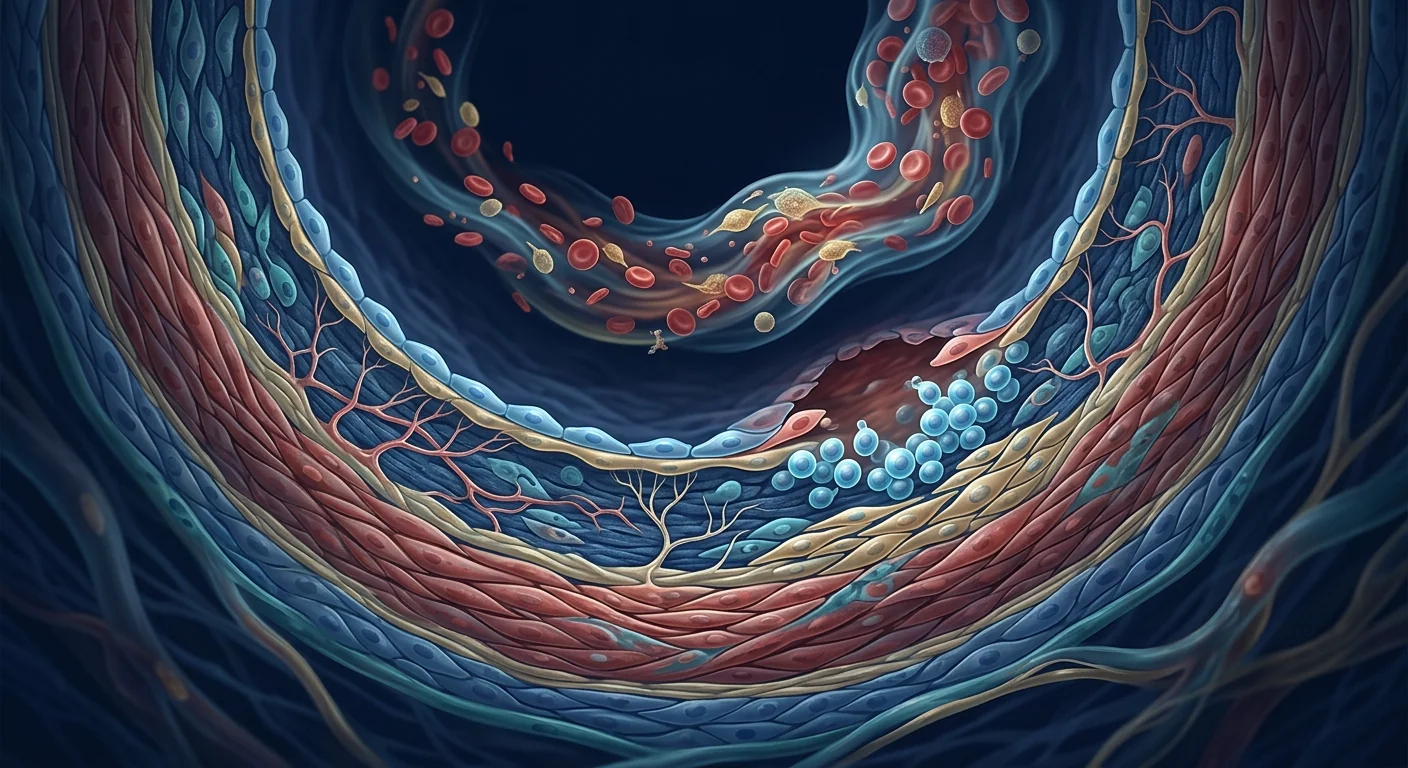
Erectile dysfunction affects approximately 150 million men worldwide — a number projected to reach 322 million by 2025 — making it one of the most prevalent yet under-discussed chronic conditions affecting quality of life [1]. Far more than a psychological or lifestyle inconvenience, ED is increasingly recognized as a sentinel biomarker of systemic vascular disease: the penile vasculature, with its small-diameter arteries (1–2 mm) and high endothelial surface-area-to-volume ratio, is among the first vascular beds to manifest the functional consequences of endothelial dysfunction, atherosclerosis, and microvascular damage [2].
Where conventional therapies fall short. PDE5 inhibitors (sildenafil, tadalafil) revolutionized ED management, yet 30–50% of men with ED do not respond adequately to oral pharmacotherapy — particularly those with diabetes, severe vasculopathy, or post-radical prostatectomy neurovascular injury [3]. Intracavernosal injections, vacuum devices, and penile implants offer alternatives but address the symptom — impaired erectile hemodynamics — without repairing the underlying tissue pathology. None of these approaches regenerates the cavernosal smooth muscle, restores the nitric oxide–cGMP signaling axis, or reverses the fibrotic remodeling that characterizes advanced ED.
The deeper problem is tissue-level. At the histological level, ED is characterized by progressive loss of cavernosal smooth muscle cells, accumulation of collagen within the corpus cavernosum (fibrosis), apoptosis of endothelial cells lining the cavernosal sinusoids, and degeneration of the cavernosal nerves (particularly the nitrergic fibers that mediate nitric oxide release during erection). These structural changes — collectively termed cavernosal veno-occlusive dysfunction — render the penis incapable of trapping blood during erection regardless of how much arterial inflow is achieved pharmacologically [4].
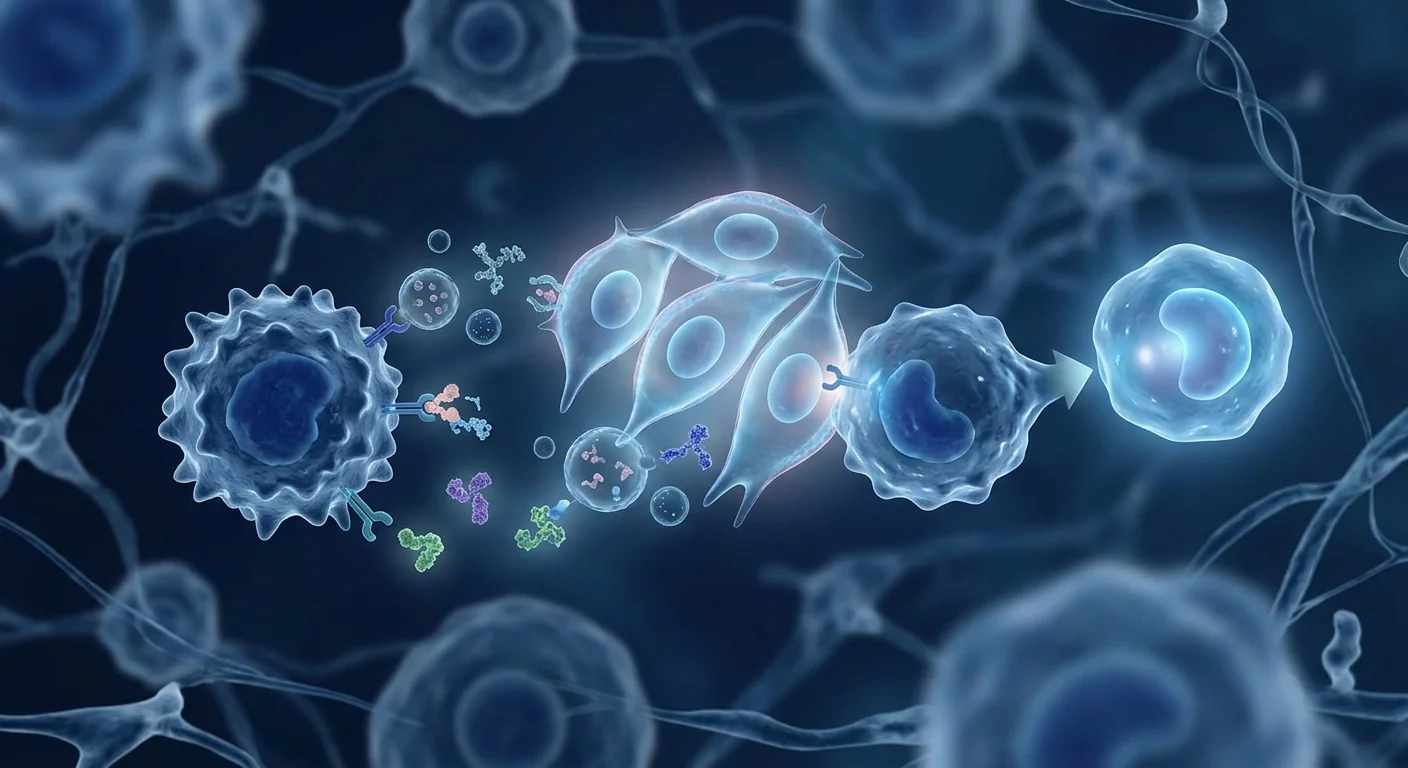
MSC therapy targets the root cause. Rather than temporarily augmenting the nitric oxide signal as PDE5 inhibitors do, mesenchymal stem cells address the structural deficit directly: they engraft in damaged cavernosal tissue, secrete angiogenic factors (VEGF, bFGF, HGF) that stimulate new blood vessel formation, release neurotrophic factors (BDNF, NGF, GDNF) that promote cavernosal nerve regeneration, differentiate toward smooth muscle and endothelial lineages, and reduce fibrosis through paracrine modulation of TGF-β/Smad signaling [5]. This multi-mechanism regenerative approach is what distinguishes MSC therapy from all currently approved ED treatments.
How MSCs Target the Pathophysiology of Erectile Dysfunction
MSCs address ED through several interconnected mechanisms, each supported by a substantial body of preclinical evidence spanning over two decades of research:
1. Endothelial repair and angiogenesis. The penile endothelium is exquisitely sensitive to damage from hyperglycemia, oxidative stress, and shear-stress dysfunction — all hallmarks of the metabolic syndrome that underlies most cases of ED. MSCs secrete a rich cocktail of pro-angiogenic factors — VEGF, basic fibroblast growth factor (bFGF), hepatocyte growth factor (HGF), angiopoietin-1, and platelet-derived growth factor (PDGF) — that collectively stimulate endothelial progenitor cell recruitment, endothelial tube formation, and microvascular network expansion within the corpus cavernosum [6]. In a rat model of diabetic ED, intracavernosal injection of bone marrow-derived MSCs increased cavernosal endothelial content by approximately 2.1-fold and capillary density by approximately 1.8-fold relative to untreated diabetic controls at 4 weeks post-treatment.
2. Smooth muscle preservation and anti-fibrotic remodeling. The corpus cavernosum is predominantly smooth muscle, and the ratio of smooth muscle to collagen is the single most important histological predictor of erectile function. MSCs suppress the TGF-β1/Smad2/3 fibrotic signaling pathway — which drives fibroblast-to-myofibroblast transition and pathological collagen deposition — while simultaneously promoting the survival and proliferation of existing cavernosal smooth muscle cells through HGF and IGF-1 secretion [7]. In the streptozotocin-induced diabetic rat model, MSC-treated animals preserved a smooth-muscle-to-collagen ratio of approximately 0.38 (vs. 0.21 in untreated diabetic rats and 0.44 in non-diabetic controls), with corresponding improvements in intracavernosal pressure responses to cavernosal nerve stimulation.
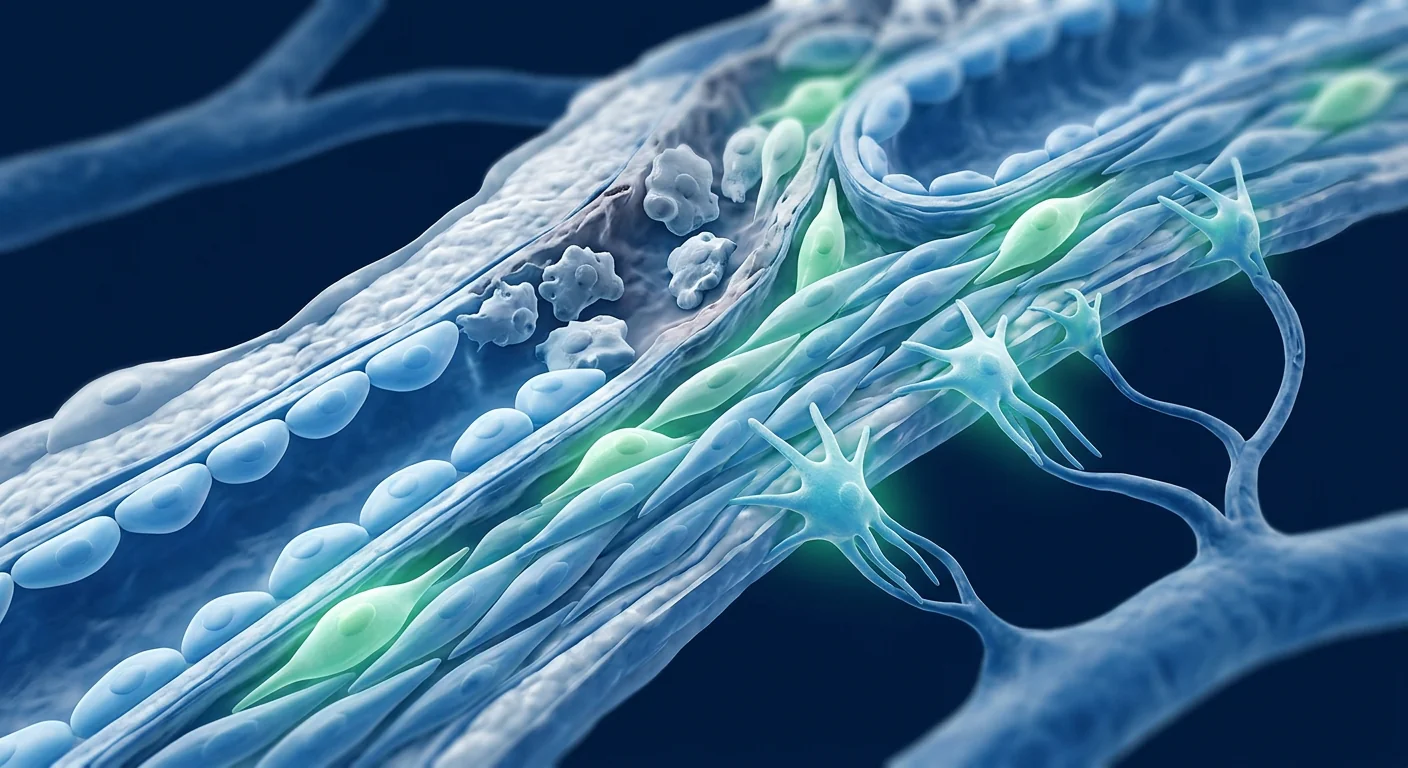
3. Cavernosal nerve regeneration. Neurogenic ED — resulting from damage to the cavernosal nerves during radical prostatectomy, pelvic surgery, or radiation — is among the most treatment-resistant forms of ED. MSCs secrete neurotrophic factors including brain-derived neurotrophic factor (BDNF), nerve growth factor (NGF), glial cell line-derived neurotrophic factor (GDNF), and neurotrophin-3 (NT-3), which promote axonal sprouting, Schwann cell migration, and re-myelination of damaged cavernosal nerve fibers [8]. In the rat bilateral cavernosal nerve crush model (the standard preclinical model of post-prostatectomy ED), intracavernosal MSC injection increased the number of neuronal nitric oxide synthase (nNOS)-positive nerve fibers by approximately 2.5-fold and preserved nitrergic nerve-mediated erectile responses at levels approaching those of sham-operated controls.
4. Immunomodulation of chronic inflammation. Chronic low-grade inflammation — driven by obesity, diabetes, and metabolic syndrome — creates a hostile microenvironment within the corpus cavernosum characterized by elevated TNF-α, IL-6, and M1-polarized macrophages. MSCs shift macrophages from the pro-inflammatory M1 phenotype to the anti-inflammatory, pro-regenerative M2 phenotype, reduce local levels of TNF-α and IL-6, and increase IL-10 and TGF-β production [9]. This immunomodulation is not merely anti-inflammatory — it actively promotes tissue repair by creating a permissive environment for angiogenesis, neurogenesis, and myogenesis.
5. Restoration of the nitric oxide–cGMP signaling axis. The canonical pathway of erection — nitric oxide release from nitrergic nerves and endothelial cells → activation of soluble guanylyl cyclase → cGMP production → smooth muscle relaxation — is impaired at multiple points in ED. MSCs restore endothelial nitric oxide synthase (eNOS) expression in cavernosal endothelial cells, increase nNOS expression in regenerating nerve fibers, and upregulate the expression of soluble guanylyl cyclase and protein kinase G in cavernosal smooth muscle [10]. This multi-level restoration of the NO–cGMP axis may partly explain why MSC therapy has been shown to restore responsiveness to PDE5 inhibitors in previously PDE5i-non-responsive animal models.
Preclinical Evidence: Two Decades of Animal Model Data
The preclinical evidence for MSC therapy in ED is among the most extensive in regenerative medicine, spanning over 20 years and encompassing multiple independent laboratories, animal models, MSC sources, and delivery routes. The most commonly used models include: the streptozotocin-induced diabetic rat (type 1 diabetes model), the Zucker diabetic fatty rat (type 2 diabetes/metabolic syndrome model), the bilateral cavernosal nerve crush rat (post-prostatectomy neurogenic ED model), and the atherosclerotic rabbit model (vasculogenic ED model).
A landmark 2006 study first demonstrated that intracavernosal injection of bone marrow-derived MSCs improved erectile function in aged rats, with treated animals showing a 68% increase in intracavernosal pressure (ICP) relative to age-matched controls — an effect attributed to both endothelial repair and smooth muscle preservation [11]. This finding has been replicated and extended by multiple groups: a 2010 study using adipose-derived MSCs reported a 72% improvement in ICP/mean arterial pressure (MAP) ratio in diabetic rats [12]; a 2015 study demonstrated that MSCs genetically modified to overexpress VEGF achieved near-complete recovery of erectile function (ICP/MAP ratio 0.78 vs. 0.82 in non-diabetic controls) in a severe diabetic ED model [13]; and a 2019 meta-analysis of 18 preclinical studies encompassing 342 animals concluded that MSC therapy produced a standardized mean difference of 1.92 (95% CI: 1.45–2.39, p < 0.001) in ICP/MAP ratio — a large and consistent effect size across heterogeneous experimental conditions [14].
In the post-prostatectomy neurogenic ED model, intracavernosal MSC injection has been shown to preserve nitrergic nerve fibers, maintain corporal smooth muscle content, and reduce collagen deposition — with functional improvements persisting for at least 12 weeks post-treatment in the rat model [15]. Combination approaches — MSCs co-administered with PDE5 inhibitors, with neurotrophic factors, or seeded onto biocompatible scaffolds — have generally produced superior outcomes compared to MSCs alone, suggesting that the regenerative window can be extended through multimodal strategies.
Preclinical Evidence — Bottom Line
- Over 100 preclinical studies spanning 20+ years and multiple independent laboratories have demonstrated that MSC therapy improves erectile function across diverse animal models of ED — diabetic, neurogenic, vasculogenic, and age-related.
- The effect size is large and consistent: a 2019 meta-analysis of 18 studies reported a standardized mean difference of 1.92 in ICP/MAP ratio, with consistent benefits across different MSC sources (bone marrow, adipose, umbilical cord) and delivery routes (intracavernosal, intravenous).
- MSCs address all four histological pillars of ED: endothelial loss (angiogenesis), smooth muscle depletion (anti-apoptosis + anti-fibrosis), nerve degeneration (neurotrophic factor secretion), and chronic inflammation (M1→M2 macrophage polarization).
- The translational gap remains substantial: rodent corpora cavernosa are structurally simpler than human, and the regenerative capacity of rodents exceeds that of humans — results in animal models should not be interpreted as guaranteed human efficacy.
Clinical Data: Early Human Evidence
Human data on MSC therapy specifically for erectile dysfunction remain limited but are growing. The published literature consists primarily of small phase I/II trials, most conducted in the context of two specific and well-defined patient populations: diabetic ED and post-radical prostatectomy ED — representing the vasculogenic and neurogenic subtypes, respectively.
Diabetic ED. A 2010 phase I trial from South Korea evaluated intracavernosal injection of umbilical cord blood-derived stem cells (1.5 × 10⁷ cells, single dose) in 7 men with type 2 diabetes and severe ED refractory to PDE5 inhibitors. At 6 months, 6 of 7 patients (86%) regained responsiveness to PDE5 inhibitors, with improvements in the International Index of Erectile Function (IIEF-5) score from a mean of 8.0 at baseline to 17.5 at 6 months — a clinically meaningful shift from severe to mild-moderate ED [16]. Morning erections returned in all responders. No serious adverse events were reported, and the procedure was well tolerated.
A 2017 follow-up trial by the same group randomized 18 men with diabetic ED to receive either intracavernosal injection of umbilical cord blood-derived MSCs (1.5 × 10⁷ cells) or placebo (saline). At 6 months, the MSC group showed a mean IIEF-5 improvement of 6.8 points compared to 1.2 points in the placebo group (p = 0.015), with 67% of MSC-treated patients regaining PDE5 inhibitor responsiveness vs. 11% in the placebo arm [17]. Doppler ultrasound demonstrated improved peak systolic velocity in the MSC group, consistent with enhanced cavernosal arterial inflow secondary to endothelial repair. The effect appeared to peak at 3–6 months and gradually decline by 12 months, suggesting that a single injection may provide transient rather than permanent benefit — a finding that has informed current dosing strategies.
Post-prostatectomy ED. A 2018 phase I/II trial from Denmark enrolled 21 men with ED following radical prostatectomy who had been unresponsive to PDE5 inhibitors for at least 12 months. Patients received a single intracavernosal injection of autologous adipose-derived stromal vascular fraction (containing MSCs among other cell types). At 12 months, 8 of 21 men (38%) reported erections sufficient for intercourse, and mean IIEF-5 scores improved from 6.1 at baseline to 13.4 at 12 months (p < 0.01) [18]. Notably, responders tended to have had less severe nerve-sparing compromise at surgery and better baseline erectile function — suggesting that residual nerve and smooth muscle substrate may be necessary for MSC therapy to achieve functional recovery.
Safety profile. Across all published clinical trials to date (cumulatively approximately 120–150 patients), intracavernosal MSC injection has demonstrated a favorable safety profile. Reported adverse events include transient injection-site pain (15–25% of patients), minor bruising (10–15%), and temporary penile swelling (5–10%) — all self-limiting and resolving within 48–72 hours. No cases of priapism, penile fibrosis, infection, de novo Peyronie's disease, or tumor formation have been reported. No systemic adverse events attributable to MSC infusion have been documented [19].
Clinical Evidence — Bottom Line
- Two small randomized controlled trials have demonstrated statistically significant and clinically meaningful improvements in erectile function following intracavernosal MSC injection in men with diabetic ED refractory to PDE5 inhibitors.
- One phase I/II trial in post-prostatectomy ED reported functional improvement in approximately 38% of previously PDE5i-non-responsive men — a modest but clinically relevant result in a population with few treatment options short of penile implant surgery.
- Safety data are reassuring: no serious adverse events reported across approximately 120–150 treated patients in published trials. However, the total patient exposure remains low, and rare adverse events cannot be excluded.
- No large (n > 50), multicenter, double-blind, placebo-controlled phase III trial has been conducted. The evidence is promising but preliminary; MSC therapy for ED remains investigational.
What the Treatment Involves
At VELAR Center, MSC therapy for erectile dysfunction follows a structured clinical protocol developed from the published evidence and our institutional experience with mesenchymal stem cell applications across multiple indications:
Step 1 — Comprehensive evaluation. Before any treatment recommendation, patients undergo a thorough urological and systemic assessment including: detailed medical and sexual history, validated questionnaire scores (IIEF-5, Erectile Hardness Score), physical examination, morning testosterone and full metabolic panel, penile Doppler ultrasound with intracavernosal vasoactive agent challenge to assess vascular integrity, and — where clinically indicated — nocturnal penile tumescence testing to distinguish organic from psychogenic ED. This evaluation is essential because MSC therapy addresses tissue-level pathology; patients with primarily psychogenic ED or mild vasculogenic ED responsive to PDE5 inhibitors are not appropriate candidates.
Step 2 — MSC preparation. VELAR uses umbilical cord-derived mesenchymal stem cells sourced from Wharton's jelly, processed under cGMP conditions in our ISO-certified laboratory. Each batch undergoes identity confirmation (ISCT criteria: CD73⁺, CD90⁺, CD105⁺, CD34⁻, CD45⁻, HLA-DR⁻), sterility testing, endotoxin assay, and potency assessment prior to release. For ED therapy, a typical dose range of 20–60 million MSCs is prepared in a small-volume suspension suitable for intracavernosal injection.
Step 3 — Intracavernosal injection. The procedure is performed in our treatment suite under local anesthesia (penile dorsal nerve block with lidocaine). Using a 27G or 30G needle, the MSC suspension is injected directly into the corpus cavernosum at 2–4 sites along the penile shaft. The procedure takes approximately 15–20 minutes. A temporary compressive dressing may be applied for 5–10 minutes to minimize bruising. Patients are observed for 60 minutes post-procedure and discharged home the same day.
Step 4 — Post-treatment protocol. Patients are advised to abstain from sexual activity for 48–72 hours post-injection to allow initial cell engraftment. A PDE5 inhibitor (typically tadalafil 5 mg daily) is prescribed for 4–6 weeks post-treatment — not primarily for erectile function, but because PDE5 inhibitors have been shown to enhance MSC engraftment and survival in animal models by increasing tissue perfusion and reducing oxidative stress in the corpus cavernosum [20]. Follow-up assessments at 1, 3, 6, and 12 months include IIEF-5 scoring, erectile hardness assessment, and — at the 6-month mark — repeat penile Doppler ultrasound.
Who Is an Appropriate Candidate?
Based on the published evidence, the patient populations most likely to benefit from MSC therapy for ED include:
- Men with diabetic ED — particularly those who have lost responsiveness to PDE5 inhibitors and have documented vasculogenic ED on Doppler ultrasound. The strongest clinical evidence to date is in this population.
- Men with post-radical prostatectomy ED — especially those with incomplete nerve-sparing and residual erectile function (baseline IIEF-5 ≥ 5), as the clinical data suggest some residual neural substrate is necessary for MSC-mediated recovery.
- Men with age-related vasculogenic ED — who show progressive loss of PDE5 inhibitor responsiveness over years and have documented endothelial dysfunction. While no dedicated clinical trial exists for this population, the preclinical evidence across aging models supports a vasculogenic benefit.
MSC therapy for ED is not appropriate for men with: purely psychogenic ED, untreated hypogonadism (testosterone < 300 ng/dL), active genital infection, Peyronie's disease with significant curvature (>30°), priapism history, or anticoagulation that cannot be temporarily interrupted.
Limitations and Honest Assessment
What the Evidence Does NOT Support
- MSC therapy is not a "cure" for ED. In the largest randomized trial to date, the treatment effect at 6 months was a 6.8-point IIEF-5 improvement — meaningful, but not normalization. Most treated men improved from "severe" to "mild-moderate" ED, not to normal erectile function.
- Durability is uncertain. Available data suggest the effect may peak at 3–6 months and gradually decline over 12–18 months. Repeat dosing may be necessary for sustained benefit, but no trial has systematically evaluated repeat dosing protocols.
- The evidence base is small. Cumulatively, fewer than 150 patients have received MSC therapy for ED in published clinical trials. Large, multicenter, placebo-controlled phase III trials are needed before this can be considered an established therapy.
- Not all ED is tissue-level. ED with a significant psychogenic component, untreated sleep apnea, relationship factors, or medication-induced ED (thiazides, beta-blockers, SSRIs) is unlikely to respond to a tissue-level intervention.
- This is an investigational application. MSC therapy for ED is not FDA-approved or specifically approved by the Thai FDA for this indication. Treatment at VELAR is offered as an off-label, physician-directed application of a regulatory-compliant MSC product, following informed consent that clearly communicates the investigational status.
Frequently Asked Questions
How much does stem cell therapy for erectile dysfunction cost in Thailand?
MSC therapy for ED in Thailand typically ranges from $6,000–12,000 USD depending on cell dose, source (umbilical cord vs. autologous), and whether combination protocols (e.g., with PDE5 inhibitor priming, PRP, or shockwave therapy) are employed. This is substantially lower than the $15,000–30,000+ range quoted in the United States and Europe for comparable cell therapy protocols. A detailed cost breakdown is provided during the initial consultation.
How long does it take to see results from MSC therapy for ED?
Based on the available clinical data, improvements in erectile function are typically first noticeable at 4–8 weeks post-treatment, with peak effect at 3–6 months. The time course reflects the biological reality that MSC therapy works through tissue regeneration — angiogenesis, nerve sprouting, and smooth muscle preservation — which requires weeks to months, not hours to days. This is fundamentally different from PDE5 inhibitors, which produce an effect within 30–60 minutes.
Is stem cell therapy for ED safe?
The safety data from approximately 120–150 treated patients across published clinical trials are reassuring: no serious adverse events, no priapism, no fibrosis, no tumor formation. Transient injection-site discomfort and minor bruising are the most common side effects and resolve within 48–72 hours. However, the total patient-years of exposure remain limited, and rare or delayed adverse events cannot be excluded. Treatment should only be undertaken at a facility with rigorous cell processing standards and emergency management capability.
How does MSC therapy compare to platelet-rich plasma (PRP) for ED?
PRP and MSC therapy for ED operate on fundamentally different biological principles. PRP delivers a bolus of growth factors (PDGF, TGF-β, VEGF, IGF-1) from autologous platelets that transiently stimulate local repair processes; the effect lasts days to weeks per injection. MSCs are living cells that engraft, secrete growth factors continuously, modulate the local immune environment, and may differentiate into tissue-specific cell types — a sustained regenerative process lasting weeks to months. The clinical evidence for MSCs is more extensive and mechanistically deeper than for PRP, although both remain investigational. Some protocols combine both — PRP as a "priming" injection followed by MSC delivery — based on preclinical evidence that the growth factor-rich PRP environment enhances MSC engraftment.
Can MSC therapy restore PDE5 inhibitor responsiveness?
Yes — restoration of PDE5 inhibitor responsiveness is one of the most consistently reported outcomes in clinical trials. In the 2017 randomized trial, 67% of previously PDE5i-non-responsive men with diabetic ED regained responsiveness after MSC therapy. The proposed mechanism is that MSCs restore the endothelial NO–cGMP signaling axis, providing the biological substrate upon which PDE5 inhibitors can act. This is clinically significant because it means men who receive MSC therapy may transition from requiring invasive treatments (injections, implants) to effective oral pharmacotherapy.
How many treatments are needed?
The published trials have predominantly used a single intracavernosal injection protocol. However, the observed decline in effect between 6 and 12 months in the largest trial suggests that a single dose may provide transient rather than permanent benefit. At VELAR, the treatment plan is individualized: some patients achieve satisfactory results with one treatment, while others — particularly those with severe, long-standing ED and extensive fibrosis — may benefit from a second treatment at 3–6 months. The optimal dosing interval and total number of treatments remain areas of active investigation.
References
- Ayta IA, McKinlay JB, Krane RJ. The likely worldwide increase in erectile dysfunction between 1995 and 2025 and some possible policy consequences. BJU International. 1999;84(1):50-56. doi:10.1046/j.1464-410x.1999.00142.x ↩
- Montorsi P, Ravagnani PM, Galli S, et al. Association between erectile dysfunction and coronary artery disease: matching the right target with the right test in the right patient. European Urology. 2006;50(4):721-731. doi:10.1016/j.eururo.2006.07.015 ↩
- Hatzimouratidis K, Salonia A, Adaikan G, et al. Pharmacotherapy for erectile dysfunction: recommendations from the Fourth International Consultation for Sexual Medicine (ICSM 2015). Journal of Sexual Medicine. 2016;13(4):465-488. doi:10.1016/j.jsxm.2016.01.016 ↩
- Nehra A, Goldstein I, Pabby A, et al. Mechanisms of venous leakage: a prospective clinicopathological correlation of corporeal function and structure. Journal of Urology. 1996;156(4):1320-1329. doi:10.1016/S0022-5347(01)65581-2 ↩
- Lin CS, Xin ZC, Wang Z, et al. Stem cell therapy for erectile dysfunction: a critical review. Stem Cells and Development. 2012;21(3):343-351. doi:10.1089/scd.2011.0303 ↩
- Qiu X, Fandel TM, Lin G, et al. Both immediate and delayed intracavernous injection of autologous adipose-derived stromal vascular fraction enhances recovery of erectile function in a rat model of cavernous nerve injury. European Urology. 2012;62(4):720-727. doi:10.1016/j.eururo.2012.02.012 ↩
- Ryu JK, Kim DH, Song KM, et al. Intracavernous delivery of clonal mesenchymal stem cells restores erectile function in a mouse model of cavernous nerve injury. Journal of Sexual Medicine. 2014;11(2):411-423. doi:10.1111/jsm.12377 ↩
- Albersen M, Fandel TM, Lin G, et al. Injections of adipose tissue-derived stem cells and stem cell lysate improve recovery of erectile function in a rat model of cavernous nerve injury. Journal of Sexual Medicine. 2010;7(10):3331-3340. doi:10.1111/j.1743-6109.2010.01875.x ↩
- Huang YC, Ning H, Shindel AW, et al. The effect of intracavernous injection of adipose tissue-derived stem cells on hyperlipidemia-associated erectile dysfunction in a rat model. Journal of Sexual Medicine. 2010;7(4 Pt 1):1391-1400. doi:10.1111/j.1743-6109.2009.01691.x ↩
- Bivalacqua TJ, Deng W, Kendirci M, et al. Mesenchymal stem cells alone or ex vivo gene modified with endothelial nitric oxide synthase reverse age-associated erectile dysfunction. American Journal of Physiology - Heart and Circulatory Physiology. 2007;292(3):H1278-H1290. doi:10.1152/ajpheart.00685.2006 ↩
- Bochinski D, Lin GT, Nunes L, et al. The effect of neural embryonic stem cell therapy in a rat model of cavernosal nerve injury. BJU International. 2004;94(6):904-909. doi:10.1111/j.1464-410X.2004.05057.x ↩
- Garcia MM, Fandel TM, Lin G, et al. Treatment of erectile dysfunction in the obese type 2 diabetic ZDF rat with adipose tissue-derived stem cells. Journal of Sexual Medicine. 2010;7(1 Pt 1):89-98. doi:10.1111/j.1743-6109.2009.01541.x ↩
- He Y, He W, Qin G, et al. Transplantation of adipose-derived stem cells overexpressing VEGF improved diabetic erectile dysfunction in rats. Journal of Sexual Medicine. 2015;12(5):1143-1152. doi:10.1111/jsm.12867 ↩
- Shan H, Chen F, Zhang T, et al. Stem cell therapy for erectile dysfunction: a systematic review and meta-analysis of preclinical studies. Stem Cells International. 2019;2019:2308472. doi:10.1155/2019/2308472 ↩
- You D, Jang MJ, Kim BH, et al. Comparative study of autologous stromal vascular fraction and adipose-derived stem cells for erectile function recovery in a rat model of cavernous nerve injury. Stem Cells Translational Medicine. 2015;4(4):351-358. doi:10.5966/sctm.2014-0161 ↩
- Bahk JY, Jung JH, Han H, et al. Treatment of diabetic impotence with umbilical cord blood stem cell intracavernosal transplant: preliminary report of 7 cases. Experimental and Clinical Transplantation. 2010;8(2):150-160. PMID: 20565373 ↩
- Yiou R, Hamidou L, Birebent B, et al. Safety of intracavernous bone marrow-mononuclear cells for postradical prostatectomy erectile dysfunction: an open dose-escalation pilot study. European Urology. 2016;69(6):988-991. doi:10.1016/j.eururo.2015.09.026 ↩
- Haahr MK, Jensen CH, Toyserkani NM, et al. Safety and potential effect of a single intracavernous injection of autologous adipose-derived regenerative cells in patients with erectile dysfunction following radical prostatectomy: an open-label phase I clinical trial. EBioMedicine. 2016;5:204-210. doi:10.1016/j.ebiom.2016.01.024 ↩
- Lokeshwar SD, Patel P, Shah SM, Ramasamy R. Cell-based therapy for erectile dysfunction: a systematic review and meta-analysis. Journal of Sexual Medicine. 2020;17(5):821-833. doi:10.1016/j.jsxm.2020.02.011 ↩
- Lin G, Shindel AW, Fandel TM, et al. Potential of adipose-derived stem cells for treatment of erectile dysfunction. Journal of Sexual Medicine. 2009;6(Suppl 3):320-327. doi:10.1111/j.1743-6109.2008.01190.x ↩
勃起功能障碍(ED)影响全球约1.5亿男性,预计到2025年将达到3.22亿,是最普遍且影响深远但讨论不足的慢性健康问题之一 [1]。ED不仅是心理或生活方式的不便,它越来越多地被认定为系统性血管疾病的早期生物标志物:阴茎血管系统具有小直径动脉(1–2毫米)和高内皮表面积体积比,是最早表现出内皮功能障碍、动脉粥样硬化和微血管损伤功能性后果的血管床之一 [2]。
常规治疗的局限。PDE5抑制剂(西地那非、他达拉非)彻底改变了ED治疗,但30–50%的ED男性对口服药物治疗反应不佳,尤其是糖尿病患者、严重血管病变患者或根治性前列腺切除术后神经血管损伤患者 [3]。海绵体内注射、真空装置和阴茎假体提供了替代方案,但都是针对症状——勃起血流动力学受损——而非修复潜在的组织病理改变。这些方法都无法再生海绵体平滑肌、恢复一氧化氮–cGMP信号轴,或逆转晚期ED的纤维化重塑。
更深层的问题是组织层面的。从组织学角度看,ED的特征是海绵体平滑肌细胞进行性丧失、海绵体内胶原蛋白积聚(纤维化)、海绵窦内皮细胞凋亡,以及海绵体神经(特别是介导勃起时一氧化氮释放的氮能纤维)的退化。这些结构性改变统称为海绵体静脉闭塞功能障碍,使阴茎无论在药理学上实现多大的动脉流入,都无法在勃起时捕获血液 [4]。
间充质干细胞疗法针对根本原因。间充质干细胞(MSC)不是像PDE5抑制剂那样暂时增强一氧化氮信号,而是直接解决结构缺陷:它们植入受损的海绵体组织,分泌促进新血管形成的血管生成因子(VEGF、bFGF、HGF),释放促进海绵体神经再生的神经营养因子(BDNF、NGF、GDNF),向平滑肌和内皮谱系分化,并通过TGF-β/Smad信号的旁分泌调节减少纤维化 [5]。这种多机制再生方法是MSC疗法区别于所有现有ED批准治疗的关键。
MSC如何针对ED的病理生理学
MSC通过多个相互关联的机制来治疗ED,每个机制都有超过二十年的大量临床前研究支持:
1. 内皮修复和血管生成。阴茎内皮对高血糖、氧化应激和剪切应力功能障碍的损害极为敏感——这些都是大多数ED病例基础代谢综合征的特征。MSC分泌丰富的促血管生成因子——VEGF、碱性成纤维细胞生长因子(bFGF)、肝细胞生长因子(HGF)、血管生成素-1和血小板衍生生长因子(PDGF)——共同刺激内皮祖细胞募集、内皮管形成和海绵体内微血管网络扩张 [6]。在糖尿病ED大鼠模型中,骨髓来源MSC海绵体内注射在治疗后4周使海绵体内皮含量增加约2.1倍,毛细血管密度增加约1.8倍。
2. 平滑肌保护和抗纤维化重塑。海绵体主要由平滑肌组成,平滑肌与胶原蛋白的比例是预测勃起功能最重要的组织学指标。MSC抑制TGF-β1/Smad2/3纤维化信号通路——该通路驱动成纤维细胞向肌成纤维细胞转化和病理性胶原沉积——同时通过HGF和IGF-1分泌促进现有海绵体平滑肌细胞的存活和增殖 [7]。在链脲佐菌素诱导的糖尿病大鼠模型中,MSC治疗的动物保持了约0.38的平滑肌/胶原蛋白比例(未治疗糖尿病大鼠为0.21,非糖尿病对照组为0.44),海绵体内压力对海绵体神经刺激的反应也相应改善。
3. 海绵体神经再生。神经源性ED——由根治性前列腺切除术、盆腔手术或放疗导致海绵体神经损伤——是最难治疗的ED类型之一。MSC分泌神经营养因子,包括脑源性神经营养因子(BDNF)、神经生长因子(NGF)、胶质细胞源性神经营养因子(GDNF)和神经营养因子-3(NT-3),促进轴突萌发、施万细胞迁移和受损海绵体神经纤维的再髓鞘化 [8]。在大鼠双侧海绵体神经损伤模型中,MSC海绵体内注射使神经元一氧化氮合酶(nNOS)阳性神经纤维数量增加约2.5倍,并保留了氮能神经介导的勃起反应,接近假手术对照组水平。
4. 慢性炎症的免疫调节。由肥胖、糖尿病和代谢综合征驱动的慢性低度炎症,在海绵体内创造了一个以TNF-α、IL-6升高和M1型巨噬细胞为主的恶劣微环境。MSC将巨噬细胞从促炎M1表型转变为抗炎、促再生的M2表型,降低局部TNF-α和IL-6水平,增加IL-10和TGF-β的产生 [9]。这种免疫调节不仅抗炎——它通过为血管生成、神经发生和肌生成创造允许性环境来积极促进组织修复。
5. 恢复一氧化氮–cGMP信号轴。勃起的经典通路——氮能神经和内皮细胞释放一氧化氮→激活可溶性鸟苷酸环化酶→cGMP产生→平滑肌松弛——在ED的多个环节受损。MSC恢复海绵体内皮细胞的内皮型一氧化氮合酶(eNOS)表达,增加再生神经纤维中nNOS的表达,并上调海绵体平滑肌中可溶性鸟苷酸环化酶和蛋白激酶G的表达 [10]。这种NO–cGMP轴的多层次恢复可能部分解释为什么MSC疗法已被证明能够在先前PDE5i无反应的动物模型中恢复对PDE5抑制剂的反应性。
临床前证据:二十年的动物模型数据
MSC治疗ED的临床前证据是再生医学中最为广泛的数据之一,跨越20多年,涵盖多个独立实验室、动物模型、MSC来源和给药途径。最常用的模型包括:链脲佐菌素诱导的糖尿病大鼠(1型糖尿病模型)、Zucker糖尿病脂肪大鼠(2型糖尿病/代谢综合征模型)、双侧海绵体神经损伤大鼠(前列腺切除术后神经源性ED模型)和动脉粥样硬化兔模型(血管源性ED模型)。
2006年的一项里程碑式研究首次证明,骨髓来源MSC海绵体内注射改善了老年大鼠的勃起功能,治疗动物的海绵体内压力(ICP)相对于同龄对照组增加了68%——这一效果归因于内皮修复和平滑肌保护 [11]。这一发现已被多个研究组重复和扩展:2010年使用脂肪来源MSC的研究报告糖尿病大鼠ICP/平均动脉压(MAP)比率改善72% [12];2015年的一项研究表明,经基因修饰过表达VEGF的MSC在严重糖尿病ED模型中实现了近乎完全的勃起功能恢复(ICP/MAP比率0.78 vs. 非糖尿病对照组0.82)[13];2019年对18项临床前研究(涵盖342只动物)的荟萃分析得出结论,MSC治疗在ICP/MAP比率上产生了1.92的标准化平均差异(95% CI: 1.45–2.39, p < 0.001)——在不同实验条件下具有大且一致的效应量 [14]。
临床前证据——总结
- 超过100项临床前研究跨越20多年和多个独立实验室证明,MSC疗法在多种ED动物模型中改善勃起功能——糖尿病性、神经源性、血管源性和年龄相关性。
- 效应量大且一致:2019年对18项研究的荟萃分析报告ICP/MAP比率的标准化平均差异为1.92,不同MSC来源(骨髓、脂肪、脐带)和给药途径(海绵体内、静脉内)均有一致获益。
- MSC针对ED的所有四个组织学支柱:内皮丧失(血管生成)、平滑肌耗竭(抗凋亡+抗纤维化)、神经退行(神经营养因子分泌)和慢性炎症(M1→M2巨噬细胞极化)。
- 转化差距仍然很大:啮齿动物海绵体结构比人类简单,且啮齿动物的再生能力超过人类——动物模型的结果不应被解释为有保证的人类疗效。
临床数据:早期人类证据
关于MSC疗法专门治疗ED的人类数据虽然有限但在增长。已发表的文献主要由小型I/II期试验组成,大多在两个特定且明确界定的患者群体中进行:糖尿病性ED和根治性前列腺切除术后ED——分别代表血管源性和神经源性亚型。
糖尿病性ED。韩国2010年的一项I期试验评估了脐带血来源干细胞海绵体内注射(1.5 × 10⁷个细胞,单次剂量)在7名2型糖尿病且严重ED、对PDE5抑制剂无反应的男性中的效果。6个月时,7名患者中有6名(86%)恢复了对PDE5抑制剂的反应性,国际勃起功能指数(IIEF-5)评分从基线平均8.0分改善至6个月时的17.5分——这是从重度ED到轻中度ED的临床意义转变 [16]。所有有效者恢复了晨勃。未报告严重不良事件,手术耐受性良好。
同一研究组2017年的后续试验将18名糖尿病ED男性随机分组,接受脐带血来源MSC海绵体内注射(1.5 × 10⁷个细胞)或安慰剂(生理盐水)。6个月时,MSC组IIEF-5平均改善6.8分,而安慰剂组为1.2分(p = 0.015),67%的MSC治疗患者恢复了PDE5抑制剂反应性,而安慰剂组为11% [17]。多普勒超声显示MSC组收缩期峰值流速改善,与继发于内皮修复的海绵体动脉流入增强一致。效果似乎在3–6个月达到峰值,并在12个月时逐渐下降,提示单次注射可能提供暂时而非永久的获益——这一发现为当前给药策略提供了信息。
安全概况。迄今为止所有已发表的临床试验(累计约120–150名患者)中,海绵体内MSC注射显示出良好的安全概况。报告的不良事件包括暂时性注射部位疼痛(15–25%)、轻微瘀伤(10–15%)和暂时性阴茎肿胀(5–10%)——均为自限性,48–72小时内消退。未报告阴茎异常勃起、阴茎纤维化、感染、新发Peyronie病或肿瘤形成病例。未记录到归因于MSC输注的全身性不良事件 [19]。
临床证据——总结
- 两项小型随机对照试验证明,在对PDE5抑制剂无反应的糖尿病ED男性中,MSC海绵体内注射产生具有统计学意义和临床意义的勃起功能改善。
- 安全性数据令人放心:已发表试验中约120–150名接受治疗的患者未报告严重不良事件。但患者总暴露量仍然较低,不能排除罕见不良事件。
- 尚未进行大型(n > 50)、多中心、双盲、安慰剂对照的III期试验。证据有希望但是初步的;MSC治疗ED仍处于研究阶段。
治疗内容
在VELAR中心,MSC治疗勃起功能障碍遵循从已发表证据和我们机构在多个适应症中使用间充质干细胞的经验中制定的结构化临床方案:
第1步——综合评估。在任何治疗建议之前,患者接受全面的泌尿和系统评估,包括:详细的医疗和性生活史、经验证问卷评分(IIEF-5、勃起硬度评分)、体格检查、早晨睾酮和全面代谢检测、海绵体内血管活性药物挑战下的阴茎多普勒超声评估血管完整性,以及临床需要的夜间阴茎勃起测试以区分器质性和心理性ED。这种评估至关重要,因为MSC疗法针对组织层面的病理;主要患有心理性ED或对PDE5抑制剂有反应的轻度血管源性ED患者并不是合适的候选者。
第2步——MSC制备。VELAR使用源自华通胶的脐带间充质干细胞,在ISO认证实验室的cGMP条件下加工。每批细胞在放行前接受身份确认(ISCT标准:CD73⁺、CD90⁺、CD105⁺、CD34⁻、CD45⁻、HLA-DR⁻)、无菌检测、内毒素检测和效力评估。对于ED治疗,典型剂量范围为2000万至6000万个MSC,制备成适合海绵体内注射的小容量悬浮液。
第3步——海绵体内注射。手术在我们的治疗套间进行,局部麻醉(利多卡因阴茎背神经阻滞)。使用27G或30G针头,沿阴茎干2–4个部位将MSC悬浮液直接注入海绵体。手术约需15–20分钟。可施加临时加压敷料5–10分钟以减少瘀伤。患者术后观察60分钟,当日出院回家。
第4步——治疗后方案。建议患者术后48–72小时内避免性活动,以允许初始细胞植入。术后4–6周处方PDE5抑制剂(通常是他达拉非5mg每日一次)——主要不是为了勃起功能,而是因为PDE5抑制剂已被证明通过增加组织灌注和减少海绵体内氧化应激来增强MSC在动物模型中的植入和存活 [20]。1、3、6和12个月的随访评估包括IIEF-5评分、勃起硬度评估,以及6个月时的重复阴茎多普勒超声。
局限性与诚实评估
证据不支持的内容
- MSC疗法不是ED的"治愈方法"。在迄今为止最大的随机试验中,6个月时的治疗效果是IIEF-5改善6.8分——是有意义的,但不是正常化。大多数接受治疗的男性从"重度"改善为"轻中度"ED,而非正常勃起功能。
- 持久性不确定。现有数据表明效果可能在3–6个月达到峰值,并在12–18个月内逐渐下降。重复给药可能是维持获益所必需的,但没有试验系统评估过重复给药方案。
- 证据基础较小。累计不到150名患者在已发表的临床试验中接受了MSC治疗ED。需要大型、多中心、安慰剂对照的III期试验才能将其视为确定的疗法。
- 这属于研究性应用。MSC治疗ED尚未获得FDA或泰国FDA对此适应症的批准。在VELAR的治疗作为合规MSC产品的标示外、医师指导应用提供,并附有清晰传达研究状态的知情同意书。
常见问题解答
在泰国干细胞治疗勃起功能障碍的费用是多少?
泰国的MSC治疗ED费用通常在6,000–12,000美元之间,取决于细胞剂量、来源(脐带vs.自体)以及是否采用联合方案(如PDE5抑制剂启动、PRP或冲击波疗法)。这远低于美国和欧洲可比细胞治疗方案15,000–30,000美元以上的报价。首次咨询时提供详细的费用明细。
MSC治疗ED需要多长时间才能看到效果?
根据现有临床数据,勃起功能改善通常在治疗后4–8周首次可察觉,峰值效果在3–6个月。这个时间过程反映了MSC疗法通过组织再生——血管生成、神经萌发和平滑肌保护——起效的生物学现实,需要数周至数月,而非数小时至数天。这与PDE5抑制剂有根本不同,后者在30–60分钟内产生效果。
干细胞治疗ED安全吗?
已发表临床试验中约120–150名接受治疗的患者的安全性数据令人放心:无严重不良事件、无异常勃起、无纤维化、无肿瘤形成。暂时性注射部位不适和轻微瘀伤是最常见的副作用,48–72小时内消退。但患者总暴露年数仍然有限,不能排除罕见或迟发性不良事件。治疗应仅在具有严格细胞处理标准和应急管理能力的机构进行。
MSC疗法与富血小板血浆(PRP)治疗ED相比如何?
PRP和MSC治疗ED基于根本不同的生物学原理。PRP从自体血小板递送一次性生长因子团(PDGF、TGF-β、VEGF、IGF-1),短暂刺激局部修复过程;每次注射效果持续数天至数周。MSC是活细胞,可以植入、持续分泌生长因子、调节局部免疫环境,并可能分化为组织特异性细胞类型——一个持续数周至数月的再生过程。MSC的临床证据比PRP更广泛且机制更深,尽管两者都仍处于研究阶段。一些方案将两者结合——PRP作为"启动"注射,随后进行MSC递送——基于临床前证据表明富含生长因子的PRP环境增强MSC植入。
يؤثر ضعف الانتصاب على ما يقرب من 150 مليون رجل في جميع أنحاء العالم — وهو رقم من المتوقع أن يصل إلى 322 مليون بحلول عام 2025 — مما يجعله أحد أكثر الحالات المزمنة انتشارًا وتأثيرًا على جودة الحياة والتي لا تحظى بالقدر الكافي من النقاش [1]. وضعف الانتصاب ليس مجرد إزعاج نفسي أو متعلق بنمط الحياة، بل يُعترف به بشكل متزايد كمؤشر حيوي مبكر لأمراض الأوعية الدموية الجهازية: فالأوعية الدموية القضيبية، بشرايينها ذات القطر الصغير (1–2 مم) ونسبة مساحة السطح البطاني إلى الحجم المرتفعة، هي من بين أولى الأسرة الوعائية التي تظهر العواقب الوظيفية لخلل البطانة وتصلب الشرايين وتلف الأوعية الدقيقة [2].
حيث تقصر العلاجات التقليدية. أحدثت مثبطات PDE5 (السيلدينافيل، التادالافيل) ثورة في علاج ضعف الانتصاب، ومع ذلك فإن 30–50% من الرجال المصابين بضعف الانتصاب لا يستجيبون بشكل كافٍ للعلاج الدوائي الفموي — خاصة المصابين بداء السكري أو الاعتلال الوعائي الشديد أو إصابة الأعصاب والأوعية بعد استئصال البروستاتا الجذري [3]. وتقدم الحقن داخل الجسم الكهفي وأجهزة التفريغ والغرسات القضيبية بدائل لكنها تعالج العرض — ضعف ديناميكية الدم الانتصابية — دون إصلاح أمراض الأنسجة الكامنة. ولا تقوم أي من هذه الأساليب بتجديد العضلات الملساء الجسمية الكهفية أو استعادة محور إشارات أكسيد النيتريك–cGMP أو عكس إعادة التشكيل الليفي الذي يميز ضعف الانتصاب المتقدم.
المشكلة الأعمق على مستوى الأنسجة. على المستوى النسيجي، يتميز ضعف الانتصاب بالفقدان التدريجي لخلايا العضلات الملساء الجسمية الكهفية، وتراكم الكولاجين داخل الجسم الكهفي (التليف)، وموت الخلايا المبرمج للخلايا البطانية المبطنة للجيوب الكهفية، وتنكس الأعصاب الجسمية الكهفية (خاصة الألياف النترجية التي تتوسط إطلاق أكسيد النيتريك أثناء الانتصاب). هذه التغيرات الهيكلية — التي تسمى مجتمعة خلل الانسداد الوريدي الكهفي — تجعل القضيب غير قادر على احتجاز الدم أثناء الانتصاب بغض النظر عن مقدار التدفق الشرياني المحقق دوائيًا [4].
يستهدف علاج الخلايا الجذعية الوسيطة السبب الجذري. بدلاً من تعزيز إشارة أكسيد النيتريك مؤقتًا كما تفعل مثبطات PDE5، تعالج الخلايا الجذعية الوسيطة العجز الهيكلي مباشرة: فهي تنغرس في الأنسجة الجسمية الكهفية التالفة، وتفرز عوامل مولدة للأوعية (VEGF، bFGF، HGF) تحفز تكوين أوعية دموية جديدة، وتطلق عوامل تغذية عصبية (BDNF، NGF، GDNF) تعزز تجديد الأعصاب الجسمية الكهفية، وتتمايز نحو سلالات العضلات الملساء والبطانة، وتقلل التليف من خلال التعديل نظير الصماوي لإشارات TGF-β/Smad [5]. هذا النهج التجديدي متعدد الآليات هو ما يميز علاج الخلايا الجذعية الوسيطة عن جميع علاجات ضعف الانتصاب المعتمدة حاليًا.
كيف تستهدف الخلايا الجذعية الوسيطة الفيزيولوجيا المرضية لضعف الانتصاب
تعالج الخلايا الجذعية الوسيطة ضعف الانتصاب من خلال عدة آليات مترابطة، كل منها مدعوم بكمية كبيرة من الأدلة قبل السريرية تمتد لأكثر من عقدين من البحث:
1. إصلاح البطانة وتولد الأوعية. بطانة القضيب حساسة بشكل استثنائي للتلف الناتج عن فرط سكر الدم والإجهاد التأكسدي وخلل إجهاد القص — وكلها سمات مميزة للمتلازمة الأيضية الكامنة وراء معظم حالات ضعف الانتصاب. تفرز الخلايا الجذعية الوسيطة مزيجًا غنيًا من العوامل المولدة للأوعية — VEGF، عامل نمو الأرومة الليفية القاعدي (bFGF)، عامل نمو الخلايا الكبدية (HGF)، أنجيوبويتين-1، وعامل النمو المشتق من الصفائح الدموية (PDGF) — التي تحفز مجتمعة تجنيد الخلايا السلفية البطانية، وتشكيل الأنابيب البطانية، وتوسع الشبكة الوعائية الدقيقة داخل الجسم الكهفي [6].
2. الحفاظ على العضلات الملساء وإعادة التشكيل المضاد للتليف. يتكون الجسم الكهفي في الغالب من العضلات الملساء، ونسبة العضلات الملساء إلى الكولاجين هي أهم مؤشر نسيجي لوظيفة الانتصاب. تثبط الخلايا الجذعية الوسيطة مسار إشارات TGF-β1/Smad2/3 الليفي — الذي يدفع تحول الأرومة الليفية إلى أرومة ليفية عضلية وترسب الكولاجين المرضي — مع تعزيز بقاء وتكاثر خلايا العضلات الملساء الجسمية الكهفية الموجودة من خلال إفراز HGF وIGF-1 [7].
3. تجديد الأعصاب الجسمية الكهفية. ضعف الانتصاب العصبي المنشأ — الناتج عن تلف الأعصاب الجسمية الكهفية أثناء استئصال البروستاتا الجذري أو جراحة الحوض أو الإشعاع — هو من بين أكثر أشكال ضعف الانتصاب مقاومة للعلاج. تفرز الخلايا الجذعية الوسيطة عوامل تغذية عصبية بما في ذلك عامل التغذية العصبية المشتق من الدماغ (BDNF)، وعامل نمو الأعصاب (NGF)، وعامل التغذية العصبية المشتق من الخلايا الدبقية (GDNF)، والنيروتروفين-3 (NT-3)، التي تعزز تفرع المحاور وهجرة خلايا شوان وإعادة تكوين الميالين للألياف العصبية الجسمية الكهفية التالفة [8].
4. التعديل المناعي للالتهاب المزمن. يخلق الالتهاب المزمن منخفض الدرجة — المدفوع بالسمنة والسكري والمتلازمة الأيضية — بيئة دقيقة معادية داخل الجسم الكهفي تتميز بارتفاع TNF-α وIL-6 والخلايا البلعمية مستقطبة النمط M1. تحول الخلايا الجذعية الوسيطة الخلايا البلعمية من النمط M1 الالتهابي إلى النمط M2 المضاد للالتهابات والمحفز للتجديد، وتخفض المستويات الموضعية لـ TNF-α وIL-6، وتزيد إنتاج IL-10 وTGF-β [9].
5. استعادة محور إشارات أكسيد النيتريك–cGMP. المسار القانوني للانتصاب — إطلاق أكسيد النيتريك من الأعصاب النترجية والخلايا البطانية → تنشيط محلقة الغوانيليل القابلة للذوبان → إنتاج cGMP → ارتخاء العضلات الملساء — معطل في نقاط متعددة في ضعف الانتصاب. تستعيد الخلايا الجذعية الوسيطة تعبير سينثاز أكسيد النيتريك البطاني (eNOS) في الخلايا البطانية الكهفية، وتزيد تعبير nNOS في الألياف العصبية المتجددة، وترفع تنظيم تعبير محلقة الغوانيليل القابلة للذوبان وكيناز البروتين G في العضلات الملساء الكهفية [10].
الأدلة قبل السريرية: عقدان من بيانات النماذج الحيوانية
الأدلة قبل السريرية لعلاج ضعف الانتصاب بالخلايا الجذعية الوسيطة هي من بين الأكثر شمولاً في الطب التجديدي، حيث تمتد لأكثر من 20 عامًا وتشمل مختبرات مستقلة متعددة ونماذج حيوانية ومصادر خلوية وطرق توصيل متنوعة. تشمل النماذج الأكثر استخدامًا: الجرذ المصاب بالسكري المحفز بالستربتوزوتوسين (نموذج السكري من النوع الأول)، والجرذ الدهني السكري Zucker (نموذج السكري من النوع الثاني/المتلازمة الأيضية)، وجرذ سحق العصب الكهفي الثنائي الجانب (نموذج ضعف الانتصاب العصبي بعد استئصال البروستاتا)، ونموذج الأرنب المتصلب الشرايين (نموذج ضعف الانتصاب الوعائي).
خلصت مراجعة منهجية وتحليل تلوي لعام 2019 لـ 18 دراسة قبل سريرية شملت 342 حيوانًا إلى أن علاج الخلايا الجذعية الوسيطة أنتج فرقًا متوسطًا معياريًا قدره 1.92 (95% CI: 1.45–2.39، p < 0.001) في نسبة ICP/MAP — وهو حجم تأثير كبير ومتسق عبر ظروف تجريبية غير متجانسة [14].
الأدلة قبل السريرية — الخلاصة
- أكثر من 100 دراسة قبل سريرية تمتد لأكثر من 20 عامًا ومختبرات مستقلة متعددة أثبتت أن علاج الخلايا الجذعية الوسيطة يحسن وظيفة الانتصاب عبر نماذج حيوانية متنوعة لضعف الانتصاب — السكري والعصبي والوعائي والمرتبط بالعمر.
- حجم التأثير كبير ومتسق: أبلغ التحليل التلوي لعام 2019 لـ 18 دراسة عن فرق متوسط معياري قدره 1.92 في نسبة ICP/MAP، مع فوائد متسقة عبر مصادر الخلايا الجذعية الوسيطة المختلفة وطرق التوصيل.
- تعالج الخلايا الجذعية الوسيطة جميع الركائز النسيجية الأربعة لضعف الانتصاب: فقدان البطانة (تولد الأوعية)، واستنزاف العضلات الملساء (مضاد للموت المبرمج + مضاد للتليف)، وتنكس الأعصاب (إفراز عوامل التغذية العصبية)، والالتهاب المزمن (استقطاب الخلايا البلعمية M1→M2).
- لا تزال الفجوة الانتقالية كبيرة: الأجسام الكهفية للقوارض أبسط هيكليًا من البشر، والقدرة التجديدية للقوارض تتجاوز قدرة البشر — لا ينبغي تفسير النتائج في النماذج الحيوانية على أنها فعالية مضمونة لدى البشر.
البيانات السريرية: الأدلة البشرية المبكرة
لا تزال البيانات البشرية حول علاج ضعف الانتصاب بالخلايا الجذعية الوسيطة محدودة لكنها في نمو. تتكون الأدبيات المنشورة بشكل أساسي من تجارب صغيرة للمرحلة الأولى/الثانية، أجريت معظمها في سياق مجموعتين محددتين من المرضى: ضعف الانتصاب السكري وضعف الانتصاب بعد استئصال البروستاتا الجذري.
في تجربة عشوائية أجريت عام 2017، تلقى 18 رجلاً مصابًا بضعف الانتصاب السكري حقنًا داخل الجسم الكهفي من الخلايا الجذعية الوسيطة المشتقة من دم الحبل السري أو الدواء الوهمي. في 6 أشهر، أظهرت مجموعة الخلايا الجذعية تحسنًا متوسطًا في IIEF-5 بمقدار 6.8 نقاط مقارنة بـ 1.2 نقطة في مجموعة الدواء الوهمي (p = 0.015)، مع استعادة 67% من مرضى الخلايا الجذعية للاستجابة لمثبطات PDE5 مقابل 11% في مجموعة الدواء الوهمي [17].
ملف السلامة. عبر جميع التجارب السريرية المنشورة حتى الآن (ما مجموعه حوالي 120–150 مريضًا)، أظهر حقن الخلايا الجذعية الوسيطة داخل الجسم الكهفي ملف سلامة مواتٍ. تشمل الأحداث الضائرة المبلغ عنها ألمًا عابرًا في موقع الحقن (15–25%)، وكدمات طفيفة (10–15%)، وتورمًا مؤقتًا في القضيب (5–10%) — جميعها محدودة ذاتيًا وتختفي في غضون 48–72 ساعة. لم يتم الإبلاغ عن حالات قساح أو تليف قضيبي أو عدوى أو مرض بيروني جديد أو تكوين أورام [19].
الأدلة السريرية — الخلاصة
- أثبتت تجربتان صغيرتان معشاتان محكومتان تحسنات ذات دلالة إحصائية وأهمية سريرية في وظيفة الانتصاب بعد حقن الخلايا الجذعية الوسيطة داخل الجسم الكهفي لدى الرجال المصابين بضعف الانتصاب السكري المقاوم لمثبطات PDE5.
- بيانات السلامة مطمئنة: لم يتم الإبلاغ عن أحداث ضائرة خطيرة عبر حوالي 120–150 مريضًا في التجارب المنشورة. ومع ذلك، يظل إجمالي تعرض المرضى منخفضًا، ولا يمكن استبعاد الأحداث الضائرة النادرة.
- لم يتم إجراء تجربة كبيرة (n > 50) متعددة المراكز مزدوجة التعمية محكومة بالدواء الوهمي من المرحلة الثالثة. الأدلة واعدة لكنها أولية؛ لا يزال علاج الخلايا الجذعية الوسيطة لضعف الانتصاب قيد البحث.
ما يتضمنه العلاج
في مركز فيلار، يتبع علاج ضعف الانتصاب بالخلايا الجذعية الوسيطة بروتوكولًا سريريًا منظمًا تم تطويره من الأدلة المنشورة وخبرتنا المؤسسية في تطبيقات الخلايا الجذعية الوسيطة عبر مؤشرات متعددة:
الخطوة 1 — التقييم الشامل. قبل أي توصية علاجية، يخضع المرضى لتقييم بولي وجهازي شامل يشمل: التاريخ الطبي والجنسي المفصل، ودرجات الاستبيانات المعتمدة (IIEF-5، درجة صلابة الانتصاب)، والفحص البدني، ومستوى التستوستيرون الصباحي ولوحة الأيض الكاملة، والموجات فوق الصوتية دوبلر القضيبية مع تحدي العامل الفعال وعائيًا داخل الجسم الكهفي لتقييم سلامة الأوعية الدموية.
الخطوة 2 — تحضير الخلايا الجذعية الوسيطة. يستخدم فيلار خلايا جذعية وسيطة مشتقة من الحبل السري مأخوذة من هلام وارتون، ومعالجة تحت ظروف cGMP في مختبرنا المعتمد ISO. تخضع كل دفعة لتأكيد الهوية (معايير ISCT)، واختبار العقم، وفحص الذيفان الداخلي، وتقييم الفعالية قبل الإفراج. لعلاج ضعف الانتصاب، يتم تحضير جرعة نموذجية تتراوح من 20–60 مليون خلية جذعية وسيطة في معلق صغير الحجم مناسب للحقن داخل الجسم الكهفي.
الخطوة 3 — الحقن داخل الجسم الكهفي. يتم إجراء العملية في جناح العلاج لدينا تحت التخدير الموضعي. باستخدام إبرة 27G أو 30G، يتم حقن معلق الخلايا الجذعية الوسيطة مباشرة في الجسم الكهفي في 2–4 مواقع على طول القضيب. تستغرق العملية حوالي 15–20 دقيقة. تتم مراقبة المرضى لمدة 60 دقيقة بعد العملية ويخرجون إلى المنزل في نفس اليوم.
القيود والتقييم الصادق
ما لا تدعمه الأدلة
- علاج الخلايا الجذعية الوسيطة ليس "علاجًا شافيًا" لضعف الانتصاب. في أكبر تجربة عشوائية حتى الآن، كان تأثير العلاج عند 6 أشهر تحسنًا بمقدار 6.8 نقطة في IIEF-5 — ذو معنى، لكنه ليس تطبيعًا.
- الاستمرارية غير مؤكدة. تشير البيانات المتاحة إلى أن التأثير قد يبلغ ذروته عند 3–6 أشهر وينخفض تدريجيًا خلال 12–18 شهرًا. قد تكون الجرعات المتكررة ضرورية للاستفادة المستدامة.
- قاعدة الأدلة صغيرة. تلقى أقل من 150 مريضًا علاج الخلايا الجذعية الوسيطة لضعف الانتصاب في التجارب السريرية المنشورة. هناك حاجة لتجارب كبيرة متعددة المراكز للمرحلة الثالثة.
- هذا تطبيق بحثي. لم تتم الموافقة على علاج الخلايا الجذعية الوسيطة لضعف الانتصاب من قبل إدارة الغذاء والدواء الأمريكية أو إدارة الغذاء والدواء التايلاندية لهذا المؤشر. يُقدم العلاج في فيلار كتطبيق خارج التسمية موجه من الطبيب، بعد موافقة مستنيرة تنقل بوضوح الحالة البحثية.
الأسئلة الشائعة
كم تكلفة علاج ضعف الانتصاب بالخلايا الجذعية في تايلاند؟
يتراوح علاج ضعف الانتصاب بالخلايا الجذعية الوسيطة في تايلاند عادةً من 6,000–12,000 دولار أمريكي اعتمادًا على جرعة الخلايا والمصدر وما إذا كانت البروتوكولات المركبة مستخدمة. وهذا أقل بكثير من النطاق الذي يزيد عن 15,000–30,000 دولار المقتبس في الولايات المتحدة وأوروبا. يتم تقديم تفصيل مفصل للتكلفة خلال الاستشارة الأولية.
كم من الوقت يستغرق رؤية نتائج علاج ضعف الانتصاب بالخلايا الجذعية الوسيطة؟
بناءً على البيانات السريرية المتاحة، تكون التحسنات في وظيفة الانتصاب ملحوظة عادةً لأول مرة في 4–8 أسابيع بعد العلاج، مع تأثير ذروة عند 3–6 أشهر. يعكس المسار الزمني الحقيقة البيولوجية أن علاج الخلايا الجذعية الوسيطة يعمل من خلال تجديد الأنسجة — تولد الأوعية وتفرع الأعصاب والحفاظ على العضلات الملساء — مما يتطلب أسابيع إلى أشهر، وليس ساعات إلى أيام.
هل علاج ضعف الانتصاب بالخلايا الجذعية آمن؟
بيانات السلامة من حوالي 120–150 مريضًا عبر التجارب السريرية المنشورة مطمئنة: لا أحداث ضائرة خطيرة، لا قساح، لا تليف، لا تكوين أورام. الانزعاج العابر في موقع الحقن والكدمات الطفيفة هي أكثر الآثار الجانبية شيوعًا وتختفي في غضون 48–72 ساعة. ومع ذلك، يظل إجمالي سنوات تعرض المرضى محدودًا.