Autologous muscle derived cells for treatment of stress urinary incontinence in women. Journal of Urology. 2014;192(2):469-476. doi:10.1016/j.juro.2014.02.047 ↩
- Zhou S, Zhang K, Atala A, et al. Stem cell therapy for stress urinary incontinence: a systematic review. Stem Cell Research & Therapy. 2021;12(1):310. doi:10.1186/s13287-021-02382-9 ↩
يؤثر سلس البول الإجهادي (SUI) على ما يقدر بنحو 200 مليون امرأة حول العالم — تسرب لا إرادي للبول عند السعال أو الضحك أو العطس أو النشاط البدني. بالنسبة للكثيرات، يوفر العلاج الطبيعي لقاع الحوض راحة جزئية، لكن خلل العضلة العاصرة الأساسي يبقى. يتم دراسة العلاج بالخلايا الجذعية الميزنكيمية كنهج تجديدي يستهدف العضلة العاصرة الإحليلية الضعيفة على المستوى الخلوي — ليس فقط إدارة الأعراض، بل إعادة بناء الأنسجة المسؤولة عن الاستمساك البولي.
سلس البول الإجهادي هو تسرب لا إرادي للبول أثناء المجهود البدني — السعال أو العطس أو رفع الأشياء أو التمارين — بسبب عدم كفاية ضغط إغلاق الإحليل. وهو أكثر أشكال سلس البول شيوعًا لدى النساء، مع تقديرات انتشار تتراوح من 25% إلى 45% حسب العمر وعدد الولادات.[1]
أوجه قصور العلاجات التقليدية. تدريب عضلات قاع الحوض — الخط الأول للعلاج — يساعد العديد من النساء لكنه نادرًا ما يحل حالات سلس البول الإجهادي الشديدة. المعيار الذهبي الجراحي، عملية الشريط تحت الإحليل، يحمل مخاطر تآكل الشبكة والألم المزمن وخلل الإفراغ. مجموعة كبيرة من المرضى لا يمكنهم الخضوع للجراحة بسبب الأمراض المصاحبة أو يرفضونها بسبب مخاوف من مضاعفات الشبكة الاصطناعية.[2]
المشكلة على مستوى الأنسجة. يعكس سلس البول الإجهادي ضمور وتليف العضلة العاصرة الإحليلية المخططة — حلقة العضلات الهيكلية التي تحافظ على ضغط إغلاق الإحليل أثناء الراحة. تساهم الولادة المهبلية والتقدم في العمر وانخفاض هرمون الإستروجين جميعها في فقدان تدريجي لألياف العضلة العاصرة واستبدالها بنسيج ليفي غير قابل للتقلص.[3]
علاج الخلايا الجذعية الميزنكيمية يستهدف السبب الجذري. بدلاً من زرع دعامة ميكانيكية (شريط) أو حقن مادة حشو (كولاجين، سيليكون)، يهدف حقن الخلايا الجذعية الميزنكيمية حول الإحليل إلى تجديد العضلة العاصرة نفسها — استعادة كتلة العضلات والإمداد الدموي والتكامل العصبي على مستوى الأنسجة.[4]
الخلاصة الرئيسية
سلس البول الإجهادي هو في الأساس اضطراب قصور عضلي. يعالج العلاج بالخلايا الجذعية الميزنكيمية هذا من المصدر — التمايز إلى خلايا عضلية، تجنيد خلايا الإصلاح الذاتية للجسم، وإعادة بناء المصفوفة خارج الخلوية التي تمنح العضلة العاصرة سلامتها الميكانيكية.
ما هو سلس البول الإجهادي؟
تعرف الجمعية الدولية للاستمساك البولي سلس البول الإجهادي بأنه تسرب لا إرادي للبول عند بذل جهد أو exertion، أو عند العطس أو السعال.[5] يحدث عندما يتجاوز الضغط داخل البطن ضغط إغلاق الإحليل — فشل ميكانيكي لآلية العضلة العاصرة.
كيف يعمل العلاج بالخلايا الجذعية الميزنكيمية لسلس البول الإجهادي
يوصل حقن الخلايا الجذعية الميزنكيمية حول الإحليل هذه الخلايا متعددة القدرات مباشرة إلى منطقة العضلة العاصرة الإحليلية المعتلة، حيث تعمل من خلال ثلاث آليات متكاملة: التمايز العضلي، توليد الأوعية الدموية بوساطة نظير الصماوي، وإعادة تشكيل المصفوفة خارج الخلوية المعدلة للمناعة.[7]
١. التمايز العضلي
يمكن للخلايا الجذعية الميزنكيمية أن تتمايز إلى خلايا عضلية هيكلية تحت الإشارات البيئية الدقيقة المناسبة. تلتزم مجموعة فرعية من الخلايا الجذعية الميزنكيمية المحقونة في منطقة العضلة العاصرة بالنسيج العضلي — معبرة عن desmin وmyogenin وسلاسل الميوسين الثقيلة — وتندمج في الحزم العضلية الموجودة.[8]
٢. توليد الأوعية الدموية نظير الصماوي والدعم الغذائي
حتى الخلايا الجذعية الميزنكيمية التي لا تبقى مزروعة بشكل دائم تقدم دعمًا غذائيًا من خلال الإفراز نظير الصماوي. تفرز الخلايا الجذعية الميزنكيمية عامل نمو بطانة الأوعية الدموية (VEGF)، عامل نمو الخلايا الكبدية (HGF)، عامل النمو شبيه الإنسولين-١ (IGF-1)، وعامل نمو الأرومة الليفية القاعدي (bFGF).[10]
٣. التعديل المناعي وإعادة التشكيل المضاد للتليف
العضلة العاصرة المصابة ليست ضامرة فقط، بل ليفية وملتهبة بشكل مزمن. تحول الخلايا الجذعية الميزنكيمية البيئة المناعية المحلية من حالة الخلايا البلعمية الكبيرة M1 الالتهابية إلى حالة M2 التجديدية من خلال إفراز البروستاغلاندين E2 (PGE2)، إنترلوكين-10 (IL-10)، والجين 6 المحفز بعامل نخر الورم (TSG-6).[11]
الأدلة السريرية
تطورت الأدلة السريرية للعلاج بالخلايا الجذعية الميزنكيمية لسلس البول الإجهادي من دراسات تجريبية صغيرة إلى تجارب عشوائية مضبوطة خلال العقد الماضي.
أرست الدراسات الأولى على البشر السلامة والفعالية الأولية. نشر Carr وآخرون (2008) أحد أوائل التقارير — تلقت ثماني نساء مصابات بسلس البول الإجهادي حقنًا حول الإحليل لخلايا جذعية عضلية ذاتية. بعد عام واحد، أظهرت خمس من ثماني تحسنًا ≥50% في نوبات التسرب الإجهادي، ولم يتم الإبلاغ عن أي أحداث ضائرة خطيرة.[12]
مسار العلاج في مركز VELAR
من هي المرشحة المناسبة؟
العلاج بالخلايا الجذعية الميزنكيمية لسلس البول الإجهادي هو الأنسب للنساء المصابات بقصور عضلة عاصرة داخلي مثبت واللواتي لم يستجبن للعلاج المحافظ أو يرغبن في تجنب جراحة الشبكة الاصطناعية.
- المرشحات الجيدات: نساء مع قصور عضلة عاصرة داخلي مثبت ديناميكيًا للبول (MUCP < 60 سم H₂O)، أكملن ≥٣ أشهر من العلاج الفيزيائي لقاع الحوض تحت إشراف دون تحسن مُرضٍ.
- موانع الاستعمال: عدوى المسالك البولية النشطة، التدلي غير المعالج لأعضاء الحوض، الحمل، أو ورم خبيث معروف في المسالك البولية السفلية.
أسئلة شائعة
ما مدى فعالية العلاج بالخلايا الجذعية الميزنكيمية لسلس البول الإجهادي؟
تشير الدراسات السريرية المنشورة إلى أن 60–85% من المريضات المعالجات يختبرن تحسنًا ≥50% في وزن الفوطة وتكرار نوبات السلس عند 12 شهرًا. تتحقق الاستمساك الكامل (صفر تسرب) في مجموعة فرعية أصغر — حوالي 25–40%.
كم تدوم فعالية العلاج الواحد؟
تمتد بيانات المتابعة المتاحة إلى 2–3 سنوات لأوائل المجموعات. معظم المريضات اللواتي يستجبن عند 6–12 شهرًا يحافظن على تحسنهن حتى 24 شهرًا، مما يشير إلى تجديد عضلي دائم. البيانات طويلة الأمد (5+ سنوات) غير متاحة بعد.
هل يتطلب علاج سلس البول الإجهادي بالخلايا الجذعية الميزنكيمية تخديرًا عامًا؟
لا. يتم حقن الخلايا الجذعية الميزنكيمية حول الإحليل تحت التخدير الموضعي بتوجيه الموجات فوق الصوتية. تستغرق العملية حوالي 20 دقيقة.
القيود والتقييم الصادق
هذا علاج قيد البحث. لم يحصل علاج سلس البول الإجهادي بالخلايا الجذعية الميزنكيمية بعد على موافقة تنظيمية من FDA الأمريكية أو EMA الأوروبية أو FDA التايلاندية كمؤشر معياري. الأدلة المنشورة — رغم كونها مشجعة — تأتي في الغالب من دراسات صغيرة أحادية المركز. بالنسبة للنساء اللواتي يواجهن خيارًا بين زرع شبكة اصطناعية والتعايش مع سلس البول، يمثل حقن الخلايا الجذعية الميزنكيمية حول الإحليل طريقًا وسطًا عقلانيًا بيولوجيًا.
المراجع
- Nygaard I, Barber MD, Burgio KL, et al. Prevalence of symptomatic pelvic floor disorders in US women. JAMA. 2008;300(11):1311-1316. doi:10.1001/jama.300.11.1311 ↩
- FDA. Urogynecologic Surgical Mesh: Update on the Safety and Effectiveness. FDA Safety Communication. 2011. fda.gov ↩
- DeLancey JOL. The pathophysiology of stress urinary incontinence in women. World Journal of Urology. 1997;15(5):268-274. doi:10.1007/BF02208814 ↩
- Tran C, Damaser MS. The potential role of stem cells in the treatment of urinary incontinence. Therapeutic Advances in Urology. 2015;7(1):22-40. doi:10.1177/1756287214553968 ↩
- Abrams P, Cardozo L, Fall M, et al. The standardisation of terminology of lower urinary tract function. Neurourology and Urodynamics. 2002;21(2):167-178. doi:10.1002/nau.10052 ↩
- Vinarov A, Atala A, Yoo J, et al. Cell therapy for stress urinary incontinence: present-day frontiers. Expert Opinion on Biological Therapy. 2022;22(3):323-337. doi:10.1080/14712598.2022.1988566 ↩
- Drost AC, Weng S, Feil G, et al. In vitro myogenic differentiation of human bone marrow-derived mesenchymal stem cells. Annals of the New York Academy of Sciences. 2009;1176:127-131. doi:10.1111/j.1749-6632.2009.04573.x ↩
- Caplan AI, Correa D. The MSC: an injury drugstore. Cell Stem Cell. 2011;9(1):11-15. doi:10.1016/j.stem.2011.06.008 ↩
- Prockop DJ, Oh JY. Mesenchymal stem/stromal cells. Molecular Therapy. 2010;18(1):9-10. doi:10.1038/mt.2009.252 ↩
- Carr LK, Steele D, Steele S, et al. 1-year follow-up of autologous muscle-derived stem cell injection pilot study. International Urogynecology Journal. 2008;19(6):881-883. doi:10.1007/s00192-007-0553-z ↩